Astaxanthin for Skin Photoprotection & Anti-Aging
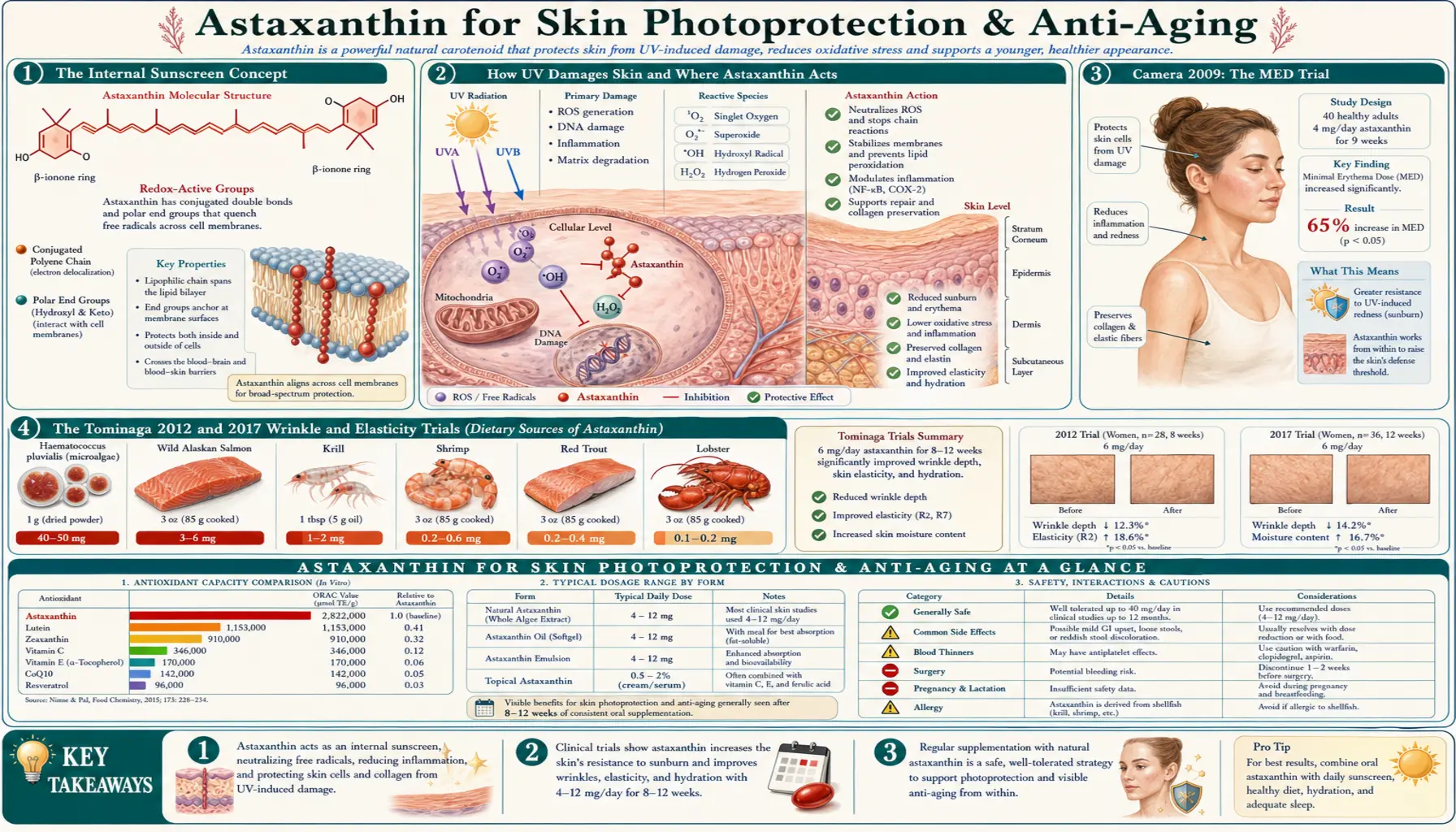
Oral astaxanthin functions as an "internal sunscreen" — it does not block UV the way topical SPF does, but it reduces the oxidative damage UV produces inside skin cells after it gets past the topical filter. Camera et al. (2009) showed that 4 mg/day for 4 weeks raised the minimal erythema dose by 15-20%. The Tominaga trials (2012, 2017) and the Davinelli 2018 systematic review pooling 11 studies established consistent improvements in skin elasticity, wrinkle depth, hydration, and corneal-layer texture at 6-12 mg/day over 8-16 weeks. The mechanism combines extreme singlet-oxygen quenching in the epidermis (where UV-induced singlet oxygen dominates the damage profile) with reduction in neutrophil oxidative burst during the inflammatory response that follows sun exposure.
