Astaxanthin for Cardiovascular & Lipid Health
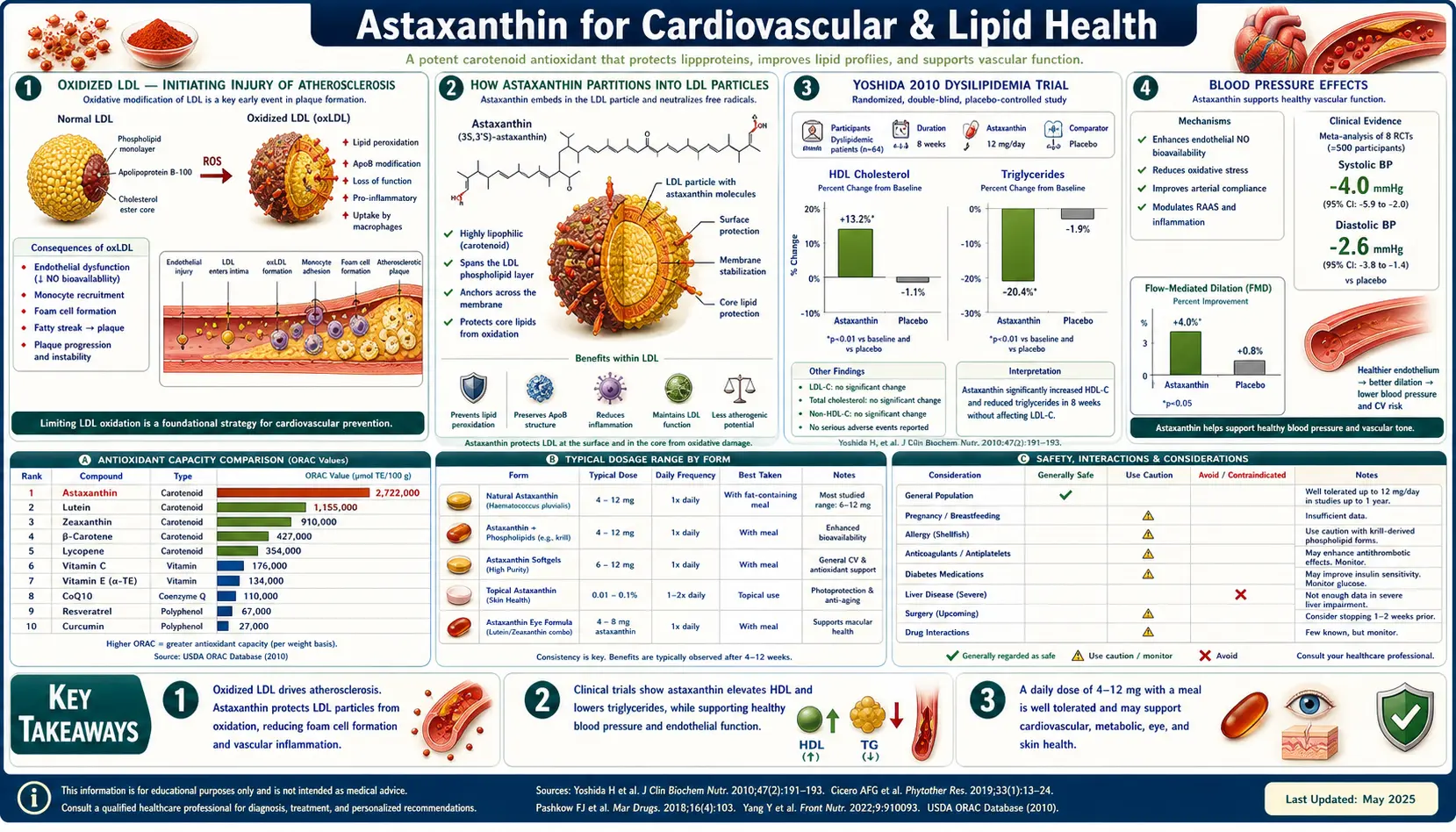
Astaxanthin partitions into lipoprotein particles in circulation and protects them from oxidative modification — oxidized LDL is the initiating injury of atherosclerosis, so this is the single most important mechanism. The Yoshida 2010 trial in patients with mild dyslipidemia showed HDL rose 10-15% and triglycerides fell 25% on 12-18 mg/day for 12 weeks. Meta-analyses pool 3-5 mmHg systolic BP reductions, flow-mediated dilation improvements indicate better endothelial function, and CRP and IL-6 fall measurably at 8-12 mg/day. Astaxanthin is not a statin and does not reduce ApoB or Lp(a) directly, but it complements statin therapy by addressing oxidative stress and inflammation — the two cardiovascular drivers statins do not fully resolve. Krill oil delivers astaxanthin alongside omega-3 phospholipids for additive benefit.
