Glutathione for Parkinson's Disease & Dopaminergic Neuroprotection
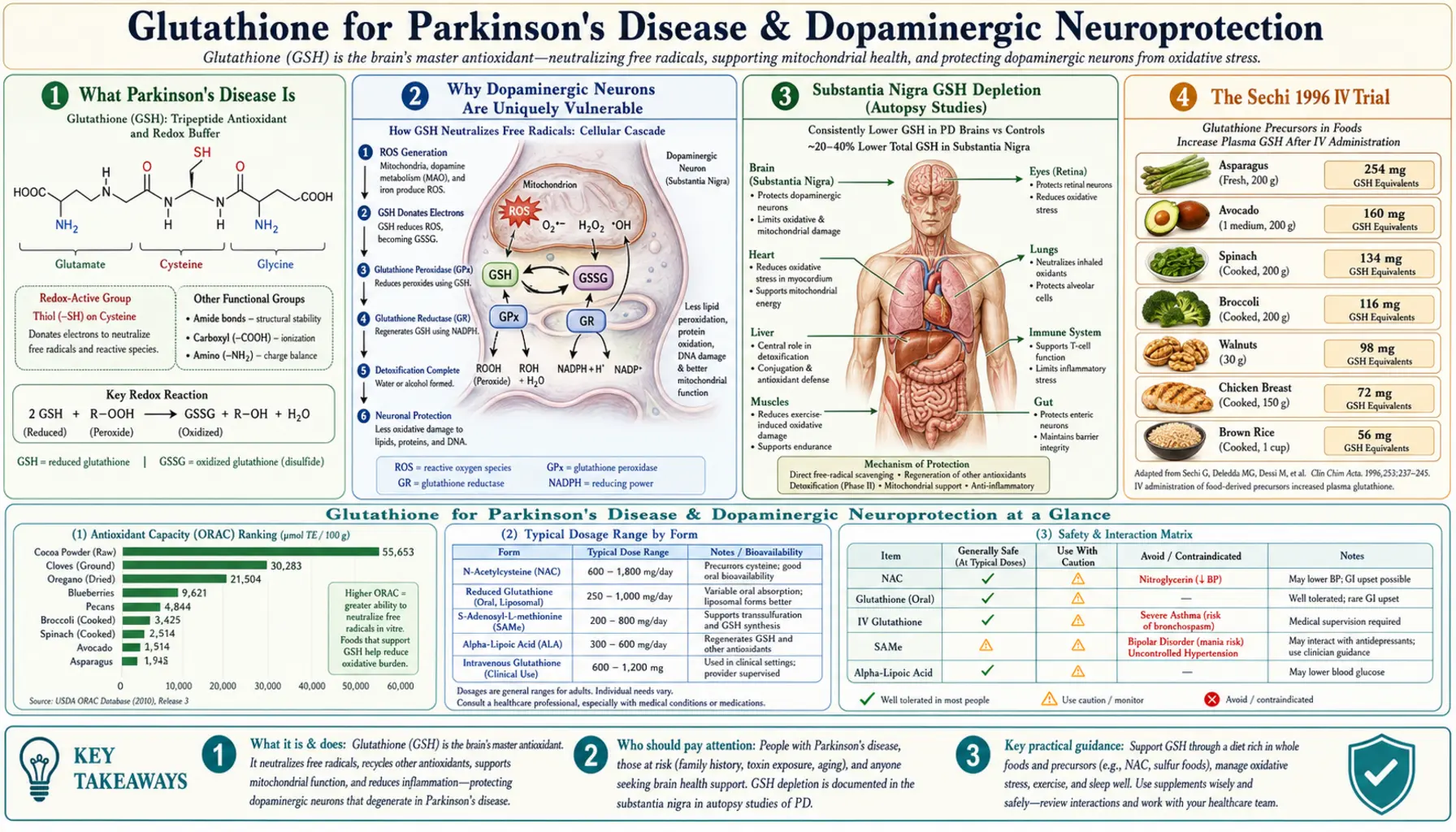
Parkinson's disease involves the selective oxidative destruction of dopaminergic neurons in the substantia nigra pars compacta. Glutathione levels in the substantia nigra are reduced by 40-50% in Parkinson's patients at autopsy, and this depletion is detectable even in early-stage disease — suggesting it may be a causal contributor rather than merely a consequence of neurodegeneration. The Sechi 1996 intravenous glutathione trial showed 42% improvement in UPDRS motor scores over 30 days at 600 mg twice daily, launching widespread off-label use of IV glutathione in integrative neurology. Subsequent controlled trials (Hauser 2009, Mischley 2017) have produced mixed but generally favorable results. This deep-dive walks through the dopaminergic-neuron oxidative vulnerability mechanism, the pivotal trials, the practical IV and intranasal protocols, and the integrative neurology framework that combines glutathione with NAC, lipoic acid, glycine, selenium, and CoQ10 for neuroprotective effect in early-stage disease.
