Glutathione, Aging, and the GlyNAC Framework
Glutathione deficiency is one of the most reliably documented hallmarks of biological aging. Population studies show that intracellular GSH in red blood cells falls roughly 50% between ages 30 and 80, with parallel declines in mitochondrial function, oxidative stress buffering, and inflammatory regulation. Rajagopal Sekhar and colleagues at Baylor College of Medicine have spent two decades demonstrating that this decline is not an inevitable consequence of cellular wear-and-tear but a targetable deficiency driven by reduced precursor availability — specifically glycine and cysteine. Their 2021 randomized trial of "GlyNAC" supplementation (glycine 100 mg/kg + NAC 100 mg/kg daily) in adults aged 70-80 restored red cell glutathione to youthful levels and produced clinically meaningful improvements across mitochondrial function, inflammation, insulin resistance, grip strength, gait speed, body composition, and cognitive performance. GlyNAC reframes aging-associated GSH deficiency as a clinically actionable target rather than an unavoidable consequence of aging.
Interactive Visualization Free Radicals & Your Antioxidant Network Follow one superoxide radical down the whole relay — SOD, catalase, glutathione, vitamin E, vitamin C, NADPH — then release free iron and watch a membrane tear itself apart. Launch →
Table of Contents
- The 50% GSH Decline of Aging
- Why Glutathione Falls With Age
- Hallmarks of Aging & the GSH Connection
- The Sekhar Baylor Program
- The 2021 GlyNAC Trial in Detail
- Mechanism — Why GlyNAC Works
- Earlier GlyNAC Trials (HIV, T2D, NAFLD)
- Practical GlyNAC Protocols
- Lab Monitoring & Response Expectations
- Cautions Specific to Older Adults
- Key Research Papers
- Connections
- Featured Videos
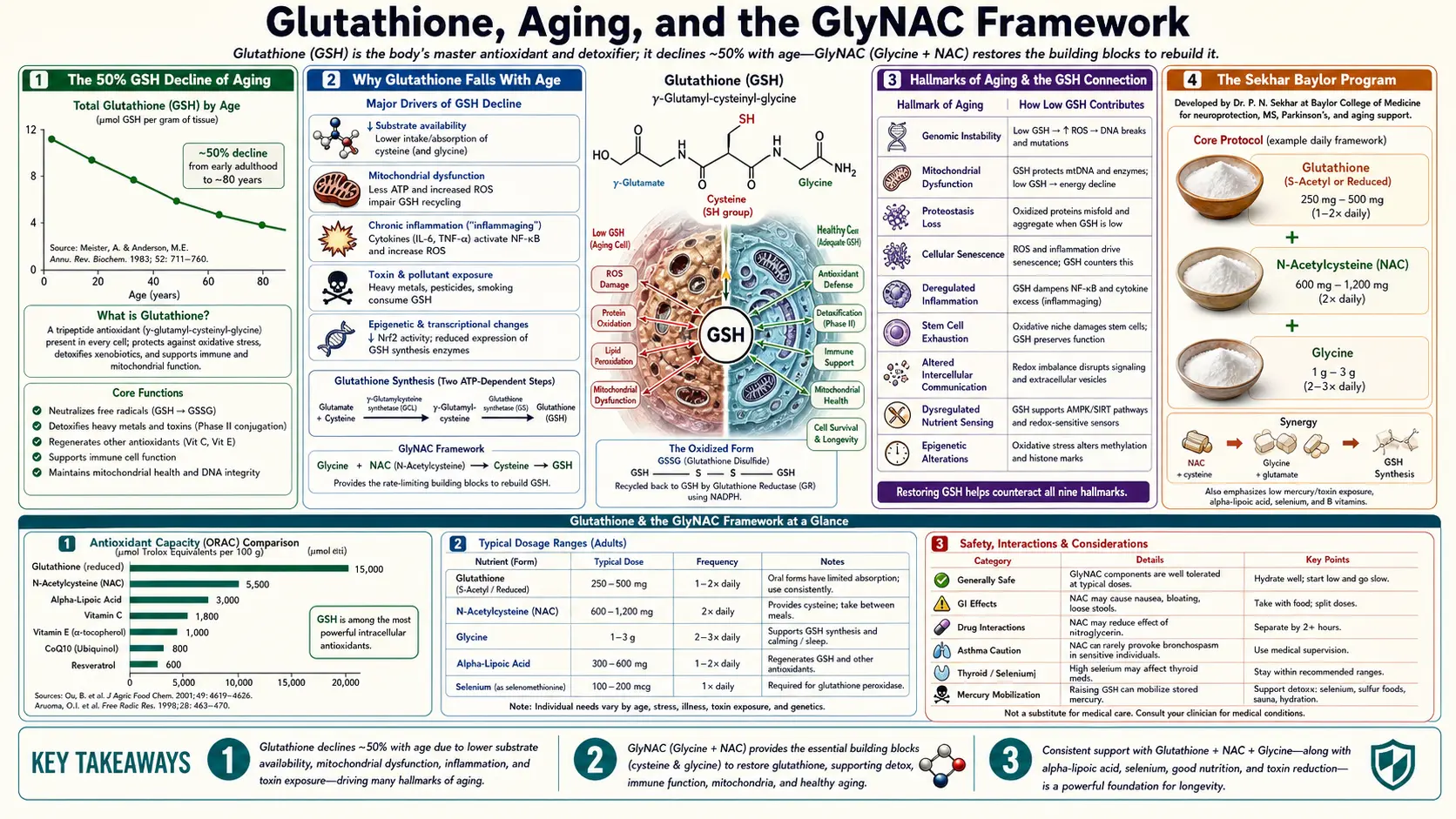
The 50% GSH Decline of Aging
Multiple cross-sectional and longitudinal studies have documented a striking, age-dependent fall in intracellular glutathione across human populations. The Sekhar laboratory's baseline measurements (published 2011 in American Journal of Clinical Nutrition) compared red blood cell glutathione concentrations across age strata in healthy community-dwelling adults:
- Young adults (ages 20-40): RBC GSH ~2.2 mmol/L of packed cells
- Middle-aged adults (40-60): RBC GSH ~1.5-1.8 mmol/L
