Vitamin B5 and Coenzyme A Biosynthesis
Coenzyme A is one of the most metabolically important cofactors in the cell. It carries acyl groups (acetyl-, succinyl-, palmityl-, malonyl-, and dozens more) through hundreds of enzymatic reactions covering fatty acid synthesis, fatty acid oxidation, the TCA cycle, ketogenesis, cholesterol biosynthesis, steroidogenesis, acetylcholine production, and Phase II acetylation detoxification. The single dietary precursor for every CoA molecule in the human body is pantothenic acid — Vitamin B5. This deep dive walks through the five-enzyme biosynthetic pathway that turns pantothenate into CoA, explains why pantothenate kinase (PANK) is the rate-limiting bottleneck, covers the parallel installation of 4'-phosphopantetheine as a prosthetic group on fatty acid synthase and acyl carrier proteins, and explains why classical clinical pantothenate deficiency is so vanishingly rare that the U.S. Institute of Medicine could not establish a formal RDA.
Table of Contents
- What Coenzyme A Does
- Pantothenate Structure
- The Five-Step CoA Biosynthesis Pathway
- Why PANK is Rate-Limiting
- 4'-Phosphopantetheine Prosthetic Groups
- CoA as Universal Acyl Carrier
- TCA Cycle, Fatty Acid Synthesis, & β-Oxidation
- Why Clinical Deficiency is Rare
- The Exception: PKAN (PANK2 Mutation)
- Absorption & Transport (SMVT)
- Cautions
- Key Research Papers
- Connections
- Featured Videos
What Coenzyme A Does
Coenzyme A — abbreviated CoA, sometimes written CoASH to emphasize its free thiol — is a complex nucleotide cofactor that carries acyl groups via a thioester bond. The structure is, from one end to the other: adenosine-3',5'-bisphosphate — pyrophosphate — pantothenate — β-mercaptoethylamine. The free thiol (−SH) on the β-mercaptoethylamine end is the business end: this is where acyl groups attach as high-energy thioesters (acetyl-CoA, succinyl-CoA, palmityl-CoA, malonyl-CoA, HMG-CoA, propionyl-CoA, and dozens of others).
The thioester linkage matters because it is high-energy — the free energy of hydrolysis of acetyl-CoA is similar to that of ATP. This means acyl-CoA molecules are kinetically primed to transfer their acyl group to acceptor substrates. CoA is, in effect, a universal "activated acyl" carrier — the way the cell hands off two-carbon (and longer) fragments between enzymes, between pathways, and between cellular compartments.
Quantitatively: CoA participates in approximately 4% of all known enzymatic reactions across all of biology. In the human cell, that includes most of the central metabolism of carbohydrates, fats, and amino acids. Every macronutrient that gets oxidized for energy passes through acetyl-CoA before entering the TCA cycle. Every fatty acid the cell synthesizes is built two carbons at a time from acetyl-CoA. Every steroid hormone in the body — cortisol, aldosterone, estrogen, testosterone, DHEA — traces back through cholesterol to acetyl-CoA. The list of CoA-dependent processes is so long that the cell-wide CoA pool is one of the most carefully regulated metabolite pools in the body.
Pantothenate Structure
Pantothenic acid is a small organic molecule: D-pantoate (a four-carbon hydroxylated branched acid) joined by an amide bond to β-alanine. The full structure is 2,4-dihydroxy-3,3-dimethylbutanoyl-β-alaninate. Only the D-(R)-enantiomer is biologically active; the L-form is inert.
The molecule embeds two structural motifs that show up later in CoA:
- The pantoate half (the four-carbon part) is structurally rigid and provides part of the binding surface that CoA-dependent enzymes recognize
- The β-alanine half (a three-carbon amino acid that is itself non-proteinogenic) provides the amide-bond linkage that will later extend, through one more amide bond, into the β-mercaptoethylamine tail that bears the active thiol
Mammalian cells cannot synthesize pantothenate from scratch; they must obtain it from diet or from gut bacteria. Plants, fungi, and most bacteria can make pantothenate from aspartate (via β-alanine) and ketoisovalerate (via pantoate). The enzymes for that synthesis (PanB, PanC, PanD, PanE) were lost in animal evolution — which is the formal reason pantothenate is a vitamin for humans rather than a synthesizable metabolite.