Table of Contents
- Oxidized LDL — The Initiating Injury of Atherosclerosis
- How Astaxanthin Partitions Into LDL Particles
- The Yoshida 2010 Dyslipidemia Trial (HDL and Triglycerides)
- Blood Pressure Effects
- Endothelial Function and Flow-Mediated Dilation
- CRP, IL-6, and Inflammatory Markers
- Krill Oil and the Astaxanthin + Omega-3 Synergy
- Comparison with Statins and Where Astaxanthin Fits
- ApoB, Lp(a), and Modern Lipidology Context
- Dosing Protocol and Timeline
- Cardiovascular-Specific Stack
- Cautions for Cardiovascular Use
- Key Research Papers
- Connections
- Featured Videos
Oxidized LDL — The Initiating Injury of Atherosclerosis
The modern understanding of atherosclerosis identifies oxidative modification of LDL particles within the arterial wall as the single most important initiating injury. The mechanism unfolds as follows:
- ApoB-containing lipoproteins (LDL, IDL, Lp(a), VLDL remnants) cross the arterial endothelium and accumulate in the subendothelial space
- Once retained in the artery wall (proteoglycan binding via ApoB), the lipoproteins are exposed to oxidative stress from local ROS-generating cells (macrophages, smooth muscle cells under inflammatory signaling)
- Oxidative modification of LDL phospholipids (especially the polyunsaturated fatty acid components) and ApoB protein generates oxidized LDL (oxLDL) — a neoantigen recognized by scavenger receptors on macrophages
- Macrophages internalize oxLDL via SR-A and CD36 scavenger receptors (uncontrolled, unlike normal LDL receptor uptake which is downregulated by cholesterol load), become foam cells, and accumulate in the artery wall as fatty streaks
- Foam cells release cytokines that recruit additional macrophages and trigger smooth muscle cell proliferation, leading to fibrous plaque formation and ultimately to plaque rupture and acute coronary events
The implication of this model: lipoprotein concentrations matter (you need ApoB-containing particles in the artery wall to get atherosclerosis), but oxidation is what makes those particles atherogenic. Two patients with the same LDL-C might have very different cardiovascular risk depending on how oxidation-prone their lipoprotein particles are and how much oxidative stress their artery walls generate.
This is the framing within which antioxidant therapy for cardiovascular disease should be understood. Statins reduce ApoB-containing particle numbers (the substrate); antioxidants like astaxanthin reduce the oxidation of those particles (the modification step that makes them atherogenic). They act on different parts of the same pathway and are complementary rather than competitive.
How Astaxanthin Partitions Into LDL Particles
After oral absorption, astaxanthin is incorporated into chylomicrons (along with dietary fat), released into circulation, and then transferred to LDL, HDL, and VLDL particles. The distribution roughly tracks the lipid content of each particle type, with LDL carrying the largest absolute astaxanthin load because LDL is the most abundant lipoprotein class. Approximately 30-40% of plasma astaxanthin is in LDL, 30-40% in HDL, and the remainder in VLDL and chylomicron remnants.
Within the LDL particle, astaxanthin sits in the outer phospholipid monolayer rather than the cholesterol ester core. Its trans-membrane geometry (the same orientation it adopts in cell membranes) positions it perpendicular to the phospholipid surface, with the polar end groups at the aqueous interface and the polyene chain spanning the lipid layer. This is the ideal position for protecting both the surface phospholipids (vulnerable to peroxidation initiation) and the ApoB protein epitopes (vulnerable to oxidative modification that creates the foam cell receptor).