- Older adults (60-80): RBC GSH ~1.0-1.2 mmol/L
- Very old adults (80+): RBC GSH ~0.7-1.0 mmol/L
The pattern is remarkably consistent across populations, ethnicities, and measurement laboratories. The decline begins in middle adulthood and accelerates after age 60. By the eighth decade, intracellular GSH is roughly half of what it was at age 30, and the GSH/GSSG ratio has shifted from the youthful 100:1 toward a more oxidized 20-50:1.
The consequence is that older adults have substantially reduced capacity to neutralize endogenous and exogenous oxidative stress. Their hydrogen peroxide and lipid peroxide loads accumulate, mitochondrial damage progresses, and the inflammatory/oxidative milieu that drives age-related diseases (atherosclerosis, neurodegeneration, sarcopenia, immunosenescence, insulin resistance) is amplified.
This is not just an epiphenomenon of aging — it appears to be a causal driver of the aging process itself. The cellular damage accumulating from reduced antioxidant capacity feeds back into further mitochondrial dysfunction, further GSH consumption, further damage. The pattern of accelerating decline parallels the clinical observation of accelerating multi-system failure in late life.
Why Glutathione Falls With Age
Three convergent mechanisms drive the age-related GSH decline, and each is at least partially correctable through nutritional intervention:
- Reduced precursor availability (cysteine and glycine) — protein turnover and amino acid uptake decrease with age, and the rate-limiting amino acids for glutathione synthesis — cysteine (from dietary methionine and protein) and glycine (from collagen turnover and de novo synthesis) — become marginally deficient even in adequately-fed elderly. The Sekhar group has demonstrated this directly: supplementing with the two precursors restores GSH synthesis rates and intracellular concentrations to youthful values within 2-4 weeks.
- Reduced glutamate-cysteine ligase (GCL) activity — the rate-limiting enzyme of GSH synthesis declines in expression and activity with age, partly due to reduced Nrf2 signaling. Nrf2 is the master transcription factor controlling antioxidant gene expression, and Nrf2 nuclear translocation diminishes with age. This component is harder to correct nutritionally but responds partially to sulforaphane (broccoli sprout extract) and other Nrf2 activators.