The Five-Step CoA Biosynthesis Pathway
Once pantothenate is inside the cell, five sequential enzymatic reactions convert it into Coenzyme A. The pathway is universally conserved across all kingdoms of life that use CoA — from E. coli to humans, the same five chemical steps in the same order.
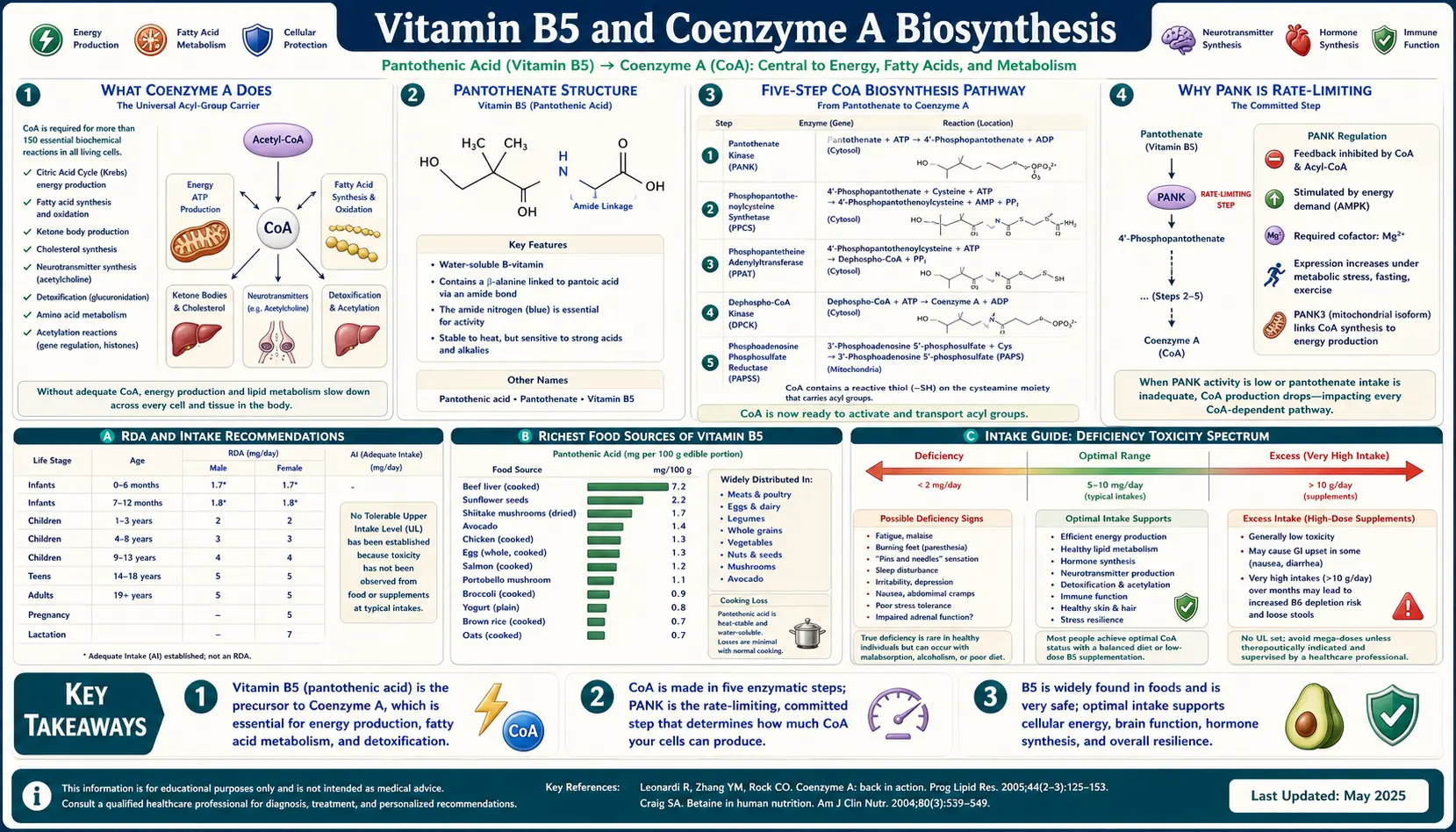
- Step 1 — Pantothenate Kinase (PANK). Pantothenate + ATP → 4'-phosphopantothenate + ADP. The pantoate hydroxyl is phosphorylated. Mammals have four isoforms: PANK1, PANK2, PANK3, PANK4. PANK2 is mitochondrial and is the isoform that, when mutated, causes the neurodegenerative disease PKAN (discussed below). PANK is the rate-limiting step of CoA biosynthesis and is feedback-inhibited by CoA, acetyl-CoA, and long-chain acyl-CoAs — a classic end-product inhibition loop.