Interactive Visualization Free Radicals & Your Antioxidant Network Follow one superoxide radical down the whole relay — SOD, catalase, glutathione, vitamin E, vitamin C, NADPH — then release free iron and watch a membrane tear itself apart. Launch →
Table of Contents
- What Parkinson's Disease Is
- Why Dopaminergic Neurons Are Uniquely Vulnerable
- Substantia Nigra GSH Depletion (Autopsy Studies)
- The Sechi 1996 IV Trial
- The Hauser 2009 Controlled Trial
- The Mischley Intranasal Trials
- NAC Trials & the Monti DaT Imaging Data
- Alpha-Synuclein, Iron, and Oxidative Modification
- Integrative Neurology Protocol (Mischley, Perlmutter)
- Practical Patient Protocol
- Patient FAQ
- Cautions Specific to Parkinson's Patients
- Key Research Papers
- Connections
- Featured Videos
What Parkinson's Disease Is
Parkinson's disease (PD) is a progressive neurodegenerative disorder characterized by the selective death of dopaminergic neurons in the substantia nigra pars compacta — the midbrain region that projects dopamine to the striatum (basal ganglia). The dopamine signal from the substantia nigra is essential for smooth, coordinated voluntary movement. As nigral neurons die, dopamine output falls; once roughly 60-80% of substantia nigra neurons have been lost, the clinical syndrome of bradykinesia, rigidity, resting tremor, and postural instability emerges.
Beyond the cardinal motor features, PD includes a constellation of non-motor manifestations: REM sleep behavior disorder (often preceding motor symptoms by 10-20 years), constipation, hyposmia (loss of smell), autonomic dysfunction, cognitive decline, depression, anxiety, and visual hallucinations. The pathological hallmark is alpha-synuclein aggregation into Lewy bodies and Lewy neurites within affected neurons.
Conventional pharmacological treatment focuses on dopamine replacement (levodopa/carbidopa) and dopamine receptor agonists (pramipexole, ropinirole, rotigotine), with adjuncts (MAO-B inhibitors selegiline and rasagiline, COMT inhibitors entacapone, the NMDA antagonist amantadine). These provide symptomatic relief but do not slow the underlying neurodegeneration. Deep brain stimulation (DBS) is reserved for advanced motor fluctuations and dyskinesias.
The fundamental therapeutic gap in PD is the absence of any approved disease-modifying intervention — nothing that actually slows the progressive loss of nigral neurons. This is the gap that glutathione, NAC, and the broader integrative neurology approach attempts to fill, particularly in early-stage disease where some neuronal rescue may still be possible. For the full clinical picture, see our Parkinson's Disease page.
Why Dopaminergic Neurons Are Uniquely Vulnerable
The substantia nigra dopaminergic neurons are among the most metabolically and oxidatively stressed neurons in the brain. Several converging factors explain their unique vulnerability:
- Dopamine itself is oxidatively unstable — dopamine spontaneously auto-oxidizes to dopamine quinones, semiquinones, and aminochrome, generating superoxide and hydrogen peroxide in the process. MAO-B metabolism of dopamine also generates hydrogen peroxide. Dopaminergic neurons therefore live with chronic intracellular ROS production simply by virtue of containing dopamine.
