Astaxanthin for Eye Health & Vision
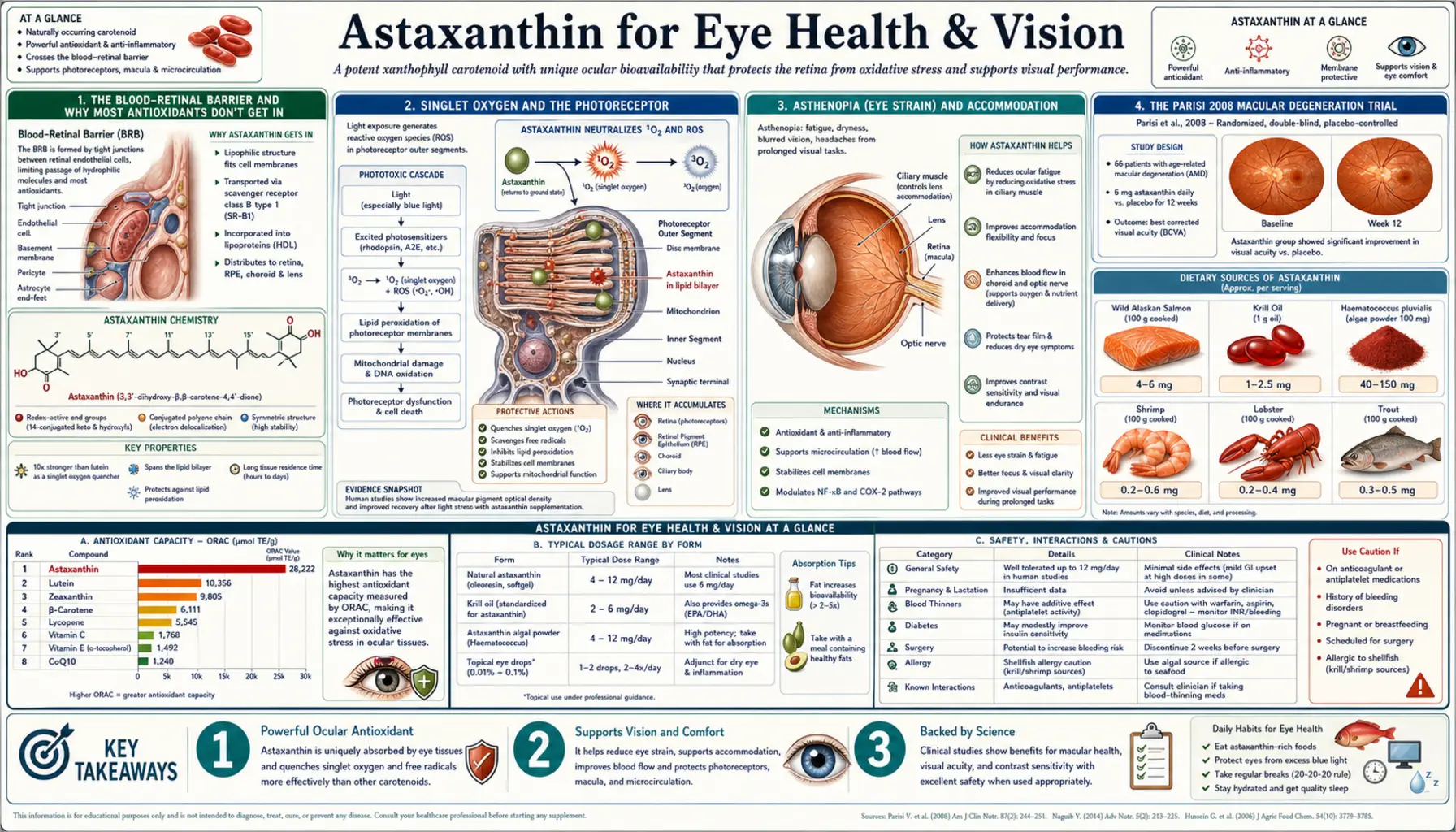
Astaxanthin is the only carotenoid that crosses both the blood-retinal barrier AND the blood-brain barrier — lutein and zeaxanthin enter the retina via specific transporters but do not enter the brain meaningfully, and beta-carotene crosses neither. This barrier-crossing combined with the strongest singlet-oxygen quenching potency of any known molecule (roughly 6,000× vitamin C and 550× vitamin E) makes astaxanthin uniquely useful in photoreceptor outer segments, the ciliary body, and the choroid. The trial base includes 4-6 mg/day asthenopia studies from Japan (Nagaki 2002, Iwasaki 2006, Nakamura 2004), the 12-month Parisi 2008 macular degeneration trial with lutein and vitamin E, the Hashimoto 2018 blue-light protection trial relevant to LED screen exposure, and accommodation amplitude improvement in computer workers.