- Step 2 — Phosphopantothenoylcysteine Synthetase (PPCS). 4'-phosphopantothenate + cysteine + CTP → 4'-phosphopantothenoylcysteine + CMP + PPi. Cysteine is attached via an amide bond — this is where the cysteine-derived thiol that will become the business end of CoA is first incorporated.
- Step 3 — Phosphopantothenoylcysteine Decarboxylase (PPCDC). 4'-phosphopantothenoylcysteine → 4'-phosphopantetheine + CO&sub2;. The carboxyl group of the cysteine residue is removed, generating the β-mercaptoethylamine tail with its free thiol.
- Step 4 — Phosphopantetheine Adenylyltransferase (PPAT, also called COASY in fused-bifunctional form). 4'-phosphopantetheine + ATP → dephospho-CoA + PPi. An ATP-derived adenylate is attached, building most of the rest of the CoA structure.
- Step 5 — Dephospho-CoA Kinase (DPCK, the second activity of COASY). Dephospho-CoA + ATP → CoA + ADP. The 3'-phosphate of the adenosine ribose is installed, yielding the final CoA molecule.
In humans, the last two steps are catalyzed by a single bifunctional enzyme called COASY (Coenzyme A Synthase) that fuses PPAT and DPCK activities into one polypeptide. COASY mutations — like PANK2 mutations — cause a rare hereditary neurodegenerative syndrome.
Stoichiometry summary: starting from one molecule of pantothenate, building one molecule of CoA requires one cysteine, four ATPs, one CTP, and releases CO&sub2; and various nucleotide byproducts. The cysteine requirement is part of why CoA biosynthesis is sometimes called a "node" in sulfur metabolism — it draws on the same cysteine pool that supplies glutathione and protein synthesis.
Why PANK is Rate-Limiting
Across virtually every tissue measured, the cellular concentration of pantothenate is much higher than the concentration of CoA. The pathway runs forward only as fast as PANK can phosphorylate pantothenate. The downstream enzymes (PPCS, PPCDC, COASY) are essentially never substrate-limited in normal cells.
PANK is also the step at which the cell regulates the CoA pool. The PANK enzymes are end-product inhibited by:
- Free CoA — competes with pantothenate at the active site
- Acetyl-CoA — the most abundant acyl-CoA species in most tissues, inhibits PANK1 and PANK3 (PANK2 is less feedback-sensitive)
- Long-chain acyl-CoAs (palmityl-CoA, stearyl-CoA) — potent allosteric inhibitors; signal that the fatty acid pool is full
The result is a homeostatic loop: when the cellular CoA pool is high, PANK slows down; when the pool drops, inhibition is relieved and the pathway speeds up. This is why supplemental pantothenate at physiologic doses has only a modest effect on the CoA pool — the rate-limiting step adjusts to keep CoA roughly constant. To meaningfully expand the CoA pool above its homeostatic setpoint, you typically need either pharmacologic-range pantothenate (gram-level doses) or, more efficiently, downstream precursors that bypass PANK — which is the rationale for pantethine supplementation (pantethine sits past the PANK step in the pathway).
4'-Phosphopantetheine Prosthetic Groups
The intermediate produced at step 3 of CoA biosynthesis — 4'-phosphopantetheine — has a parallel destiny independent of free CoA. Several enzymes incorporate 4'-phosphopantetheine as a covalently attached prosthetic group, installed by phosphopantetheinyl transferases (PPTases). The prosthetic group then functions as a swinging arm that hands off acyl intermediates between catalytic domains within a single multifunctional enzyme.