- Neuromelanin and iron accumulation — nigral neurons accumulate neuromelanin (a polymerized derivative of dopamine and dopa-quinone) over decades. Neuromelanin binds iron, and the substantia nigra has the highest iron concentration of any brain region. Free iron catalyzes the Fenton reaction (H2O2 + Fe2+ → OH• + OH− + Fe3+), generating extremely damaging hydroxyl radicals.
- Very high mitochondrial density and energy demand — these neurons have unusually long, unmyelinated axons with thousands of synaptic boutons, each requiring continuous mitochondrial ATP production. The high mitochondrial density means high baseline electron transport chain leak and high superoxide production.
- Calcium channel-driven autonomous firing — nigral dopaminergic neurons use Cav1.3 L-type calcium channels to drive their pacemaker firing, which produces continuous intracellular calcium oscillations. Calcium-driven mitochondrial uncoupling adds to oxidative stress.
- Reduced antioxidant capacity — nigral neurons have relatively low baseline glutathione compared to other brain regions, and lower expression of catalase, superoxide dismutase, and glutathione peroxidase. They are positioned at the edge of their antioxidant reserve under normal conditions.
- Mitochondrial complex I deficiency in PD — the iconic biochemical finding in Parkinson's substantia nigra is a 25-40% reduction in mitochondrial complex I activity, which both impairs ATP production and increases superoxide leak. This is the basis of the MPTP/MPP+ model of PD — MPTP is converted by MAO-B to MPP+, which inhibits complex I and produces a Parkinson's-like syndrome.
The combination — high baseline ROS production, high iron load, mitochondrial complex I dysfunction, and low baseline antioxidant capacity — explains why these specific neurons are uniquely vulnerable to oxidative damage and why glutathione supplementation has a particularly compelling theoretical rationale in PD. The biology is exactly the kind of setting where restoring antioxidant capacity might rescue surviving neurons and slow further loss.
Substantia Nigra GSH Depletion (Autopsy Studies)
The Sian, Dexter, Marsden group at King's College London (1990s landmark papers) and the Perry group's Vancouver autopsy series both documented dramatic and selective reductions in substantia nigra glutathione in Parkinson's patients at autopsy:
- 40-50% reduction in total substantia nigra GSH compared to age-matched non-PD controls
- Selectivity — the reduction was confined to the substantia nigra; other brain regions (cortex, striatum, cerebellum) showed normal GSH levels
- Early disease finding — reduced nigral GSH was present in patients with incidental Lewy body disease (preclinical PD identified at autopsy in patients who died of other causes), suggesting GSH depletion precedes clinical symptoms
- Independent of treatment — the reduction was present in patients who had received levodopa and in untreated patients, so it's not a drug effect
- Parallel reductions in glutathione synthesis enzymes (GCL subunits) and increased markers of oxidative damage (4-hydroxynonenal, malondialdehyde, 8-OHdG)
The temporal sequence is critical. If GSH depletion were merely a consequence of neuronal death, it would correlate with disease severity and be absent in incidental Lewy body disease. The fact that it appears in pre-symptomatic disease and precedes overt neuronal loss is consistent with a causal contribution — GSH depletion may be one of the early biochemical events that creates the oxidative milieu permitting dopaminergic degeneration to progress.
This is the clinical and biochemical foundation for considering glutathione replacement as potentially disease-modifying rather than merely symptomatic. The mechanism is plausible; the question is whether exogenous glutathione (or its precursors) can actually raise intra-nigral glutathione to therapeutic levels.