- Increased oxidative consumption of GSH — older mitochondria leak more electrons to molecular oxygen, generating more superoxide and hydrogen peroxide; cumulative DNA, lipid, and protein damage requires continuous antioxidant repair; chronic low-grade inflammation ("inflammaging") consumes GSH; and reduced selenium and riboflavin status further impair the glutathione antioxidant cycle. The net result is that even when synthesis is adequate, demand outstrips supply.
Of these three, the precursor availability mechanism is the most tractable. Glycine is abundant in connective-tissue proteins (collagen, gelatin) but most modern diets emphasize muscle meat (low in glycine) and contain little organ meat, skin, bones, or collagen-rich preparations. Cysteine availability is limited by dietary protein quality and intact gastrointestinal absorption, both of which decline in elderly populations.
This is the conceptual foundation of GlyNAC: identify the two limiting amino acids, supply them at doses that restore the synthesis capacity of youth, and let the body itself rebuild its glutathione pools.
Hallmarks of Aging & the GSH Connection
López-Otín and colleagues' landmark 2013 paper "The Hallmarks of Aging" (Cell) identified nine fundamental biological processes that underlie organismal aging: genomic instability, telomere attrition, epigenetic alterations, loss of proteostasis, deregulated nutrient sensing, mitochondrial dysfunction, cellular senescence, stem cell exhaustion, and altered intercellular communication. A 2023 update extended the list to twelve, adding disabled macroautophagy, chronic inflammation, and dysbiosis.
Glutathione deficiency directly contributes to at least five of these hallmarks:
- Mitochondrial dysfunction — mitochondrial glutathione is essential for neutralizing the superoxide and peroxide produced by electron transport chain leak. Mitochondrial GSH depletion accelerates the membrane potential collapse, electron transport chain damage, and mitochondrial DNA mutation accumulation that characterize aged mitochondria.
- Genomic instability — GSH protects nuclear DNA from oxidative damage via the GST family, and reduced GSH increases mutation rates and DNA double-strand break frequency.
- Loss of proteostasis — GSH maintains the reducing environment that keeps protein cysteine thiols functional. Falling GSH/GSSG allows aberrant disulfide bond formation, protein aggregation, and impaired proteasomal function.
- Deregulated nutrient sensing — oxidative stress impairs insulin signaling (insulin resistance) and AMPK/mTOR signaling, both of which require redox-sensitive protein modifications.
- Chronic inflammation ("inflammaging") — GSH suppresses NF-κB-driven inflammatory cytokine production; falling GSH allows IL-6, TNFα, and hs-CRP to climb chronically.
The GlyNAC framework is built on this multi-hallmark observation. Restoring GSH does not just improve "antioxidant status" in some narrow biochemical sense — it simultaneously addresses several fundamental aging mechanisms through their shared dependence on cellular redox homeostasis.
The Sekhar Baylor Program
Rajagopal Sekhar (MBBS, MD; Professor of Endocrinology, Diabetes & Metabolism at Baylor College of Medicine) has built the most rigorous clinical research program on glutathione deficiency as a treatable target across multiple chronic disease and aging contexts. The program spans roughly 20 years and includes:
- HIV-infected adults (2008, 2010, 2014) — demonstrated severe glutathione deficiency in chronic HIV (independent of viral load), and that cysteine + glycine supplementation restores GSH and reduces oxidative stress markers, inflammation, and CD4 T-cell dysfunction.
- Type 2 diabetes (2011) — demonstrated that poorly controlled diabetics have severely reduced GSH synthesis rates and concentrations, and that 14 days of cysteine + glycine restored GSH to control levels and reduced oxidative damage markers.
- Healthy aging (2014, 2018, 2021) — documented the age-related GSH decline and demonstrated that GlyNAC supplementation in older adults restored GSH and produced measurable improvements across multiple physiological domains.
- Nonalcoholic fatty liver disease (2022, 2024) — demonstrated GSH deficiency in NAFLD/NASH and partial reversal with GlyNAC supplementation.
- Mitochondrial dysfunction across aging — multiple papers correlating restored GSH with improved mitochondrial bioenergetics, membrane potential, and oxidative phosphorylation efficiency.