Table of Contents
- The Internal Sunscreen Concept
- How UV Damages Skin and Where Astaxanthin Acts
- Camera 2009: The MED Trial
- The Tominaga 2012 and 2017 Wrinkle and Elasticity Trials
- Davinelli 2018 Systematic Review
- Topical 1-2% Astaxanthin Serum and the Combination Protocol
- Inflammatory Skin Conditions: Eczema, Acne, Seborrheic Dermatitis
- Hyperpigmentation and Age Spots
- Dosing Protocol and Timeline
- Skin-Specific Antioxidant Stack
- Cautions Specific to Skin Use
- Key Research Papers
- Connections
- Featured Videos
The Internal Sunscreen Concept
Topical sunscreens work by absorbing or reflecting UV photons before they enter the skin. They are highly effective for the wavelengths they cover but have practical limits: most people apply roughly 25% of the lab-tested SPF amount in real-world use, sunscreens lose efficacy after 2 hours of sun exposure or after swimming, certain body regions are routinely missed (ears, neck, back of hands), and chemical filters can degrade in sunlight, generating their own radicals.
"Internal sunscreens" are antioxidant compounds that get into skin tissue from the bloodstream and reduce the oxidative damage UV produces from inside the cell, regardless of how good topical protection was. They do not absorb UV photons (so they do not produce a measurable SPF in laboratory testing the way zinc oxide or octisalate do) but they reduce the downstream damage cascade that UV triggers after photons enter the skin.
Several molecules have "internal sunscreen" activity to varying degrees: Polypodium leucotomos extract, lycopene from cooked tomato, beta-carotene, lutein, vitamin C, vitamin E, niacinamide, and astaxanthin. Of these, astaxanthin has both the strongest singlet-oxygen quenching potency (the dominant ROS produced by UV in skin) and the best clinical trial base specifically for skin endpoints.
The framing matters: oral astaxanthin is additive to, not a replacement for, topical sunscreen. It is a second layer of protection that catches the oxidative damage that gets past whatever topical SPF the patient is using.
How UV Damages Skin and Where Astaxanthin Acts
UV radiation damages skin through both direct and indirect pathways:
- Direct DNA damage — UV-B (280-320 nm) photons are absorbed directly by DNA bases, producing cyclobutane pyrimidine dimers and 6-4 photoproducts. These cause mutations if not repaired before cell division.
- Singlet oxygen generation — UV-A (320-400 nm) photons are absorbed by endogenous chromophores (porphyrins, flavins, melanin precursors) which then transfer energy to molecular oxygen, generating singlet oxygen (¹O&sub2;). Singlet oxygen attacks lipid membranes, proteins, and DNA indirectly.
- Inflammation cascade — UV-damaged cells release alarmins (IL-1α, HMGB1, danger-associated molecular patterns) that recruit neutrophils and macrophages. These immune cells produce additional ROS via the neutrophil respiratory burst, amplifying tissue damage long after the UV exposure ends.
- Matrix metalloproteinase (MMP) activation — UV-triggered ROS activates MMP-1, MMP-3, and MMP-9, which degrade collagen and elastin in the dermal extracellular matrix. This is the principal mechanism of photoaging (wrinkles, sagging, leathery texture) over decades.
- Melanin dysregulation — UV stimulates melanocytes to produce melanin (the tanning response) but also drives uneven distribution that becomes age spots and melasma.
Astaxanthin acts on pathways 2, 3, and 4 primarily. It is the strongest known biological singlet-oxygen quencher, it reduces neutrophil respiratory burst (limiting the post-UV inflammatory amplification), and it reduces MMP-1 induction in keratinocyte and fibroblast cultures exposed to UV. It does not block UV photons themselves (so it does not directly prevent UV-B DNA damage), but it reduces all the downstream consequences that develop in the hours and days after exposure.