The Sechi 1996 IV Trial
Giovanni Sechi and colleagues at the University of Sassari (Sardinia) published the landmark 1996 paper in Progress in Neuropsychopharmacology & Biological Psychiatry that essentially launched IV glutathione as an off-label PD therapy in integrative neurology. The trial design was simple:
- Patients: 9 untreated, newly diagnosed Parkinson's patients (no prior levodopa or dopamine agonists)
- Intervention: Reduced glutathione 600 mg IV twice daily for 30 days (total 18 g/day cumulative)
- Design: Open-label, single-arm, with patients serving as their own pre/post controls
- Outcome measure: Unified Parkinson's Disease Rating Scale (UPDRS) motor score and global clinical assessment
Results
- 42% improvement in UPDRS motor score at the end of the 30-day treatment course
- Clinical improvement persisted for 2-4 months after the IV glutathione was discontinued before gradually declining
- Improvement was apparent in bradykinesia, rigidity, and resting tremor
- No significant adverse events; the IV infusions were well-tolerated
Limitations
The trial design has important weaknesses that subsequent commentary has emphasized:
- Small sample size (n=9)
- Open-label, no placebo control — placebo response in PD is substantial (15-25% UPDRS improvement is typical in placebo arms)
- Single center, single investigator
- Patients served as their own controls, but spontaneous early-disease variability could contribute
Impact
Despite the methodological limitations, the magnitude of effect (42% UPDRS improvement, larger than most pharmaceutical trials) and the persistence of benefit after discontinuation captured clinical attention. The study spawned widespread off-label use of IV glutathione in integrative neurology practices in Europe and the US. Many of the surviving patients of the Sechi study reportedly continued periodic IV glutathione courses with reported sustained benefit, though no formal long-term follow-up was published.
The replication record since 1996 has been mixed, but the Sechi study remains the founding clinical observation that motivates continued exploration of glutathione-based PD interventions.
The Hauser 2009 Controlled Trial
Robert Hauser and colleagues at the University of South Florida ran a small randomized, double-blind, placebo-controlled trial of IV glutathione published in Movement Disorders in 2009:
- Patients: 21 Parkinson's patients with moderate disease (Hoehn-Yahr stage 2-3)
- Intervention: IV glutathione 1400 mg three times weekly versus IV saline placebo for 4 weeks (total 12 infusions)
- Outcome measures: UPDRS motor score, global clinical impression, quality of life measures
Results
- The glutathione group showed a trend toward UPDRS improvement (mean reduction ~2.8 points) that did not reach statistical significance (p=0.32)
- Quality of life measures showed numerical but non-significant improvement
- The placebo group also showed some improvement (typical placebo response in PD trials)
- No significant adverse events; IV glutathione was well-tolerated
Interpretation
The Hauser trial is often cited as "negative" because it did not reach statistical significance, but the magnitude and direction of effect were consistent with a smaller version of the Sechi finding. Several factors likely contributed to the failure to demonstrate clear benefit:
- Underpowered — with n=21 split across two arms, the trial had limited power to detect modest effects against placebo response
- Short duration — 4 weeks vs Sechi's 30 days at twice the daily dose
- More advanced disease — Sechi enrolled untreated newly-diagnosed patients where neuronal rescue might be most feasible; Hauser enrolled patients with moderate established disease
- Less frequent dosing — three times weekly vs daily, possibly producing less sustained intracellular elevation
The Hauser trial does not refute the Sechi finding, but it tempers enthusiasm: if there is a real effect of IV glutathione on PD progression, the effect size in moderate-stage disease with intermittent dosing may be too small to detect in 21 patients over 4 weeks.
The Mischley Intranasal Trials
Laurie Mischley (ND, MPH, PhD) at Bastyr University has run the most systematic clinical program on intranasal glutathione delivery in PD. The intranasal route is appealing because it potentially delivers glutathione directly to the brain via olfactory and trigeminal nerve pathways, bypassing the blood-brain barrier limitations of oral or systemic IV administration.
Phase IIb trial (Mischley et al., 2017, Movement Disorders)
- Design: Randomized, double-blind, placebo-controlled, three-arm trial
- Patients: 45 Parkinson's patients
- Interventions: Intranasal reduced glutathione 100 mg/day, 200 mg/day, or placebo, three times daily for 3 months
- Outcome: UPDRS, quality of life, and biomarker measures
Results
- Both glutathione doses (100 mg and 200 mg) produced clinically meaningful UPDRS motor improvements that did not statistically separate from placebo
- The placebo group showed substantial improvement — the typical PD trial placebo response
- Glutathione was well-tolerated; no significant adverse events
- Subgroup analyses suggested possible greater benefit in patients with higher baseline oxidative stress markers
Interpretation
Like the Hauser trial, the Mischley study illustrates the fundamental challenge of PD neuroprotection trials: placebo response is large, the disease progresses slowly, sample sizes are typically small, and demonstrating that an intervention slows progression requires long-duration trials with careful biomarker selection.