Table of Contents
- The Blood-Retinal Barrier and Why Most Antioxidants Don't Get In
- Singlet Oxygen and the Photoreceptor
- Asthenopia (Eye Strain) and Accommodation
- The Parisi 2008 Macular Degeneration Trial
- Blue Light Protection and Screen Exposure
- Diabetic Retinopathy Pilot Data
- Dry Eye and Omega-3 Combination Trials
- Choroidal Blood Flow and Glaucoma
- Optimal Ocular Stack: Astaxanthin + Lutein + Zeaxanthin
- Dosing Protocol and Timeline
- Cautions Specific to Ocular Use
- Key Research Papers
- Connections
- Featured Videos
The Blood-Retinal Barrier and Why Most Antioxidants Don't Get In
The blood-retinal barrier is the ocular equivalent of the blood-brain barrier — a tight-junction structure formed by retinal capillary endothelium (the inner barrier) and the retinal pigment epithelium (the outer barrier) that controls what reaches retinal tissue. The barrier protects the retina from circulating pathogens, toxins, and inflammatory mediators but also excludes most water-soluble compounds and many lipophilic ones.
Vitamin C does not enter the neural retina in significant amounts; it concentrates in the aqueous humor and vitreous instead. Glutathione is synthesized locally inside lens and retinal cells but is not transported in from circulation. Vitamin E enters at modest concentrations. Beta-carotene essentially does not cross. Lutein and zeaxanthin cross via specific carotenoid-binding proteins (STARD3 and GSTP1) and concentrate dramatically in the macular pigment, but their distribution is heavily skewed to the macula rather than spread throughout the retina.
Astaxanthin crosses freely and distributes throughout the entire retina — macula, periphery, photoreceptor outer segments, retinal pigment epithelium, and the choroid behind. After 4-week oral dosing at 6 mg/day, astaxanthin appears in measurable concentrations across all these compartments. This is the structural prerequisite for the clinical effects seen in trials — astaxanthin can only protect tissue it actually reaches.
The same barrier-crossing applies to the blood-aqueous barrier (between ciliary body and aqueous humor) and the blood-brain barrier (where astaxanthin enters cortex, hippocampus, and brainstem). For the broader retinal disease context, see Macular Degeneration and the Ophthalmology landing page.
Singlet Oxygen and the Photoreceptor
The retina is one of the most metabolically active tissues in the body. Photoreceptor outer segments use oxygen at the second-highest rate per gram of any tissue (behind only the heart), they are stuffed with polyunsaturated fatty acids (especially DHA, which makes up over 50% of photoreceptor outer-segment fatty acids and is among the most peroxidation-vulnerable molecules in human biology), and they absorb focused light energy throughout waking hours.
This combination — high oxygen, high PUFA, focused light — produces continuous generation of singlet oxygen (¹O&sub2;). Unlike the more familiar superoxide and hydrogen peroxide (which have enzymatic defenses through SOD, catalase, and glutathione peroxidase), singlet oxygen has no efficient enzymatic neutralizer. The principal biological defense is carotenoids quenching the excited oxygen through energy transfer to the carotenoid polyene system.
Astaxanthin's singlet-oxygen quenching capacity is the highest measured for any biological molecule. The Shimidzu, Goto, and Miki 1996 comparative measurements (since replicated) place it at:
- Approximately 6,000× vitamin C
- 800× CoQ10
- 550× vitamin E (alpha-tocopherol)
- 11× beta-carotene
- ~5× lutein (the principal macular pigment)
The clinical implication is that astaxanthin can be effective at the 4-12 mg doses used in trials — orders of magnitude below the gram-scale doses needed for vitamin C effects — specifically because it is so efficient at this one reaction that dominates photoreceptor oxidative damage.