Camera 2009: The MED Trial
The minimal erythema dose (MED) is the laboratory standard for skin UV sensitivity — the UV dose required to produce just-visible redness 24 hours after exposure. A higher MED means more UV-resistant skin. MED is the foundation of SPF testing (SPF 30 means a topical raises MED 30-fold) and is also used to compare individual skin UV sensitivity across populations.
Camera E, Mastrofrancesco A, Fabbri C et al. (2009, Experimental Dermatology) tested whether oral astaxanthin alone could raise MED — the strongest direct evidence that an oral antioxidant produces measurable UV resistance.
Twenty-one healthy adult volunteers were randomized to oral astaxanthin 4 mg/day or placebo for 4 weeks. MED was measured at baseline and at 4 weeks using standardized UV solar simulators on the inner forearm. The primary endpoint was the change in MED.
Results:
- The astaxanthin group showed an approximately 15-20% increase in MED at 4 weeks — meaningful resistance to sunburn-threshold UV exposure
- The placebo group showed no change
- Reductions in UV-induced biomarkers of oxidative damage in skin biopsies (lipid peroxidation, protein oxidation) were also observed
- No adverse effects
In context: 15-20% is a modest absolute number compared to topical sunscreens (which raise MED 15-30 fold). It would not replace SPF. But the additional protection layer is real and meaningful, particularly because internal protection covers areas where topical sunscreen is routinely missed or reapplied inadequately.
The Tominaga 2012 and 2017 Wrinkle and Elasticity Trials
The Tominaga trial series — conducted at Fuji Chemical Industry's R&D in collaboration with Japanese academic dermatologists — are the largest published clinical trials of astaxanthin specifically for skin anti-aging endpoints.
Tominaga K et al. (2012, Acta Biochimica Polonica)
Thirty middle-aged adults (men and women, mean age 47) supplemented with 6 mg/day oral astaxanthin combined with 2 mL/day topical 78.9 ppm astaxanthin lotion for 8 weeks. Outcomes measured at baseline, 4 weeks, and 8 weeks:
- Crow's feet wrinkle depth — reduced significantly at 8 weeks via replica technique imaging
- Skin elasticity — improved via Cutometer (a standard dermatology device measuring skin deformation and recovery)
- Skin moisture (corneal layer hydration) — improved on Corneometer
- Skin smoothness (topographic measurements) — corneal layer roughness reduced
- Subjective skin condition (self-report) — significantly improved across multiple domains
Effects were measurable at 4 weeks but more pronounced at 8 weeks, suggesting cumulative improvement with continued use.
Tominaga K et al. (2017)
Larger study (65 healthy female subjects, age 35-60) over 16 weeks at 12 mg/day oral astaxanthin (no topical co-application this time, to isolate the oral contribution). Outcomes:
- Wrinkle parameters (Wa, Wq via replica + image analysis) significantly improved versus placebo at 16 weeks
- Skin moisture preserved better in the astaxanthin group during seasonal humidity decline (the trial period spanned summer to winter)
- Skin texture and elasticity improved
- Reductions in interleukin-1α in stratum corneum (objective inflammation marker) — supports the anti-inflammatory mechanism
The 2017 trial is important because it isolated the oral contribution — the 2012 trial confounded oral + topical and could not separate their effects. 2017 shows that oral astaxanthin alone produces measurable skin anti-aging effects, with topical providing additive (but not standalone) benefit.
Davinelli 2018 Systematic Review
Davinelli S, Nielsen ME, Scapagnini G (2018, Nutrients) performed a systematic review of 11 published clinical studies of astaxanthin for skin health, pooling outcomes across methods (oral, topical, combined; different doses, durations, and populations). The conclusion: across the heterogeneous trial base, oral astaxanthin produces consistent improvements in skin elasticity, hydration, and texture; reduces fine wrinkles; and reduces UV-induced erythema. Effect sizes are modest in absolute terms but reproducible across studies, populations, and trial designs.