The two most important examples in human biology:
- Fatty Acid Synthase (FASN). The mammalian FAS is a large dimeric protein (~270 kDa per subunit) that catalyzes the entire seven-step cycle of fatty acid elongation in one enzymatic complex. Each round of elongation adds two carbons (from malonyl-CoA) to a growing fatty acid chain. The growing chain is tethered to a 4'-phosphopantetheine arm on the FAS's built-in acyl carrier protein (ACP) domain. The swinging arm physically delivers the chain to each catalytic domain in sequence: condensation, ketoreduction, dehydration, enoyl reduction, and so on.
- α-Aminoadipate Semialdehyde Synthase (AASS) — uses a 4'-phosphopantetheine cofactor in lysine catabolism.
- Mitochondrial ACP (mtACP) — a free-standing acyl carrier protein in mitochondria that carries 4'-phosphopantetheine and participates in mitochondrial fatty acid synthesis (the type II FAS system), which produces the octanoate precursor that the lipoic acid synthase later builds into lipoic acid — the cofactor that alpha lipoic acid supplementation targets.
These prosthetic groups are not part of the cellular CoA pool and don't turn over with it — they are installed when the host protein is folded and stay there for the protein's lifetime. But they all draw on the same upstream pool of 4'-phosphopantetheine that CoA biosynthesis uses, which means they share a dependency on dietary pantothenate.
CoA as Universal Acyl Carrier
The free CoA pool inside the cell is most directly measured by the concentration of acyl-CoA species, since free CoASH is rapidly loaded with acyl groups in active metabolism. Among the most quantitatively important acyl-CoAs:
- Acetyl-CoA — the central currency of two-carbon metabolism. Generated from pyruvate (via pyruvate dehydrogenase), from fatty acid β-oxidation, from ketogenic amino acids, and from ketone body utilization. Used to enter the TCA cycle, build fatty acids, build cholesterol, acetylate proteins, and acetylate small-molecule substrates.
- Succinyl-CoA — a TCA cycle intermediate. Also the entry point for propionyl-CoA (from branched-chain amino acid catabolism and odd-chain fatty acid oxidation, via methylmalonyl-CoA mutase — the only known mammalian enzyme that requires vitamin B12).
- Malonyl-CoA — the activated two-carbon donor for fatty acid synthesis. Built from acetyl-CoA + bicarbonate by acetyl-CoA carboxylase (ACC). High malonyl-CoA also inhibits CPT-I — the transporter that moves long-chain fatty acids into mitochondria for oxidation — thereby acting as the master metabolic switch that says "store fat, don't burn fat" when energy is abundant.
- HMG-CoA (3-hydroxy-3-methylglutaryl-CoA) — the substrate of HMG-CoA reductase, the rate-limiting step of cholesterol biosynthesis (and the target of statin drugs). Also an intermediate in ketone body production.
- Long-chain acyl-CoAs (palmityl-CoA, stearyl-CoA, oleyl-CoA) — the activated forms of long-chain fatty acids needed for transport across the mitochondrial membrane (via the carnitine shuttle) for β-oxidation, and for incorporation into phospholipids and triglycerides.
- Propionyl-CoA — produced from BCAA catabolism (valine, isoleucine, methionine, threonine) and odd-chain fatty acid oxidation. Must be metabolized through the methylmalonyl-CoA / succinyl-CoA pathway requiring biotin + vitamin B12.
The total cellular CoA pool is on the order of 0.1-0.5 mM in most tissues, with the highest pools in liver and heart (high metabolic activity). Mitochondria contain a separate, larger CoA pool than the cytosol — the inner mitochondrial membrane is impermeable to CoA, so mitochondrial and cytosolic CoA are physically segregated and have independent dynamics.
TCA Cycle, Fatty Acid Synthesis, & β-Oxidation
Three of the largest CoA-dependent metabolic processes in the cell:
Entry to the TCA Cycle
The TCA cycle begins when acetyl-CoA condenses with oxaloacetate to form citrate (catalyzed by citrate synthase). Inside the cycle, α-ketoglutarate is oxidatively decarboxylated to succinyl-CoA (by the α-ketoglutarate dehydrogenase complex, which requires lipoic acid as a cofactor). Succinyl-CoA then transfers its CoA to GDP (via succinyl-CoA synthetase) to form succinate + GTP. CoA is liberated and recycled. So in one turn of the TCA cycle, CoA is consumed at citrate synthase and regenerated at succinyl-CoA synthetase — a tight, closed loop.