Asthenopia (Eye Strain) and Accommodation
Asthenopia is the medical term for eye strain — the cluster of symptoms (tired eyes, blurred vision, headache, dryness, difficulty focusing, neck and shoulder tension) that accompanies prolonged close work, especially screen use. Underlying mechanisms include ciliary muscle fatigue (from sustained accommodation for near work), reduced blink rate (drying the tear film), and lower-grade oxidative stress in the eye's muscular and vascular tissues.
The Japanese trial series in the early 2000s established astaxanthin as the only nutraceutical with reproducible randomized trial evidence for this indication:
Nagaki et al. (2002)
The seminal trial. Healthy adults received 5 mg/day astaxanthin or placebo for 4 weeks. The astaxanthin group showed statistically significant improvement in subjective asthenopia symptoms (less eye fatigue, less blurred vision, less heaviness) and an objective improvement in accommodation amplitude (the eye's focusing range, measured by accommodograph). The accommodation finding was particularly important because it represents an objective biomechanical change in ciliary muscle function, not just a subjective symptom report.
Iwasaki et al. (2006)
Focused on visual display terminal (VDT) workers — office workers who spend at least 4 hours per day at a computer. Six-week trial of 6 mg/day astaxanthin versus placebo. Results showed significant improvement on the asthenopia symptom questionnaire and reduced visual fatigue during work. Critical accommodation indices and pupillary reflex measures also improved in the astaxanthin group.
Nakamura et al. (2004)
Examined accommodation amplitude specifically in computer-using office workers. Four-week trial of 5 mg/day astaxanthin. Accommodation amplitude improved significantly compared to placebo, with the improvement most pronounced in the dominant eye. Subjective end-of-day eye-tiredness scores also fell.
For computer-heavy professionals and anyone with screen-based asthenopia symptoms, astaxanthin 4-6 mg/day is the best-evidenced nutritional intervention. Effects accumulate over weeks rather than producing acute relief — expect to assess response at the 4-6 week mark.
The Parisi 2008 Macular Degeneration Trial
Age-related macular degeneration (AMD) is the leading cause of irreversible vision loss in older adults in developed countries. The macula concentrates the carotenoid pigments lutein and zeaxanthin precisely because the body needs maximum carotenoid protection in this region of focused image formation. The AREDS and AREDS2 trials established that high-dose antioxidant-plus-zinc combinations slow AMD progression in intermediate-stage patients. Astaxanthin was not in AREDS, but Parisi et al. tested it specifically.
Parisi V, Tedeschi M, Gallinaro G, et al. (2008, Ophthalmology) randomized 27 patients with early non-exudative AMD to a combination supplement containing astaxanthin 4 mg + lutein 10 mg + zeaxanthin 1 mg + vitamin E + vitamin C + zinc + copper, taken daily for 12 months. The control group received no supplementation.
The primary outcome was multifocal electroretinography (mfERG) — an objective measurement of central retinal function in which an array of stimuli probes electrical responses across different retinal locations. The mfERG is more sensitive than standard visual acuity for early macular dysfunction.
Results showed statistically significant improvement in mfERG response density in the central macula (the 5° central foveal area) at 12 months in the supplemented group, while the control group showed progressive decline consistent with the natural history of early AMD. Visual acuity remained stable in both groups (12 months is short for visual acuity change in early AMD), but the central retinal electrophysiology improved measurably with supplementation.
The Parisi trial is small (27 patients) and uses a combination product (so the astaxanthin-specific contribution cannot be isolated), but it is the most direct evidence available for astaxanthin in AMD and supports inclusion in modern macular protection protocols alongside the AREDS2 nutrients.
Blue Light Protection and Screen Exposure
Blue light (400-490 nm wavelength range, particularly the 415-455 nm "high-energy visible" band) is the most damaging portion of the visible light spectrum for the retina. It penetrates through the cornea and lens to reach the photoreceptors and retinal pigment epithelium, where it generates ROS (especially singlet oxygen) through photochemical reactions with retinal pigments. Chronic blue-light exposure is implicated in early AMD pathophysiology.