The Mischley group has continued to develop intranasal glutathione protocols in clinical practice, where the outcomes appear (anecdotally) more favorable than the formal trial data would suggest. The intranasal route remains an active area of investigation.
NAC Trials & the Monti DaT Imaging Data
Daniel Monti and colleagues at Thomas Jefferson University Hospital have run trials of intravenous and oral NAC in Parkinson's disease with imaging biomarkers, providing some of the most provocative data in this area.
Monti 2016, 2019 trials
The Monti group's 2019 publication in Clinical Pharmacology & Therapeutics reported a randomized trial of IV NAC (50 mg/kg IV weekly) plus oral NAC (600 mg twice daily) versus standard care alone in Parkinson's patients, with DaT-SPECT imaging at baseline and 3 months:
- DaT-SPECT imaging measures dopamine transporter density in the striatum, an objective biomarker of presynaptic dopaminergic neuron integrity
- The NAC group showed measurable increased DaT binding in the caudate and putamen compared to standard-care controls
- UPDRS motor scores improved more in the NAC group
- The imaging finding is potentially the first objective evidence of dopaminergic neuron rescue or restoration in human PD trials
Interpretation
The Monti DaT imaging data are the strongest objective evidence in this entire area that antioxidant intervention can favorably affect dopaminergic neuron integrity in PD. The result has been replicated by some groups and not by others; the methodological community has debated whether the DaT changes reflect actual neuron rescue, surviving-neuron upregulation, or technical artifact.
For clinical practice, the Monti trials reinforce the use of NAC (oral 600 mg BID minimum, often higher; IV NAC weekly to monthly in some integrative protocols) as a foundational PD nutraceutical, complementing or potentially substituting for direct glutathione administration.
Alpha-Synuclein, Iron, and Oxidative Modification
Alpha-synuclein is the protein whose abnormal aggregation forms the Lewy bodies pathognomonic of Parkinson's disease. Recent biochemistry has clarified that alpha-synuclein aggregation is dramatically accelerated by oxidative modification of specific cysteine and tyrosine residues, and that glutathione status modulates this process.
- Methionine oxidation at alpha-synuclein methionine residues (Met1, Met5, Met116, Met127) shifts the protein conformation toward aggregation-prone forms
- Nitration of tyrosine residues by peroxynitrite (formed when nitric oxide reacts with superoxide) stabilizes alpha-synuclein oligomers and accelerates fibril formation
- Glutathione covalent adducts on alpha-synuclein can either accelerate or slow aggregation depending on the modification context
- Iron binding at the C-terminus of alpha-synuclein promotes aggregation; the substantia nigra's high iron load is a key contributor
- Dopamine quinone adducts on alpha-synuclein stabilize a particularly toxic oligomeric form
The convergence is striking: every modification that promotes alpha-synuclein toxicity involves an oxidative reaction that glutathione is positioned to prevent or reverse. This provides an additional mechanistic rationale for glutathione-targeted intervention — not just protecting neurons from generic oxidative damage, but specifically preventing the pathognomonic alpha-synuclein aggregation cascade.
The integrative neurology framework therefore typically pairs glutathione/NAC with iron chelators (in patients with elevated serum iron or ferritin — sometimes deferiprone is used in trial settings), reduced dietary iron (vegetable-heavy diets), and avoidance of unnecessary iron supplementation. Some advanced protocols include the lactoferrin-derived peptide pepto-glutamax that binds iron in the gut.