Studies measuring LDL oxidation resistance after astaxanthin supplementation consistently show:
- Increased lag time before copper-induced LDL oxidation begins (the standard in vitro test of LDL oxidation resistance) by 5-30% depending on dose and duration
- Reduced production of conjugated dienes and lipid hydroperoxides during oxidation challenges
- Reduced TBARS (a downstream lipid peroxidation marker) in plasma
- Reduced antibodies against oxidized LDL epitopes in serum (in some trials)
The effect is meaningful but smaller in absolute terms than what statins achieve through ApoB reduction. The two mechanisms are complementary — statins reduce the number of LDL particles available to be oxidized; astaxanthin reduces the oxidation rate of the particles that remain.
The Yoshida 2010 Dyslipidemia Trial (HDL and Triglycerides)
Yoshida H, Yanai H, Ito K et al. (2010, Atherosclerosis) is the most-cited human trial of astaxanthin for lipid effects. The design tested a dose-response across the typical supplemental range in patients with mild dyslipidemia (high triglycerides, borderline-low HDL) but not on lipid-lowering medication.
Methods
- 61 adults with non-treated mild dyslipidemia (fasting triglycerides 120-200 mg/dL)
- Randomized 4-arm parallel: astaxanthin 0, 6, 12, or 18 mg/day for 12 weeks
- Outcomes: total cholesterol, LDL-C, HDL-C, triglycerides, apolipoproteins, and adiponectin at baseline, week 4, week 8, and week 12
Results
- HDL cholesterol: rose by approximately 10-15% in the 12 mg and 18 mg groups (significant). 6 mg group showed a smaller increase. This is mechanistically interesting because few interventions reliably raise HDL.
- Triglycerides: fell by approximately 25% in the 12 mg and 18 mg groups (significant). 6 mg group showed approximately 15% reduction.
- Adiponectin: rose in all dose groups, with the largest effect at 12-18 mg/day. Adiponectin is an insulin-sensitizing adipokine that is associated with reduced cardiovascular risk.
- LDL-C and total cholesterol: no significant change in any group (consistent with the mechanism — astaxanthin does not affect cholesterol synthesis or LDL particle number, only oxidation susceptibility)
- ApoB and ApoA1: minor changes; ApoB unchanged (no LDL particle reduction)
- No serious adverse events; mild dose-dependent increase in skin pigmentation visible only at 18 mg with prolonged use
The 12 mg dose produced the best balance of effect size and side-effect profile and has become the standard cardiovascular dose. The 18 mg dose did not provide proportionally additional benefit.
Clinical context: HDL +10-15% and triglycerides −25% is a meaningful lipid profile improvement, comparable to what is achieved with low-dose fibrates or high-dose niacin (both of which have significant side effects astaxanthin lacks). For patients with metabolic syndrome or mild dyslipidemia who are not yet on prescription therapy, astaxanthin is a reasonable first-line lipid intervention alongside diet and exercise.
Blood Pressure Effects
Astaxanthin produces modest blood pressure reductions across several small trials and meta-analyses, with effects typically in the 3-5 mmHg systolic and 1-3 mmHg diastolic range. The effects are larger in patients with baseline hypertension than in normotensive subjects (consistent with a regression-to-mean component plus genuine effect in those who need it most).
Mechanisms proposed for the BP effect:
- Endothelial nitric oxide protection — reduced oxidative inactivation of NO preserves vasodilation capacity. This is the dominant mechanism in most analyses.
- Mild calcium channel modulation — in vitro evidence of weak calcium channel blocking activity. Unclear clinical relevance, but consistent with reduced vascular smooth muscle tone.
- Reduced sympathetic activation — through reduced inflammation and improved endothelial function
- Mild diuretic effect — minimal but reported in some studies
For patients with stage 1 hypertension (130-139/80-89), astaxanthin 8-12 mg/day combined with diet, exercise, weight management, and stress management can sometimes obviate the need for pharmacological therapy. For patients with stage 2 hypertension or established cardiovascular disease, astaxanthin is an adjunct rather than a substitute for proven pharmacological treatment.
The combination with potassium intake (4000+ mg/day from food — potatoes, beans, leafy greens, avocados, bananas), magnesium 300-400 mg/day, and a DASH-style or Mediterranean dietary pattern produces additive BP reduction.
Endothelial Function and Flow-Mediated Dilation
The vascular endothelium — the thin cell layer lining all blood vessels — is the principal regulator of vascular tone, anti-thrombotic state, anti-inflammatory tone, and barrier function in the cardiovascular system. Endothelial dysfunction is the earliest detectable abnormality in atherosclerosis, often preceding visible structural plaque by years or decades.