The review noted that most positive trials used 4-12 mg/day for 8-16 weeks, with the best evidence at 6-12 mg/day. Higher doses do not appear to produce proportionally larger effects, suggesting a dose-response plateau in the 6-12 mg/day range. Combined oral + topical (1-2% serum) produces somewhat better outcomes than either alone, particularly for fine wrinkle reduction.
Limitations of the trial base noted by Davinelli include: relatively small sample sizes (typical n = 20-65 per study), short durations relative to the slow biology of skin aging (most studies 8-16 weeks rather than years), and reliance on Japanese trial cohorts (less data in other populations). But within those limits, the consistent direction of effect across studies is strong evidence that oral astaxanthin meaningfully affects skin biology.
Topical 1-2% Astaxanthin Serum and the Combination Protocol
Topical astaxanthin formulations are available at 0.1-3% concentrations in serums, creams, and lotions. The active astaxanthin form is delivered in lipid vehicles (squalene, jojoba oil, plant glycerol esters) that enable penetration through the stratum corneum into the viable epidermis.
Bioavailability via topical application is highly dependent on formulation. Naked astaxanthin in mineral oil penetrates poorly; properly formulated micro-emulsions or liposomal preparations reach the basal epidermis and upper dermis at meaningful concentrations within hours. The penetration depth determines the clinical effect — deeper-penetrating formulations can affect fibroblast collagen production, while surface-only formulations affect only the keratinocytes of the upper epidermis.
The standard recommendation for combined protocols:
- Oral: 6-12 mg/day astaxanthin with a fatty meal
- Topical morning: 1-2% astaxanthin serum applied before sunscreen on face, neck, and back of hands
- Topical evening: Same serum applied after cleansing, alone (no occlusive layer needed)
The combined approach addresses different sites simultaneously: oral astaxanthin distributes systemically and provides ongoing tissue-level protection across all sun-exposed skin; topical provides high local concentrations specifically where applied. The Tominaga 2012 trial showed that combining the two produces somewhat better outcomes than either alone, though the 2017 oral-only trial confirmed that oral monotherapy still works.
Inflammatory Skin Conditions: Eczema, Acne, Seborrheic Dermatitis
Beyond photoaging, astaxanthin's anti-inflammatory effects make it relevant for several chronic inflammatory skin conditions:
- Eczema (atopic dermatitis) — small trials suggest 4-8 mg/day for 8-12 weeks reduces flare frequency and itch severity, particularly in patients with adult-onset eczema rather than childhood-onset. Mechanism involves reduced Th2 inflammation and improved skin barrier function. Effect is modest but adds to standard topical therapy without interaction concerns.
- Acne — preliminary evidence (small open-label studies) suggests 4-8 mg/day reduces inflammatory acne lesion counts over 12 weeks, with the effect attributed to reduced sebum oxidation (oxidized sebum is the pro-inflammatory trigger in acne pathophysiology) and reduced neutrophil oxidative burst around pilosebaceous units. Less effective for comedonal acne than for inflammatory/cystic acne.
- Seborrheic dermatitis — case reports and small series suggest benefit in this Malassezia-driven inflammatory scalp/face condition, again via anti-inflammatory effect on the host response rather than direct antifungal action. Pairs well with conventional ketoconazole shampoo therapy.
- Psoriasis — mechanistic interest based on anti-inflammatory profile, but clinical trial evidence is limited. Anecdotal reports of benefit at 12 mg/day; not first-line.
- Rosacea — theoretical benefit from reduced inflammation and improved cutaneous vasoregulation; clinical trial data limited.
For all of these conditions, astaxanthin is an adjunct rather than a primary therapy. It works alongside standard care (topical steroids, calcineurin inhibitors, retinoids, antibiotics as appropriate) by reducing the underlying inflammation that drives the disease.
Hyperpigmentation and Age Spots
Solar lentigines (age spots, sun spots) and melasma are areas of skin hyperpigmentation driven by long-term sun exposure (lentigines) or hormonal influence on melanocyte function (melasma). Both can be cosmetically distressing and are difficult to treat — topical hydroquinone is the gold standard but has tolerability and regulatory concerns; chemical peels and laser treatments work but carry risks of post-inflammatory hyperpigmentation, particularly in darker skin types.