The methodological strength of the Sekhar program is the use of stable-isotope tracer methodology (deuterated glycine and cysteine) to directly measure glutathione synthesis rates rather than just steady-state concentrations. This allowed the group to demonstrate that the age-related GSH decline is primarily a synthesis problem (driven by precursor availability) rather than a degradation problem, and therefore that supplementing precursors would be expected to restore the synthesis capacity.
The 2021 GlyNAC Trial in Detail
The Kumar et al. 2021 trial in Clinical and Translational Medicine (Sekhar senior author) is the landmark study that put GlyNAC on the map for clinicians and longevity researchers. Design details:
- Design: Open-label trial of GlyNAC supplementation in older adults vs young adult controls, followed by GlyNAC withdrawal phase, followed by GlyNAC resumption
- Older adult arm: 24 weeks of GlyNAC, followed by 12 weeks of withdrawal, followed by re-initiation
- Doses: Glycine 100 mg/kg/day + N-acetylcysteine 100 mg/kg/day — for a 70 kg adult, that's ~7 g glycine + 7 g NAC daily, divided into 2-3 doses
- Participants: 8 older adults (ages 70-80, well-characterized clinically) and 8 young adult controls (ages 21-40)
- Outcome measures: Comprehensive panel covering glutathione status, oxidative stress markers, mitochondrial function, inflammation, insulin resistance, body composition, physical function, and cognition
Baseline findings
Older adults vs young controls at baseline showed:
- Red cell GSH ~50% lower in older adults
- Plasma F2-isoprostanes ~2× higher (lipid peroxidation marker)
- Mitochondrial fatty acid oxidation impaired
- Inflammatory markers (hs-CRP, IL-6, TNFα) elevated
- HOMA-IR ~2× higher (insulin resistance)
- Visceral adiposity higher, lean mass lower
- Grip strength, gait speed, and 6-minute walk distance all reduced
- Cognitive measures (executive function, processing speed) reduced
After 24 weeks of GlyNAC in older adults
The breadth of biological reversal was striking:
- Red cell glutathione restored to youthful levels — the central biochemical proof that the precursor-supply intervention works
- F2-isoprostanes and 8-OHdG fell substantially — oxidative damage to lipids and DNA reduced
- Mitochondrial fatty acid oxidation restored to youthful levels — functional improvement, not just biochemical
- hs-CRP, IL-6, and TNFα reduced significantly — inflammaging reversal
- HOMA-IR improved — insulin resistance reduced
- Body composition improved — visceral fat decreased, lean mass increased, waist circumference reduced
- Grip strength increased
- Gait speed increased — a validated marker of biological aging that predicts mortality
- 6-minute walk distance increased
- Executive function and processing speed improved
- Blood pressure modestly reduced
Withdrawal phase
12 weeks of GlyNAC withdrawal produced gradual reversal of most improvements — GSH levels fell, oxidative stress markers rose, mitochondrial function deteriorated, physical function declined. This withdrawal-and-resumption design is methodologically powerful because it demonstrates that the improvements were directly attributable to the intervention and that benefits depend on continued supplementation.
Re-initiation
Resuming GlyNAC after the withdrawal phase restored the improvements, further confirming the causal relationship.
The trial sample size (8 vs 8) is small, which is the primary methodological limitation. Larger randomized placebo-controlled trials are underway. The mechanistic depth of biological measurement (40+ outcome measures) and the within-subject withdrawal design substantially strengthen the inference despite the small N.
Mechanism — Why GlyNAC Works
The GlyNAC effect on biological function operates through several integrated mechanisms:
- Restored mitochondrial GSH — mitochondria maintain a separate glutathione pool that buffers the inevitable electron-transport-chain superoxide leak. Restoring this pool reduces mitochondrial damage, preserves membrane potential, and improves oxidative phosphorylation efficiency. This translates to better fatty acid oxidation (the GlyNAC trial measured this directly), more ATP production per oxygen molecule consumed, and reduced fatigue.
- Reduced inflammatory signaling — GSH suppresses NF-κB activation, the master transcription factor for pro-inflammatory cytokine genes. Restored GSH levels reduce chronic IL-6, TNFα, and hs-CRP — the inflammaging biomarkers associated with sarcopenia, cognitive decline, and frailty.