Modern life has substantially increased blue-light exposure: LED screens (phones, tablets, computers, televisions), LED room lighting (more blue-skewed than the warm-white incandescent bulbs they replaced), and longer time indoors with reduced UV-blocking from natural daylight cycling. The retinal blue-light burden of a heavy screen user is qualitatively different from that of a person living in the pre-LED era.
Hashimoto H et al. (2018) randomized 22 healthy adults to 6 mg/day astaxanthin or placebo for 2 weeks, then exposed both groups to a controlled blue-light load. Measurements of blue-light-induced retinal oxidative stress (using a specific lipid peroxidation biomarker assayed in the tear fluid) showed significantly reduced markers in the astaxanthin group compared to placebo, suggesting astaxanthin partially shielded the retina from the experimental blue-light damage.
The clinical implication is preventive: for office workers, gamers, screen-heavy professionals, and anyone with high daily screen exposure, astaxanthin 4-6 mg/day plus lutein and zeaxanthin is a reasonable nutritional layer of retinal protection alongside the harder interventions (proper screen distance, 20-20-20 break rule, ambient room lighting that matches screen brightness, blue-light-filtering glasses for evening use).
Diabetic Retinopathy Pilot Data
Diabetic retinopathy is one of the three classic microvascular complications of diabetes (alongside nephropathy and peripheral neuropathy). Chronic hyperglycemia damages retinal capillaries through the same five pathways that drive peripheral nerve damage — the polyol pathway, AGE formation, PKC activation, hexosamine flux, and mitochondrial superoxide overproduction. The retinal capillary bed is unusually vulnerable because of its high metabolic demand and exposure to focused light energy.
Small pilot studies in diabetic patients have explored astaxanthin's effect on retinal oxidative damage markers. The general finding is that 6-12 mg/day for 8-12 weeks reduces lipid peroxidation markers in the aqueous humor and improves subjective vision quality, with some preliminary evidence of slowed retinopathy progression on fundus examination. The trial base is small, and the largest randomized trials needed to establish definitive efficacy have not been completed.
The mechanistic rationale is reasonable: astaxanthin directly addresses the unifying mitochondrial superoxide pathway, modestly inhibits aldose reductase (the polyol pathway), and improves retinal blood flow through endothelial protection. It also crosses the blood-retinal barrier where conventional aldose reductase inhibitors (which have failed in clinical development due to liver toxicity) cannot work effectively.
For diabetic patients with early retinopathy or strong family history, astaxanthin 6-12 mg/day is a reasonable adjunct alongside good glycemic control (the foundation), alpha lipoic acid 600 mg/day, benfotiamine 300 mg/day, and the AREDS2 vitamins. None of these is a substitute for tight glucose control, but the layered approach addresses different damage pathways.
Dry Eye and Omega-3 Combination Trials
Dry eye disease is a multifactorial condition involving deficient tear production, tear film instability, increased tear evaporation, and ocular surface inflammation. It is particularly common in screen-heavy professionals (reduced blink rate), post-menopausal women (hormonal influence on lacrimal glands), and patients with autoimmune conditions like Sjögren's syndrome.
Omega-3 fatty acids (EPA and DHA) have been studied for dry eye with mixed results — the DREAM trial in 2018 was disappointing despite earlier positive smaller studies. Astaxanthin has been tested mostly in combination with omega-3 (typically krill oil, which naturally contains both). The combination shows modest improvements in tear film breakup time, Schirmer test scores, and subjective dryness symptoms in several small trials.
The mechanism likely involves a combination of reduced ocular surface inflammation (both omega-3 and astaxanthin reduce inflammatory cytokines), improved meibomian gland lipid composition (omega-3 mostly), and reduced oxidative damage to the corneal epithelium (astaxanthin mostly). The combination is more biologically rational than either alone.
For dry eye, a reasonable protocol is krill oil 1-2 g/day (providing EPA, DHA, and 0.1-0.5 mg astaxanthin) PLUS standalone astaxanthin 4-6 mg/day for additive effect. Effects accumulate over 8-12 weeks. Topical lubrication and the underlying drivers (screen breaks, humidifier, treatment of any underlying autoimmune disease) remain primary.
Choroidal Blood Flow and Glaucoma
The choroid is the highly vascularized layer behind the retina that supplies oxygen and nutrients to the outer retina and photoreceptors. Choroidal blood flow declines with age and is impaired in glaucoma, AMD, and diabetic eye disease. Pharmacological agents that improve choroidal perfusion (Ginkgo biloba, some antihypertensives) have shown modest benefits in these conditions.