Flow-mediated dilation (FMD) of the brachial artery is the standard non-invasive measure of endothelial function. The test measures how much the artery dilates after a 5-minute inflation of an upstream cuff (which causes ischemia and then reactive hyperemia, triggering nitric oxide-mediated dilation). Healthy young adults show 8-12% FMD; patients with cardiovascular disease often show under 5%. Interventions that improve FMD by 1-3 percentage points are associated with reduced cardiovascular event rates.
Astaxanthin trials in subjects with reduced FMD (mild hypertensive, mild dyslipidemic, smokers, diabetic) show 1-3 percentage point FMD improvements after 8-12 weeks of 6-12 mg/day. The mechanism: reduced oxidative inactivation of endothelial NO, allowing more NO to reach vascular smooth muscle and produce relaxation. This connects mechanistically to the BP-lowering effect (both involve preserved NO bioavailability) and to the broader atherosclerosis prevention story (endothelial dysfunction precedes plaque formation).
For patients with detectable endothelial dysfunction (low FMD, elevated ADMA, elevated endothelin), astaxanthin 8-12 mg/day plus omega-3 plus L-arginine or L-citrulline plus consistent aerobic exercise is a reasonable multi-pronged endothelial support protocol.
CRP, IL-6, and Inflammatory Markers
Vascular inflammation is increasingly recognized as a cardiovascular risk factor independent of cholesterol. The CANTOS trial (2017) showed that targeting IL-1β with canakinumab reduced cardiovascular events even in patients with already-optimal LDL-C on statins, confirming that the inflammatory pathway is a parallel target. High-sensitivity CRP (hs-CRP) is the most accessible clinical biomarker of vascular inflammation, with levels above 2 mg/L associated with elevated risk.
Astaxanthin reduces multiple inflammatory markers in clinical trials at 8-12 mg/day for 4-12 weeks:
- hs-CRP: typical reductions of 20-40% from baseline in patients with elevated CRP (smaller effects in those with already-low CRP)
- IL-6: reduced in most trials measuring it
- TNFα: reduced
- Soluble adhesion molecules (sICAM-1, sVCAM-1): reduced; these reflect endothelial activation in response to inflammation
- Oxidized LDL antibodies: reduced in some trials
The mechanism involves NF-κB inhibition (the central inflammatory transcription factor), reduced neutrophil and macrophage oxidative burst, reduced inflammasome activation, and reduced inflammatory cytokine cascades. These are the same mechanisms by which omega-3 fatty acids reduce inflammation, which is part of why the krill oil + astaxanthin combination works well — the two compounds reinforce each other.
For patients with elevated hs-CRP (over 2 mg/L) who are not yet on a statin, astaxanthin + omega-3 + addressing the underlying drivers (visceral fat, poor sleep, periodontal disease, gut dysbiosis) is a reasonable initial anti-inflammatory approach. For patients already on a statin with persistent inflammation, astaxanthin is an additive option.
Krill Oil and the Astaxanthin + Omega-3 Synergy
Krill oil (from Antarctic krill Euphausia superba) contains a distinctive lipid profile: omega-3 fatty acids (EPA and DHA) delivered as phospholipids rather than triglycerides, plus naturally co-occurring astaxanthin at concentrations of typically 100-500 mcg per gram of krill oil. The phospholipid form and the co-presence of astaxanthin distinguish krill oil from standard fish oil.
Several proposed advantages of krill oil over fish oil:
- Phospholipid omega-3 absorption — phospholipid-bound EPA and DHA may be absorbed more efficiently than triglyceride-bound forms, particularly for patients on low-fat diets where triglyceride-form fish oil absorption is limited
- Native astaxanthin content — adds the cardiovascular and anti-inflammatory benefits described in this article without requiring a separate supplement
- Better oxidation stability — the astaxanthin protects the fragile omega-3 fatty acids in the bottle from oxidation, and the phospholipid form is more oxidation-resistant than triglyceride fish oil
- No fish burp — krill oil capsules typically do not produce the reflux/fishy aftertaste that some patients experience with fish oil
However: the astaxanthin content of 1-2 g of krill oil daily is only 0.1-1 mg — well below the therapeutic dose of 4-12 mg for most clinical indications. Krill oil is a useful combination delivery vehicle but is not a substitute for standalone astaxanthin supplementation when therapeutic effects are desired.