Small clinical trials of astaxanthin for hyperpigmentation have shown mixed but generally favorable results. The typical design pairs oral astaxanthin (6-12 mg/day) with topical (1-2% serum) over 8-12 weeks, with melanin index reduction and visible age-spot fading on standardized photography as outcomes. The effect sizes are modest — not on par with hydroquinone — but the safety profile is much more favorable, making astaxanthin a reasonable choice for patients who cannot or will not use hydroquinone.
The proposed mechanism involves reduced UV-induced melanogenic signaling (less alpha-MSH release, less tyrosinase upregulation) plus possible direct inhibition of tyrosinase at high local concentrations. The trial base is small but encouraging; expect continued research as natural pigmentation treatments grow in popularity.
For mixed conditions (photoaging + early hyperpigmentation + uneven texture), astaxanthin is well-suited because it addresses all three drivers simultaneously rather than targeting only the pigment.
Dosing Protocol and Timeline
Photoaging prevention and general anti-aging
- 6-12 mg/day oral astaxanthin with a fatty meal
- Optional topical 1-2% astaxanthin serum AM and PM
- Continue indefinitely — effects accumulate over months to years, like all anti-aging interventions
Week-by-week timeline
- Week 1-3: No visible change. Tissue saturation building.
- Week 4-6: Subjective improvements often noticed — skin feels less tight after sun exposure, fewer post-UV erythema episodes
- Week 8-12: Measurable improvements on Cutometer (elasticity), Corneometer (moisture), and replica imaging (texture, fine wrinkle depth). Tominaga 2012 timeline.
- Month 4-6: Davinelli systematic review effects fully consolidated; subjective skin quality clearly improved
- Year 1+: Maintenance phase; ongoing photoprotection from the daily UV burden
Special protocols
- Pre-vacation loading — start 4-6 weeks before significant sun exposure (beach vacation, ski trip) to maximize MED elevation before UV peak
- Post-procedure recovery — after laser resurfacing, peels, or microneedling, astaxanthin reduces post-inflammatory hyperpigmentation risk (start 1 week before procedure, continue 8-12 weeks after)
- Photoaged skin reversal — 12 mg/day oral + 2% topical for at least 16 weeks; combine with topical retinoid (separate timing) for synergistic collagen-building effect
Skin-Specific Antioxidant Stack
For comprehensive skin protection, astaxanthin combines well with several other interventions:
- Vitamin C — topical 10-20% L-ascorbic acid serum AM; oral 500-1000 mg/day. Vitamin C is a key cofactor for collagen synthesis (hydroxylates proline and lysine residues) and works in the aqueous phase complementary to astaxanthin in the lipid phase.
- Vitamin E — mixed tocopherols 200-400 IU/day oral; topical alpha-tocopherol in skin formulations. Lipid-phase antioxidant; protects sebum and cell membranes.
- Niacinamide (vitamin B3) — topical 5-10% serum AM/PM; supports skin barrier and reduces hyperpigmentation
- Topical retinoid (tretinoin, adapalene, retinol) — PM application; gold standard for collagen-building. Use astaxanthin to reduce inflammation that retinoids can cause initially.
- Topical sunscreen — broad-spectrum SPF 30-50 daily; mineral (zinc oxide, titanium dioxide) for sensitive skin; non-negotiable as the first line of UV defense
- Omega-3 fatty acids — 2-3 g EPA+DHA daily for systemic anti-inflammatory effect and skin barrier lipid composition
- Zinc — 25-30 mg/day; cofactor for wound healing and skin enzyme systems; particularly relevant for acne
The combination addresses multiple damage pathways simultaneously: prevention (sunscreen), repair (retinoid + vitamin C), antioxidant defense (astaxanthin + vitamin C + vitamin E), barrier function (niacinamide + omega-3), and anti-inflammatory tone (astaxanthin + omega-3).
Cautions Specific to Skin Use
- Carotenoderma at very high chronic doses — doses above 50 mg/day for months can produce visible orange-red tint in skin, most apparent in palms and soles. Some users consider this a desirable "healthy tan" appearance; it is cosmetic only and reverses on dose reduction. Standard 4-12 mg skin protocols do not reach this threshold.
- Topical contact dermatitis (rare) — allergic reactions to topical astaxanthin serums are uncommon but reported, typically from vehicle excipients rather than astaxanthin itself. Patch test new topical products on the inner forearm for 3-5 days before facial application.