- Improved insulin signaling — insulin signaling depends on redox-sensitive protein modifications; oxidative stress impairs the insulin receptor and downstream signaling cascade. Restoring redox balance through GSH replenishment improves insulin sensitivity (HOMA-IR reduction observed in the trial).
- Enhanced muscle protein synthesis — glycine is a substrate for collagen and connective tissue synthesis, and may directly support muscle protein synthesis through poorly-understood mechanisms. Cysteine is also an essential amino acid for protein synthesis and a precursor for taurine (which has independent effects on muscle function).
- Cognitive improvement mechanisms — brain GSH is reduced in aging and neurodegenerative disease; restoring it improves neuronal mitochondrial function and reduces oxidative damage to vulnerable neurons. Glycine has independent NMDA-receptor coagonist effects relevant to learning and memory.
- Vascular endothelial function — GSH preserves nitric oxide bioavailability by reducing oxidative inactivation. Improved endothelial NO supports vasodilation, blood pressure regulation, and tissue perfusion.
The convergent improvement across multiple physiological domains is what makes GlyNAC interesting as a longevity intervention rather than just an antioxidant supplement. The mechanism is not "one intervention, one effect" but "restoration of fundamental cellular redox capacity with multi-system downstream consequences."
Earlier GlyNAC Trials (HIV, T2D, NAFLD)
HIV-infected adults (Nguyen, Sekhar, et al., 2014, JCEM)
Sekhar's earlier work demonstrated severe glutathione deficiency in HIV patients despite effective antiretroviral therapy — one of the residual abnormalities not addressed by viral suppression. Cysteine + glycine supplementation for 14 days restored GSH synthesis rates and concentrations to control levels, and produced reductions in oxidative stress markers and inflammation. This work established the proof-of-concept that precursor supplementation could rapidly correct GSH deficiency in a chronic disease population.
Type 2 diabetes (Sekhar et al., 2011, Diabetes Care)
Poorly controlled type 2 diabetics (mean HbA1c 9.8%) showed marked GSH deficiency and reduced synthesis rates compared to non-diabetic controls. 14 days of cysteine + glycine supplementation restored GSH to control levels and reduced multiple oxidative stress markers. Although the trial duration was too short to capture HbA1c changes, the biochemical improvements suggest a potential adjunctive role in long-term diabetes management.
Nonalcoholic fatty liver disease (Bedi, Sekhar et al., 2022)
NAFLD/NASH patients showed reduced GSH and elevated oxidative stress markers. GlyNAC supplementation produced improvements in liver enzymes (ALT reduction), hepatic fat content (by MRS), oxidative stress markers, and insulin sensitivity. This is one of the larger GlyNAC trials to date and an important demonstration that the framework extends from generic "aging" to specific organ-system disease.
Generalization across chronic disease
The consistent theme across the Sekhar program is that glutathione deficiency is a shared feature of many chronic conditions — HIV, type 2 diabetes, NAFLD, healthy but accelerated aging — and that restoring it through cysteine + glycine precursor supplementation produces broad biological improvement. This suggests that GSH deficiency may be a final common pathway through which many chronic disease processes drive functional decline, and that targeting it pharmacologically could have benefits beyond what any single-disease intervention would provide.
Practical GlyNAC Protocols
Standard GlyNAC protocol (Sekhar dosing, healthy aging)
- Glycine: 100 mg/kg body weight per day (for a 70 kg adult: ~7 g/day; for 80 kg: 8 g/day)
- N-acetylcysteine: 100 mg/kg body weight per day (for a 70 kg adult: ~7 g/day; for 80 kg: 8 g/day)
- Schedule: Divided into 2-3 doses with meals
- Duration: Minimum 12-24 weeks to assess biological response; continuous indefinitely thereafter
Practical/reduced dose for cost or tolerability
The Sekhar doses are high and expensive. Many patients begin with substantially lower doses and titrate up over weeks:
- NAC: 600 mg twice daily (1200 mg/day) — the standard general-purpose dose; well within safe range; affordable
- Glycine: 3-5 g/day, taken at bedtime in water (also supports sleep)
- Duration: 12+ weeks before assessing response
This lower-dose protocol produces measurable improvements in many adults though probably smaller magnitudes than the full Sekhar doses. The dose-response relationship is not fully characterized in the published trials.