For cardiovascular protocol: krill oil 2 g/day (delivering ~600 mg EPA+DHA in phospholipid form plus 0.5-1 mg native astaxanthin) plus standalone astaxanthin 8-12 mg/day is a reasonable combination. Alternative: standard fish oil 2-3 g EPA+DHA plus standalone astaxanthin 8-12 mg/day for the patient who is fine with fish oil capsules and wants more EPA+DHA per cost.
The synergy between omega-3 and astaxanthin operates at multiple levels: both reduce vascular inflammation through different pathways (omega-3 via resolvins and SPMs; astaxanthin via NF-κB inhibition), both improve endothelial function, both reduce triglycerides, and astaxanthin protects the omega-3 fatty acids themselves from peroxidation once incorporated into cell membranes.
Comparison with Statins and Where Astaxanthin Fits
Statins (HMG-CoA reductase inhibitors) are the foundation of modern cardiovascular pharmacology. They reduce ApoB-containing lipoprotein particles by 30-55% depending on intensity, reduce cardiovascular event rates by 20-30% in primary prevention, and reduce all-cause mortality in secondary prevention. They also have anti-inflammatory effects independent of cholesterol reduction (the "pleiotropic effects").
Astaxanthin is not a statin and does not work through the same mechanism. Key differences:
| Outcome | Statin (moderate-intensity) | Astaxanthin 12 mg/day |
|---|---|---|
| LDL-C reduction | 30-50% | No effect |
| ApoB reduction | 25-45% | No effect |
| HDL increase | ~5% | 10-15% |
| Triglyceride reduction | ~10-20% | ~25% |
| hs-CRP reduction | ~30-40% | ~20-40% |
| oxLDL reduction | Modest (via particle reduction) | Direct (via oxidation prevention) |
| Side effects | Myopathy 5-10%; diabetes risk +9%; cognitive complaints; CoQ10 depletion | Minimal at 4-12 mg/day |
| Hard cardiovascular outcome data | Extensive RCT evidence | Limited; mostly surrogate endpoints |
The framing: statins are the proven primary cardiovascular pharmacology for patients with elevated risk (ASCVD risk over 7.5-10%, established CVD, familial hypercholesterolemia, diabetes). Astaxanthin is a complementary intervention that addresses oxidation and inflammation — the parallel pathways statins do not fully resolve. The two combine well; patients on statins benefit from adding astaxanthin, and patients who cannot tolerate statins still benefit from astaxanthin's effects on HDL, triglycerides, inflammation, and oxidation even though it does not lower LDL.
One specific use case: statin-induced CoQ10 depletion. Statins reduce mevalonate pathway output, which reduces endogenous CoQ10 synthesis. This is implicated in statin-associated muscle symptoms. Adding CoQ10 100-200 mg/day plus astaxanthin 8-12 mg/day to a statin regimen often reduces muscle complaints and supports mitochondrial function in statin-treated patients.
ApoB, Lp(a), and Modern Lipidology Context
Modern lipidology has moved beyond LDL-C toward more particle-level metrics:
- ApoB — counts the total number of atherogenic lipoprotein particles (each LDL, IDL, Lp(a), and VLDL particle has exactly one ApoB-100 molecule). Better predictor of cardiovascular events than LDL-C in many comparative studies. Target under 80 mg/dL for primary prevention, under 70 mg/dL for secondary prevention.
- Lp(a) (lipoprotein little-a) — genetically determined particle similar to LDL but with an attached apolipoprotein(a). Elevated Lp(a) (above 50 mg/dL) is an independent cardiovascular risk factor affecting 20% of the population. Statins do not lower it; emerging RNA-targeted therapies (pelacarsen, olpasiran) are in late-stage trials.
- Particle size and number (NMR or ion mobility lipoprotein analysis) — small dense LDL particles are more atherogenic than large buoyant LDL. Insulin resistance and metabolic syndrome shift the particle distribution toward small dense LDL.
Where does astaxanthin fit in this landscape?
- ApoB: astaxanthin does not significantly reduce ApoB (no particle number reduction). For ApoB reduction, you need statins, PCSK9 inhibitors, ezetimibe, bempedoic acid, or bile acid sequestrants.
- Lp(a): astaxanthin does not significantly reduce Lp(a). However, astaxanthin reduces Lp(a) particle oxidation in vitro, which may be relevant for the atherogenicity of those particles regardless of their concentration.