Integrative Neurology Protocol (Mischley, Perlmutter)
The integrative neurology approach to early-stage Parkinson's disease — pioneered by clinicians including Laurie Mischley, David Perlmutter, Roger Murphree, and others — goes beyond glutathione monotherapy to a multi-component nutraceutical protocol targeting the broader oxidative-mitochondrial-inflammatory cascade. Typical components:
- Glutathione precursors — NAC 600-1800 mg/day, glycine 5-10 g/day (GlyNAC approach)
- Direct glutathione — liposomal glutathione 500-1000 mg/day OR IV glutathione 600-2000 mg weekly to monthly OR intranasal glutathione 100-200 mg three times daily
- Alpha lipoic acid 300-600 mg/day — regenerates oxidized glutathione; crosses blood-brain barrier; addresses mitochondrial complex I dysfunction (see ALA for Neuroprotection)
- CoQ10 (ubiquinol form) 200-1200 mg/day — addresses mitochondrial complex I-III deficiency; the QE3 trial used 1200-2400 mg/day, though with mixed results
- Selenium 200 mcg/day — essential cofactor for glutathione peroxidase
- Vitamin D 5000 IU/day to target serum 25-OH-D 50-80 ng/mL — PD patients commonly deficient; deficiency associated with faster progression
- Omega-3 fatty acids (EPA + DHA) 2-4 g/day — anti-inflammatory; supports neuronal membrane integrity
- B-complex with methylated B12, methylfolate, P5P — supports methylation, transsulfuration to cysteine, and homocysteine clearance
- Vitamin K2 (MK-7) 100-200 mcg/day — some early evidence of motor benefit in PD
- Curcumin 500-1000 mg twice daily — Nrf2 activator; anti-inflammatory; some evidence of alpha-synuclein modulation
- Sulforaphane 30 mg/day from broccoli sprout extract — potent Nrf2 activator, upregulates endogenous antioxidant gene expression
- Mucuna pruriens — standardized to 15-30% L-dopa, sometimes used as adjunctive natural levodopa source; coordinate carefully with pharmaceutical levodopa dosing
This combination targets multiple mechanisms simultaneously — glutathione precursors + direct GSH for antioxidant defense, ALA + CoQ10 for mitochondrial function, omega-3 + curcumin + sulforaphane for inflammation and Nrf2 activation, B-complex for methylation. The integrative position is that the disease has multiple pathophysiological drivers and that addressing one in isolation (the conventional pharmaceutical approach) misses the converging biology.
Outcomes data on this comprehensive approach are largely anecdotal and observational (Mischley's practice registry data, clinical observation), with limited randomized trial evidence for the full combination. The components individually have varying degrees of evidence as outlined above. Patients pursuing this approach should work with an integrative neurology clinician familiar with PD management.
Practical Patient Protocol
Early-stage Parkinson's disease (Hoehn-Yahr 1-2)
- NAC 600 mg twice daily minimum; consider increasing to 1200 mg twice daily
- Glycine 5-10 g/day at bedtime
- Selenium 200 mcg/day from selenomethionine
- Alpha lipoic acid 300-600 mg/day on empty stomach
- CoQ10 (ubiquinol) 200-600 mg/day
- Vitamin D 5000 IU/day to target 25-OH-D 50-80 ng/mL
- Omega-3 (EPA + DHA) 2-4 g/day
- Methylated B-complex
- Consider liposomal glutathione 500-1000 mg/day OR periodic IV glutathione 1500-2000 mg weekly to monthly
- Consider intranasal glutathione 100-200 mg three times daily
- Exercise — vigorous aerobic exercise has the strongest evidence base of any intervention for slowing PD progression
Moderate Parkinson's disease (Hoehn-Yahr 3)
Same foundation as early-stage with these additions:
- Consider monthly to weekly IV glutathione 1500-2000 mg per the Sechi-style protocol
- Add curcumin 500-1000 mg twice daily
- Add sulforaphane 30 mg/day
- Address sleep optimization (REM behavior disorder is common; melatonin 3-9 mg HS may help)
- Coordinate carefully with neurologist on conventional dopamine replacement
Advanced Parkinson's disease (Hoehn-Yahr 4-5)
The integrative interventions become more about quality of life, swallowing safety, and reducing complications than disease modification. NAC and glycine often continued; IV glutathione less commonly used given limited evidence of meaningful effect at this stage.