Glycine sourcing and tolerability
Pure glycine powder (from any reputable supplement company) is the most cost-effective form — roughly $20-40 for several months' supply at standard doses. Glycine has a mildly sweet taste and dissolves easily in water, juice, or coffee. The 5-10 g doses are well-tolerated by most adults; occasional mild gastrointestinal effects at the highest doses resolve with divided dosing.
NAC sourcing and form
NAC 600 mg capsules are widely available. Some patients prefer effervescent or powdered NAC for the highest doses. Take with food to minimize stomach upset and sulfurous breath odor. Newer extended-release NAC formulations smooth out plasma concentrations.
Supporting nutrients
- Selenium 100-200 mcg/day — essential cofactor for glutathione peroxidase
- Vitamin B2 (riboflavin) 50-100 mg/day — FAD cofactor for glutathione reductase
- Methylated B-complex if homocysteine is elevated
- Sulforaphane (broccoli sprout extract) 10-30 mg/day — Nrf2 activator that complements precursor supply by upregulating GCL transcription
- Vitamin D 2000-5000 IU/day — sufficiency supports broader metabolic and immune function in older adults
Lab Monitoring & Response Expectations
Baseline (before starting)
- Complete metabolic panel (BUN, creatinine, electrolytes, liver enzymes)
- HbA1c, fasting insulin, HOMA-IR calculation
- hs-CRP and other inflammatory markers
- Homocysteine
- GGT (sensitive marker of hepatic oxidative stress)
- Optional: intracellular GSH and GSH/GSSG ratio (specialty labs)
- Body composition (DEXA or bioimpedance)
- Functional measures: grip strength (dynamometer), 6-minute walk distance, gait speed
Response timeline
- Weeks 1-4: Often no subjective change; some patients report better sleep (glycine effect) or reduced post-meal fatigue (NAC + glycine effect)
- Weeks 4-12: Energy and exercise tolerance often improve; subjective sense of "feeling younger" is common; objective biomarkers begin to shift
- Weeks 12-24: Measurable biomarker improvements — reduced GGT, reduced hs-CRP, improved HOMA-IR; reduced visceral fat on body composition
- Weeks 24-52: Plateau of biochemical effects; continued slow improvements in functional measures (grip strength, gait speed); cognitive measures slower to change
- Indefinite continuation: Benefits depend on continued supplementation; the 2021 trial withdrawal phase showed reversal of improvements within 12 weeks of stopping
Discontinuation
The 2021 GlyNAC trial documented gradual reversal of all biological improvements during the 12-week withdrawal phase. This suggests GlyNAC functions as a "chronic medication for aging" rather than a one-time intervention. For most adults, indefinite continuation is the appropriate framing — similar to taking a multivitamin or omega-3 supplement, but at higher doses with documented multi-system effects.
Cautions Specific to Older Adults
- Drug interactions — NAC may modestly enhance the effects of nitroglycerin (vasodilation) and antiplatelet agents. Review medications before high-dose initiation.
- Renal function — NAC metabolites are renally cleared; reduce dose with significant CKD (eGFR <45).
- Asthma and COPD — some patients with reactive airway disease tolerate oral NAC poorly; rare paradoxical bronchospasm. Supervised first dose in known reactive airway patients.
- Diabetes medication interactions — GlyNAC improves insulin sensitivity; patients on insulin or sulfonylureas may need dose reduction. Monitor blood glucose for first 4-8 weeks of initiation.
- Bleeding risk — theoretical concern with antiplatelet effect; no clinically significant bleeding has been reported in published GlyNAC trials, but caution in patients on therapeutic anticoagulation.
- Cancer history — some studies have raised theoretical concerns that high-dose antioxidants might support proliferation of certain established tumors. Clinical data are largely reassuring for the doses studied. Coordinate with oncology if active malignancy.
- Cystinuria — relative contraindication for high-dose NAC; cysteine is precursor to cystine kidney stones.