Fatty Acid Synthesis
In the cytosol, fatty acid synthesis builds long-chain fatty acids two carbons at a time from acetyl-CoA. The pathway: acetyl-CoA is first carboxylated to malonyl-CoA (by acetyl-CoA carboxylase, ACC, a biotin-dependent enzyme). Then fatty acid synthase (FAS, the multi-domain mammalian enzyme) iteratively condenses malonyl-CoA units onto a growing acyl chain tethered to the 4'-phosphopantetheine arm of the ACP domain. Each round releases CO&sub2; (driving the reaction forward) and produces a chain extended by 2 carbons. After 7 rounds, palmitoyl-ACP (16-carbon palmitate) is released. This pathway is the main reason for the obesity-relevant role of ACC: when ACC is highly active (postprandial, high insulin), the cell makes malonyl-CoA, which both drives fatty acid synthesis AND inhibits fat oxidation. When ACC is suppressed (fasting, low insulin, AMPK active), malonyl-CoA falls, CPT-I is uninhibited, and the cell switches to burning fat.
β-Oxidation
Long-chain fatty acids are activated to acyl-CoAs in the cytosol (by acyl-CoA synthetase, consuming 2 ATP-equivalents), then transported into mitochondria via the carnitine shuttle (carnitine palmitoyltransferase I and II, with carnitine-acylcarnitine translocase in between). Once inside the mitochondrial matrix, each round of β-oxidation chops off two carbons as acetyl-CoA, generates one FADH2 and one NADH, and shortens the acyl-CoA chain by 2. Palmitate (16 C) yields 8 acetyl-CoAs after 7 rounds. Those acetyl-CoAs then enter the TCA cycle.
The CoA accounting is striking: a single round of β-oxidation of palmitate uses 1 free CoASH at the start (to load the fatty acid), generates 1 acetyl-CoA at the end, and consumes/regenerates additional CoA at each chain-shortening step. In active fat oxidation (during fasting, exercise, ketogenic diet), the mitochondrial CoA pool turns over many times per minute.
Why Clinical Deficiency is Rare
Two structural reasons explain why classical pantothenate deficiency — with measurable depletion of the CoA pool and downstream metabolic consequences — is essentially never seen in free-living humans:
- Pantothenate is in essentially every food. The name itself comes from the Greek "pantos" (everywhere). Animal foods, plant foods, fungi, dairy, grains, legumes — all contain pantothenate, typically at meaningful concentrations. A diet diverse enough to provide any reasonable calorie intake is essentially guaranteed to provide adequate pantothenate.
- The gut microbiome produces pantothenate. Many of the bacteria that colonize the human large intestine retain the PanB/PanC/PanD/PanE biosynthesis pathway that mammalian cells have lost. They synthesize pantothenate that is then absorbed via the colonic SMVT transporter. The exact quantitative contribution of microbial pantothenate to human pantothenate status is not precisely measured, but it is non-trivial — germ-free animal studies show pantothenate is among the B-vitamins whose status drops measurably when the microbiome is eliminated.
Together, these two sources mean that even in nutritionally deprived populations, frank pantothenate deficiency is extraordinarily uncommon. The Institute of Medicine could not gather enough deficiency data to establish a formal RDA for pantothenate — instead, they set an "Adequate Intake" (AI) of 5 mg/day for adults, based on the typical intake observed in healthy populations rather than on a documented requirement.
The two settings where experimental pantothenate deficiency has been produced in humans:
- WWII POW studies (the "burning feet syndrome"). Severe long-term malnutrition in some prisoner-of-war populations produced a syndrome characterized by burning, painful feet, fatigue, headache, irritability, and digestive symptoms that responded to pantothenate supplementation. This is the closest documented case of frank human pantothenate deficiency in a non-experimental setting.
- Pantothenate antagonist studies. ω-Methylpantothenate (a competitive PANK inhibitor) was administered along with a pantothenate-poor diet in volunteer studies in the 1950s. The syndrome included fatigue, gastrointestinal distress, paresthesias, and characteristic personality changes — confirming that pantothenate is functionally required, even though spontaneous deficiency is virtually never seen.