IV glutathione protocol details
- Reduced glutathione 1500-2000 mg in 100-250 mL normal saline
- Infusion over 15-30 minutes
- Schedule: weekly × 4-8 weeks initially, then every 2-4 weeks for maintenance
- Reassess after 12 weeks; continue if patient reports benefit
- Performed by integrative medicine clinic or IV nutrient therapy clinic
- Cost typically $100-300 per infusion (rarely insurance-covered)
Patient FAQ
Q: Will glutathione cure my Parkinson's?
No. No intervention currently cures Parkinson's. The realistic hope with glutathione and integrative protocols is to slow progression and improve quality of life, particularly in early-stage disease. Set expectations accordingly.
Q: How quickly will I notice benefit?
Most patients who respond report subjective improvement within 2-6 weeks of starting comprehensive protocol. Objective UPDRS improvement, if it occurs, is typically apparent at 8-12 weeks. Some patients report no detectable benefit despite consistent use.
Q: Should I use IV glutathione?
The evidence for IV glutathione is mixed but the safety profile is excellent and many integrative neurologists use it routinely in early-stage disease. If accessible and affordable, a 4-8 week trial of weekly infusions is reasonable. Discontinue if no perceived benefit; continue indefinitely if clear improvement.
Q: Will glutathione replace my levodopa?
No. Glutathione and integrative protocols are complementary to conventional dopamine replacement, not substitutes. Continue your prescribed neurology medications and discuss any changes with your neurologist.
Q: Are there any interactions with my Parkinson's medications?
No significant interactions are documented between glutathione/NAC and levodopa, dopamine agonists, MAO-B inhibitors, or COMT inhibitors. The combination is well-tolerated in clinical practice.
Q: Should I get DaT-SPECT imaging to track progression?
Routine serial DaT-SPECT imaging is not standard of care. It can be useful in unclear diagnostic situations or research protocols. The Monti trial used it as an outcome measure, but for individual patients it adds cost without clear benefit beyond what clinical UPDRS assessment provides.
Q: What about exercise?
Vigorous aerobic exercise has the strongest disease-modifying evidence of any PD intervention — stronger than any medication or supplement. Aim for 150+ minutes per week of moderate-to-vigorous activity. Boxing, dance, and cycling protocols (e.g., Rock Steady Boxing, LSVT BIG) are particularly effective.
Cautions Specific to Parkinson's Patients
- Do not substitute for prescribed medications — glutathione, NAC, and integrative protocols complement conventional dopamine replacement; they do not replace it. Discontinuing levodopa or dopamine agonists without neurology supervision can cause severe motor decline or neuroleptic malignant-like syndrome.
- Coordinate with neurologist — PD management increasingly involves multiple medications with complex titration. Integrative additions should be discussed with the primary neurologist.
- L-dopa absorption interactions — levodopa is absorbed by the same intestinal transporter as large neutral amino acids (including some used in glutathione precursor protocols). Take L-dopa 30-60 minutes before high-protein meals or amino acid supplements (NAC, glycine) for optimal absorption.
- Pyridoxine (B6) caveat — high-dose pyridoxine (>25 mg/day) can increase peripheral L-dopa decarboxylation, reducing brain bioavailability. Modern carbidopa/levodopa combinations include carbidopa to prevent this, so the interaction is now less clinically significant than historically.
- Iron supplementation — given the iron-alpha-synuclein interaction, avoid iron supplements unless documented iron deficiency. Iron supplements also reduce levodopa absorption; if needed, separate dosing by 2+ hours.
- Sleep medication interactions — glycine has mild sedative properties; combine cautiously with prescription sleep medications.
- IV glutathione safety — safe when performed by trained clinicians in clinical settings. Avoid cosmetic IV glutathione protocols (those are pharmacologically different and have documented serious adverse events).
- Sulfur sensitivity — rare patients with CBS pathway polymorphisms tolerate sulfur-containing supplements poorly; start with low doses.