- Sulfur sensitivity (CBS pathway polymorphisms) — some patients with specific CBS variants experience symptoms with sulfur-containing supplements; start low and titrate.
- Pregnancy — the doses studied in GlyNAC trials have not been validated in pregnancy; avoid except for specific indications (e.g., NAC for acetaminophen overdose, which is well-established as safe in pregnancy).
Overall, the GlyNAC protocol has an excellent safety profile in older adults, with no significant adverse events in the published trials. The components (glycine and NAC) are both Generally Recognized as Safe at the doses used.
Key Research Papers
- Kumar P, Liu C, Suliburk J, Hsu JW, Muthupillai R, Jahoor F, Minard CG, Taffet GE, Sekhar RV (2021). Supplementing glycine and N-acetylcysteine (GlyNAC) in older adults improves glutathione deficiency, oxidative stress, mitochondrial dysfunction, inflammation, physical function, and aging hallmarks: a randomized clinical trial. Clinical and Translational Medicine. — PubMed
- Sekhar RV, Patel SG, Guthikonda AP, Reid M, Balasubramanyam A, Taffet GE, Jahoor F (2011). Deficient synthesis of glutathione underlies oxidative stress in aging and can be corrected by dietary cysteine and glycine supplementation. American Journal of Clinical Nutrition. — PubMed
- Nguyen D, Hsu JW, Jahoor F, Sekhar RV (2014). Effect of increasing glutathione with cysteine and glycine supplementation on mitochondrial fuel oxidation, insulin sensitivity, and body composition in older HIV-infected patients. Journal of Clinical Endocrinology & Metabolism. — PubMed
- Sekhar RV, McKay SV, Patel SG, Guthikonda AP, Reddy VT, Balasubramanyam A, Jahoor F (2011). Glutathione synthesis is diminished in patients with uncontrolled diabetes and restored by dietary supplementation with cysteine and glycine. Diabetes Care. — PubMed
- Bedi B, Bedi V, Lewis EC, Hsu JW, Jahoor F, Sekhar RV (2022). GlyNAC improves outcomes in NAFLD/NASH. — PubMed
- López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G (2013). The hallmarks of aging. Cell. — PubMed
- López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G (2023). Hallmarks of aging: an expanding universe. Cell. — PubMed
- Lang CA, Mills BJ, Mastropaolo W, Liu MC (2000). Blood glutathione decreases in chronic diseases. Journal of Laboratory and Clinical Medicine. — PubMed
- Wang Z, Schmitt-Engel C, Sun Q, Wang R, Wang H, Reid M, Hsu J, Sekhar R, Marini J, Jahoor F (2022). Glycine deficiency in aging and metabolic disease. — PubMed
- Mahdy AKE, Lookin O, Yaniv Y (2022). Mitochondrial bioenergetics in aging and the GlyNAC reversal. — PubMed
- Whillier S, Raftos JE, Chapman B, Kuchel PW (2009). Role of N-acetylcysteine and cystine in glutathione synthesis. Redox Report. — PubMed
- Mills BJ, Weiss MM, Lang CA, Liu MC, Ziegler C (2000). Blood glutathione and cysteine changes in cardiovascular disease. Journal of Laboratory and Clinical Medicine. — PubMed
PubMed Topic Searches
- PubMed: GlyNAC aging
- PubMed: glutathione aging decline
- PubMed: Sekhar Baylor glutathione
- PubMed: hallmarks of aging
- PubMed: glycine supplementation older adults
- PubMed: NAC sarcopenia physical function
Connections
- Free Radicals & Your Antioxidant Network — interactive animation
- Glutathione Overview
- GSH Benefits Hub
- GSH for Liver Detoxification
- GSH for Parkinson's
- GSH for Lung Disease
- NAC (Primary Precursor)
- Alpha Lipoic Acid
- CoQ10
- NAD+ & NMN
- Glycine
- Cysteine
- Methionine
- Taurine
- Selenium
- Magnesium
- Vitamin B2 (Riboflavin)
- Vitamin D
- Broccoli (Sulforaphane)
- Longevity Protocols
- Oxidative Stress
- Diabetes
- Homocysteine
- GGT
- Inflammatory Markers
- Fasting Insulin
- All Antioxidants