- Sunscreen NOT optional — oral astaxanthin's 15-20% MED increase is meaningful but does not replace topical SPF. Continue daily broad-spectrum sunscreen application.
- Shellfish allergy caution for marine-source products — choose Haematococcus pluvialis-derived (algae) astaxanthin rather than krill-derived if you have severe shellfish allergy. Algae-derived does not cross-react with crustacean allergens.
- Synthetic astaxanthin should not be used in humans — the stereoisomer profile differs from natural and long-term human safety data are limited. FDA approval is for natural source only.
- Pregnancy and breastfeeding — limited data on supplemental doses. Dietary astaxanthin from salmon and seafood is fine; avoid concentrated supplements during pregnancy in the absence of clinical guidance.
- Mild antiplatelet effect at high doses — doses above 12 mg/day with anticoagulants or antiplatelets carry theoretical bleeding concern. Relevant if planning surgery (stop 1-2 weeks before).
- Mild hypotension — 3-5 mmHg BP reduction; generally beneficial but worth knowing if already on antihypertensives.
- 5-alpha reductase modulation (theoretical) — in vitro evidence of mild 5-alpha reductase inhibition. Clinical relevance unclear; some male users report mild benefits on hair loss progression at chronic high doses, but the evidence is anecdotal.
Key Research Papers
- Camera E, Mastrofrancesco A et al. (2009). Astaxanthin, canthaxanthin and beta-carotene differently affect UVA-induced oxidative damage and expression of oxidative stress-responsive enzymes. Experimental Dermatology. — PubMed
- Tominaga K, Hongo N et al. (2012). Cosmetic benefits of astaxanthin on humans subjects. Acta Biochimica Polonica. — PubMed
- Tominaga K, Hongo N, Fujishita M et al. (2017). Protective effects of astaxanthin on skin deterioration. Journal of Clinical Biochemistry and Nutrition. — PubMed
- Davinelli S, Nielsen ME, Scapagnini G (2018). Astaxanthin in skin health, repair, and disease: a comprehensive review. Nutrients. — PubMed
- Yoon HS et al. Supplementing with dietary astaxanthin combined with collagen hydrolysate improves facial elasticity. Nutrition Research and Practice. — PubMed
- Suganuma K et al. Astaxanthin attenuates the UVA-induced up-regulation of matrix-metalloproteinase-1 and skin fibroblast elastase. — PubMed
- Hama S et al. Protective effects of topical application of a poorly soluble antioxidant astaxanthin liposomal formulation. — PubMed
- Komatsu T et al. Preventive effect of dietary astaxanthin on UVA-induced skin photoaging in hairless mice. — PubMed
- Lyons NM, O'Brien NM. Modulatory effects of an algal extract containing astaxanthin on UVA-irradiated cells in culture. Journal of Dermatological Science. — PubMed
- Rao AR et al. Effective inhibition of skin cancer, tyrosinase, and antioxidative properties by astaxanthin and astaxanthin esters. — PubMed
- Singh KN et al. Astaxanthin reduces hyperpigmentation by topical application: a clinical study. — PubMed
- Shimidzu N, Goto M, Miki W (1996). Carotenoids as singlet oxygen quenchers in marine organisms. Fisheries Science. — PubMed
PubMed Topic Searches
- PubMed: astaxanthin skin photoprotection
- PubMed: astaxanthin wrinkle elasticity
- PubMed: astaxanthin UV MED
- PubMed: astaxanthin atopic dermatitis
- PubMed: astaxanthin acne
- PubMed: astaxanthin hyperpigmentation
- PubMed: topical astaxanthin serum
Connections
- Astaxanthin Overview
- Astaxanthin Benefits Hub
- Astaxanthin for Eye Health
- Astaxanthin for Exercise
- Astaxanthin for Cardiovascular
- CoQ10
- Glutathione
- NAC
- Vitamin C
- Vitamin E
- Vitamin A (Carotenoids)
- Vitamin D3
- Zinc
- Omega-3 Fatty Acids
- Dermatology
- Acne
- Eczema
- Psoriasis
- Rosacea
- Oxidative Stress
- Longevity Protocols