- Sulfurous breath / body odor — common with high-dose NAC; reduce dose, take with food, or use breath fresheners.
- Orthostatic hypotension — PD patients often have autonomic dysfunction with orthostatic hypotension. NAC and glutathione don't typically affect this but be alert to symptoms.
Key Research Papers
- Sechi G, Deledda MG, Bua G, Satta WM, Deiana GA, Pes GM, Rosati G (1996). Reduced intravenous glutathione in the treatment of early Parkinson's disease. Progress in Neuropsychopharmacology & Biological Psychiatry. — PubMed
- Hauser RA, Lyons KE, McClain T, Carter S, Perlmutter D (2009). Randomized, double-blind, pilot evaluation of intravenous glutathione in Parkinson's disease. Movement Disorders. — PubMed
- Mischley LK, Lau RC, Shankland EG, Wilbur TK, Padowski JM (2017). Phase IIb study of intranasal glutathione in Parkinson's disease. Movement Disorders. — PubMed
- Monti DA, Zabrecky G, Kremens D, Liang TW, Wintering NA, Cai J, Wei X, Bazzan AJ, Zhong L, Bowen B, Intenzo CM, Iacovitti L, Newberg AB (2019). N-acetyl cysteine is associated with dopaminergic improvement in Parkinson's disease. Clinical Pharmacology & Therapeutics. — PubMed
- Sian J, Dexter DT, Lees AJ, Daniel S, Agid Y, Javoy-Agid F, Jenner P, Marsden CD (1994). Alterations in glutathione levels in Parkinson's disease and other neurodegenerative disorders affecting basal ganglia. Annals of Neurology. — PubMed
- Perry TL, Godin DV, Hansen S (1982). Parkinson's disease: a disorder due to nigral glutathione deficiency? Neuroscience Letters. — PubMed
- Schapira AH, Cooper JM, Dexter D, Jenner P, Clark JB, Marsden CD (1990). Mitochondrial complex I deficiency in Parkinson's disease. Journal of Neurochemistry. — PubMed
- Bharath S, Hsu M, Kaur D, Rajagopalan S, Andersen JK (2002). Glutathione, iron, and Parkinson's disease. Biochemical Pharmacology. — PubMed
- Mischley LK, Standish LJ, Weiss NS, Padowski JM, Kavanagh TJ, White CC, Rosenfeld ME (2016). Glutathione as a biomarker in Parkinson's disease. Journal of the Neurological Sciences. — PubMed
- Smeyne M, Smeyne RJ (2013). Glutathione metabolism and Parkinson's disease. Free Radical Biology & Medicine. — PubMed
- Surmeier DJ, Schumacker PT, Guzman JD, Ilijic E, Yang B, Zampese E (2017). Calcium and Parkinson's disease. Biochemical and Biophysical Research Communications. — PubMed
- Olanow CW, Schapira AHV (2013). Therapeutic prospects for Parkinson disease. Annals of Neurology. — PubMed
PubMed Topic Searches
- PubMed: glutathione Parkinson disease
- PubMed: NAC Parkinson dopaminergic
- PubMed: SN GSH depletion oxidative
- PubMed: alpha-synuclein oxidation
- PubMed: complex I deficiency PD
- PubMed: integrative neurology Parkinson
Connections
- Free Radicals & Your Antioxidant Network — interactive animation
- Glutathione Overview
- GSH Benefits Hub
- GSH for Liver Detoxification
- GSH for Aging (GlyNAC)
- GSH for Lung Disease
- NAC (Primary Precursor)
- Alpha Lipoic Acid
- ALA for Neuroprotection
- CoQ10
- NAD+ & NMN
- Cysteine
- Glycine
- Tyrosine (Dopamine Precursor)
- Selenium
- Magnesium
- Vitamin D
- Vitamin B12
- Parkinson's Disease
- Mucuna Pruriens (Natural L-Dopa)
- Turmeric (Curcumin)
- Broccoli (Sulforaphane)
- Oxidative Stress
- Longevity Protocols
- Homocysteine
- Inflammatory Markers
- All Antioxidants