Several small Japanese trials (Saito et al., Nagaki et al.) have measured choroidal blood flow using laser Doppler flowmetry before and after astaxanthin supplementation at 4-12 mg/day for 4-8 weeks. Results consistently show modest improvements in choroidal blood velocity and blood volume in the supplemented group. The mechanism likely involves reduced oxidative damage to nitric oxide (preserving endothelial vasodilation capacity) and possibly mild calcium-channel modulation.
In glaucoma specifically, the pathophysiology involves both intraocular pressure (the primary target of conventional treatment) and impaired optic nerve head perfusion (an under-treated component). Astaxanthin's modest improvements in posterior segment blood flow plus its direct neuroprotective effects on retinal ganglion cells (the cell type that dies in glaucoma) make it a rational adjunct, though clinical trial data specific to glaucoma outcomes are still limited.
Optimal Ocular Stack: Astaxanthin + Lutein + Zeaxanthin
The three carotenoids work complementarily inside the eye rather than redundantly:
- Lutein and zeaxanthin — concentrate in the macular pigment, with zeaxanthin densest in the fovea and lutein spreading more peripherally. They absorb blue light directly (acting as an internal yellow filter) and quench ROS specifically in the central retina. AREDS2 doses: lutein 10 mg + zeaxanthin 2 mg.
- Astaxanthin — distributes throughout the entire retina including photoreceptor outer segments, peripheral retina, ciliary body, and choroid. Extreme singlet-oxygen quenching potency. Crosses both blood-retinal and blood-brain barriers. Typical dose 4-6 mg/day for ocular indications.
- Meso-zeaxanthin — not typically present in food but produced in the macula from dietary lutein; some supplements include it directly for additional macular density.
The complete ocular protective stack for adults at risk for AMD or with significant screen exposure: astaxanthin 4-6 mg + lutein 10-20 mg + zeaxanthin 2-4 mg + omega-3 (preferably krill oil) 1-2 g + vitamin E 200 IU + zinc 25-40 mg + copper 1-2 mg. This combines the AREDS2 formulation with the carotenoid extensions that the original AREDS trials did not test. Taken with a fatty meal (carotenoids require fat for absorption).
Dosing Protocol and Timeline
Standard ocular dose
- 4-6 mg/day astaxanthin with a fatty meal (breakfast with eggs, avocado toast, or salmon is ideal)
- Combined with lutein 10-20 mg and zeaxanthin 2-4 mg — either as combination product or stacked separately
- Source: natural Haematococcus pluvialis-derived astaxanthin only; avoid synthetic (the stereoisomer profile differs and long-term human safety data are limited)
Week-by-week timeline
- Week 1-2: No perceptible change. Plasma astaxanthin rising; tissue saturation building.
- Week 3-4: First subjective improvements often noticed — less end-of-day eye fatigue, easier focus shifts, less dryness.
- Week 5-8: Asthenopia symptom scores improve measurably (Nagaki and Nakamura trials show the most consistent effect by week 4-6).
- Month 3-6: Accommodation amplitude improvements consolidate; choroidal blood flow improvements visible on Doppler if measured.
- Year 1+: Macular function improvements consistent with the Parisi 2008 12-month timeline. Continue indefinitely for ongoing protection.
Special protocols
- Heavy screen users: 6 mg/day; consider increasing to 8 mg during especially screen-intensive work periods
- Early AMD: 4 mg/day astaxanthin within a full AREDS2 + lutein/zeaxanthin combination, indefinitely
- Diabetic with early retinopathy: 6-12 mg/day astaxanthin alongside alpha lipoic acid 600 mg, benfotiamine 300 mg, and tight glycemic control
- Dry eye: 4-6 mg/day astaxanthin + krill oil 1-2 g/day; topical lubrication for symptom relief
Cautions Specific to Ocular Use
- Carotenoderma at very high doses — chronic doses above 50 mg/day for months can produce a faint orange-red skin tint (most visible in palms and soles). Cosmetic only, reversible on dose reduction. Standard 4-12 mg ocular doses do not produce this.