- Particle size: astaxanthin's effect on triglycerides indirectly favors larger LDL particle size (high triglycerides drive the small dense LDL phenotype via CETP exchange). Some studies show shift toward less atherogenic particle distribution after 12 weeks of supplementation.
- HDL particle number and function: astaxanthin raises HDL-C and improves HDL functional measures (cholesterol efflux capacity) in several studies.
The integrated picture: astaxanthin is not a substitute for ApoB-reducing therapy when ApoB is elevated. But it improves the qualitative aspects of lipoprotein metabolism (oxidation resistance, HDL function, triglycerides, particle size distribution) and complements quantitative interventions like statins.
For modern lipidology-informed cardiovascular management: target ApoB under 70-80 mg/dL with statin and/or other ApoB-reducing therapy; check Lp(a) at least once per lifetime and pursue emerging therapies if elevated; add astaxanthin + omega-3 for oxidation and inflammation reduction; pursue lifestyle modifications (Mediterranean or low-carb dietary pattern, regular exercise, sleep, stress) that improve all parameters simultaneously.
Dosing Protocol and Timeline
Standard cardiovascular dose
- 8-12 mg/day astaxanthin with a fat-containing meal
- For dyslipidemia (HDL/TG focus): 12 mg/day is the dose with the strongest evidence from Yoshida 2010
- For BP and endothelial function: 8-12 mg/day produces measurable effects within 8-12 weeks
- For statin-treated patients: 8-12 mg/day plus CoQ10 100-200 mg/day
Week-by-week timeline
- Week 1-2: No visible change; tissue saturation building
- Week 4-6: First measurable changes in inflammatory markers if checked (hs-CRP starts to fall)
- Week 8-12: Lipid changes consolidate (Yoshida 2010 timeline); HDL up, TG down, hs-CRP further reduced
- Month 3-6: BP changes stabilize; endothelial function improvements measurable by FMD if checked
- Year 1+: Maintenance phase; benefits sustained indefinitely with continued dosing
Monitoring
- Baseline lipid panel + ApoB + hs-CRP before starting; recheck at 12 weeks
- Home BP monitoring 2-3 times per week for the first 8 weeks if BP is a target
- Annual lipid panel and inflammatory markers after stable on regimen
Cardiovascular-Specific Stack
- Astaxanthin 8-12 mg/day — oxidation prevention, HDL/TG improvement, inflammation reduction
- Omega-3 (EPA+DHA) 2-3 g/day (krill oil or fish oil) — triglyceride reduction, anti-inflammatory, endothelial function. Icosapent ethyl (Vascepa) is the prescription pure-EPA form with REDUCE-IT trial outcome data.
- CoQ10 / ubiquinol 100-200 mg/day — mitochondrial function; particularly important if on statins
- Vitamin K2 (MK-7) 100-200 mcg/day — arterial calcification prevention; activates matrix Gla protein
- Magnesium glycinate or malate 300-400 mg/day — BP support, arrhythmia prevention, NMDA modulation
- L-arginine or L-citrulline 3-6 g/day — nitric oxide substrate for endothelial function (alternative for those with intact endothelial NO synthesis machinery)
- Berberine 500 mg three times daily — lipid lowering and glycemic improvement via AMPK; can produce LDL reduction of 15-20% in some patients
- Nattokinase 100 mg/day — antithrombotic support (with bleeding-risk caution)
- Beetroot powder or juice — nitrate to NO pathway; produces BP reduction of 4-5 mmHg acutely
The base layer (astaxanthin + omega-3 + CoQ10 + K2 + magnesium) is appropriate for most adults with cardiovascular risk concerns. Additional ingredients are stacked based on individual circumstances and lab findings.
Cautions for Cardiovascular Use
- Hypotension — the 3-5 mmHg BP-lowering effect is generally beneficial but worth monitoring in patients on antihypertensives, particularly the first 4-8 weeks after starting. Watch for orthostatic symptoms in elderly patients.
- Antiplatelet effect at doses above 12 mg/day — theoretical bleeding-risk concern in combination with warfarin, DOACs (apixaban, rivaroxaban, dabigatran, edoxaban), aspirin, clopidogrel, or other antiplatelets. Real-world events are not well-documented but caution is reasonable. Stay at 8-12 mg/day in these patients unless otherwise indicated.