- Mild hypotension — astaxanthin can lower blood pressure by 3-5 mmHg, generally beneficial but worth monitoring if you're already on antihypertensives.
- Antiplatelet effect at high doses — theoretical bleeding concern at doses above 12 mg/day in combination with anticoagulants (warfarin, DOACs) or antiplatelets (aspirin, clopidogrel). Relevant pre-cataract or pre-retinal surgery — stop astaxanthin 1-2 weeks before any planned eye surgery.
- Never use synthetic astaxanthin in humans — the synthetic form's racemic stereoisomer mix (33% 3S,3'S + 33% 3R,3'R + 33% meso) differs from the dominant 3S,3'S form in Haematococcus. Long-term human safety data exist only for natural astaxanthin. FDA approval is for natural source only.
- Shellfish allergy and marine-source caution — astaxanthin from Haematococcus pluvialis (a freshwater microalga) is the standard supplement source and does not cross-react with shellfish allergens. However, krill-oil-based products contain crustacean material and may cross-react in severe shellfish-allergic patients. Read source labels carefully and choose algae-derived for any patient with documented shellfish allergy.
- Pregnancy and breastfeeding — dietary astaxanthin from salmon and other seafood has been consumed across human history without adverse signal, but isolated supplemental doses lack pregnancy-specific clinical trials. Avoid concentrated supplementation during pregnancy in the absence of clinical guidance; dietary sources are fine.
- Glycemic effects — astaxanthin modestly improves insulin sensitivity; diabetic patients on insulin or sulfonylureas should monitor for hypoglycemia during the first 4 weeks of supplementation.
Key Research Papers
- Nagaki Y et al. (2002). Effects of astaxanthin on accommodation, critical flicker fusion, and pattern visual evoked potentials in visual display terminal workers. Journal of Traditional Medicines. — PubMed
- Iwasaki T, Tawara A et al. (2006). Effects of astaxanthin on eyestrain induced by accommodative dysfunction. Journal of the Eye (Atarashii Ganka). — PubMed
- Nakamura A et al. (2004). Astaxanthin and accommodation in adult subjects. — PubMed
- Parisi V, Tedeschi M et al. (2008). Carotenoids and antioxidants in age-related maculopathy Italian study: multifocal electroretinogram modifications after 1 year. Ophthalmology. — PubMed
- Hashimoto H et al. (2018). Effects of astaxanthin on antioxidative activity against blue-light-induced retinal damage. — PubMed
- Saito M et al. Astaxanthin increases choroidal blood flow velocity. Graefe's Archive for Clinical and Experimental Ophthalmology. — PubMed
- Piermarocchi S et al. Carotenoids in Age-related Maculopathy Italian Study (CARMIS): 2-year results. European Journal of Ophthalmology. — PubMed
- Shimidzu N, Goto M, Miki W (1996). Carotenoids as singlet oxygen quenchers in marine organisms. Fisheries Science. — PubMed
- Sasaki Y et al. Astaxanthin and visual fatigue: a randomized, double-blind, placebo-controlled study. — PubMed
- Yoshida K et al. Astaxanthin and dry eye disease. — PubMed
- Hashimoto H et al. Astaxanthin maintains performance and training quality in badminton players (visual fatigue side analysis). — PubMed
- Giannaccare G et al. Astaxanthin in age-related macular degeneration: a review. — PubMed
PubMed Topic Searches
- PubMed: astaxanthin eye vision
- PubMed: astaxanthin macular degeneration
- PubMed: astaxanthin asthenopia eye strain
- PubMed: astaxanthin blue light retina
- PubMed: astaxanthin diabetic retinopathy
- PubMed: astaxanthin dry eye tear film
- PubMed: lutein zeaxanthin astaxanthin combination
Connections
- Astaxanthin Overview
- Astaxanthin Benefits Hub
- Astaxanthin for Skin
- Astaxanthin for Exercise
- Astaxanthin for Cardiovascular
- Alpha Lipoic Acid Benefits
- CoQ10
- Glutathione
- Vitamin A (Carotenoids)
- Vitamin E
- Vitamin C
- Zinc
- Omega-3 (Krill Oil)
- Salmon
- Ophthalmology
- Macular Degeneration
- Cataracts
- Glaucoma
- Diabetes
- Oxidative Stress