- Pre-surgery washout — stop astaxanthin 1-2 weeks before any planned cardiac procedure (CABG, valve replacement, PCI with stenting, ablation) due to bleeding-risk concern.
- Insulin sensitization — mild improvement in insulin sensitivity may produce hypoglycemia in patients on insulin or sulfonylureas. Monitor blood glucose during first 4 weeks of supplementation.
- Statin combination — safe and complementary. Astaxanthin does not interact with statin pharmacology and may reduce statin-associated muscle symptoms when combined with CoQ10.
- Anticoagulant combination — safety not definitively established at higher doses. Stay at 8 mg/day or below in patients on warfarin or DOACs without specific guidance.
- Pregnancy — avoid concentrated supplementation; dietary sources from seafood are fine.
- Shellfish allergy — choose Haematococcus-derived (algae) rather than krill-derived if severely shellfish-allergic. Algae source does not cross-react.
- Carotenoderma at very high doses — chronic doses above 50 mg/day for months can produce orange-red skin tint, particularly in palms and soles. Cosmetic only; reversible. Standard cardiovascular doses do not reach this threshold.
- Synthetic astaxanthin should not be used in humans — use only natural Haematococcus pluvialis-derived. FDA approval is for natural source only.
Key Research Papers
- Yoshida H, Yanai H, Ito K et al. (2010). Administration of natural astaxanthin increases serum HDL-cholesterol and adiponectin in subjects with mild hyperlipidemia. Atherosclerosis. — PubMed
- Iwabayashi M, Fujioka N et al. Efficacy and safety of eight-week treatment with astaxanthin in middle-aged subjects with healthy skin and lipid profile. Anti-Aging Medicine. — PubMed
- Choi HD et al. Effects of astaxanthin on oxidative stress in overweight and obese adults. Phytotherapy Research. — PubMed
- Karppi J et al. Effects of astaxanthin supplementation on lipid peroxidation. International Journal for Vitamin and Nutrition Research. — PubMed
- Mashhadi NS et al. Astaxanthin improves glucose metabolism and reduces blood pressure in patients with type 2 diabetes mellitus. Asia Pacific Journal of Clinical Nutrition. — PubMed
- Kim YK et al. Effects of astaxanthin on coronary blood flow and blood lipids. — PubMed
- Iwamoto T et al. Inhibition of low-density lipoprotein oxidation by astaxanthin. Journal of Atherosclerosis and Thrombosis. — PubMed
- Fassett RG, Coombes JS. Astaxanthin: a potential therapeutic agent in cardiovascular disease. Marine Drugs. — PubMed
- Pashkow FJ, Watumull DG, Campbell CL. Astaxanthin: a novel potential treatment for oxidative stress and inflammation in cardiovascular disease. American Journal of Cardiology. — PubMed
- Park JS et al. Astaxanthin decreased oxidative stress and inflammation and enhanced immune response in humans. Nutrition & Metabolism. — PubMed
- Saito M et al. Astaxanthin and the cardiovascular system. Cardiovascular Therapeutics. — PubMed
- Ulven SM et al. Metabolic effects of krill oil are essentially similar to those of fish oil but at lower dose of EPA and DHA. Lipids. — PubMed
PubMed Topic Searches
- PubMed: astaxanthin cardiovascular disease
- PubMed: astaxanthin HDL triglyceride lipid
- PubMed: astaxanthin oxidized LDL
- PubMed: astaxanthin blood pressure
- PubMed: astaxanthin endothelial function
- PubMed: astaxanthin CRP vascular inflammation
- PubMed: krill oil astaxanthin cardiovascular
Connections
- Astaxanthin Overview
- Astaxanthin Benefits Hub
- Astaxanthin for Eye Health
- Astaxanthin for Skin
- Astaxanthin for Exercise
- CoQ10
- Alpha Lipoic Acid
- Glutathione
- NAC
- Vitamin K2
- Vitamin E
- Vitamin C
- Magnesium
- Omega-3 (Krill Oil)
- Salmon
- Cardiology
- Cardiovascular Disease
- Cholesterol Management
- Atherosclerosis
- Hypertension
- Coronary Artery Disease
- Heart Failure
- Diabetes
- Lipid Panel
- ApoB
- Inflammatory Markers
- Oxidative Stress