The Exception: PKAN (PANK2 Mutation)
The one clinical setting where CoA biosynthesis is dramatically disrupted is in Pantothenate Kinase Associated Neurodegeneration (PKAN) — an autosomal recessive neurogenetic disorder caused by mutations in the PANK2 gene. PKAN was previously called Hallervorden-Spatz syndrome before the underlying genetics were discovered. It is part of a broader category called Neurodegeneration with Brain Iron Accumulation (NBIA), and it accounts for roughly half of NBIA cases.
PANK2 is the mitochondrial isoform of pantothenate kinase. When it is non-functional due to homozygous or compound-heterozygous mutations, the mitochondrial CoA pool is depleted in tissues that depend particularly heavily on PANK2 — most notably the globus pallidus in the basal ganglia, where the disease produces its characteristic MRI sign (the "eye of the tiger" pattern: a central region of T2 hyperintensity surrounded by hypointensity from iron accumulation).
Clinical presentation typically begins in childhood or adolescence with progressive dystonia, dysarthria, rigidity, and retinal degeneration. There is no cure. Symptomatic treatments include baclofen and trihexyphenidyl for dystonia; deep brain stimulation has produced benefit in some cases. Experimental therapies targeting the underlying biochemistry are in development:
- Fosmetpantotenate — a pantothenate prodrug designed to bypass the PANK step. Phase III trial (FORT trial) failed to meet its primary efficacy endpoint.
- Pantethine (which sits past the PANK step) — small studies have explored whether high-dose pantethine can partially restore the CoA pool. Results have been mixed.
- PANK1 / PANK3 activators (PANK isoforms unaffected by PANK2 mutation) — in preclinical development.
PKAN is the clinical proof-of-principle that the CoA biosynthesis pathway, while normally robust, can become rate-limiting under genetic disruption — and that the resulting metabolic deficit produces predictable neurodegeneration in the most metabolically demanding regions of the brain.
Absorption & Transport (SMVT)
Dietary pantothenate is absorbed from the small intestine. The transport is mediated by the Sodium-dependent Multivitamin Transporter (SMVT), encoded by the SLC5A6 gene. SMVT is a low-affinity, high-capacity transporter that handles three different B-vitamins: pantothenate, biotin (vitamin B7), and lipoic acid. Because these three vitamins share a transporter, they can competitively interfere with each other's absorption at very high doses — which is the mechanistic basis for the recommendation to add supplemental biotin during chronic high-dose pantothenate or chronic high-dose alpha-lipoic-acid therapy.
In tissues, pantothenate enters cells via SMVT (and, in some specialized tissues, via additional transporters). Once inside, pantothenate is rapidly phosphorylated by PANK to 4'-phosphopantothenate — locking the molecule inside the cell, since the phosphorylated form cannot cross the membrane back out. This is the same general "trap and convert" mechanism the cell uses for many B-vitamins.
Plasma pantothenate concentrations are around 1-2 µM in fasting humans. Total whole-blood concentrations are higher (~5-10 µM) because red blood cells contain CoA. After a high oral dose, plasma pantothenate rises within 1-2 hours and falls back to baseline within 8-12 hours; the urinary excretion of unmetabolized pantothenate increases dose-dependently above the saturable absorption range.
Cautions
- Frank deficiency is extraordinarily rare. Don't supplement pantothenate to "fix" a deficiency that does not exist; pharmacologic-dose pantothenate has different goals (see the acne and adrenal-support deep-dives).
- Biotin competition at SMVT. Chronic high-dose pantothenate (over months at gram-level dosing) may modestly reduce biotin absorption. If you are taking pharmacologic pantothenate long-term, consider a 300-500 µg/day biotin supplement.
- GI side effects at high doses. Gram-level pantothenate often produces mild GI upset, loose stools, or diarrhea — not dangerous, but uncomfortable. Splitting the dose across the day (e.g., 3×1 g rather than 1×3 g) usually reduces the symptoms.
- Pregnancy. No specific risks documented at AI-level intakes (6 mg/day in pregnancy, 7 mg/day in lactation). Pharmacologic doses during pregnancy lack safety data and should be avoided.
- Drug interactions. No significant pharmacokinetic interactions are well-documented at typical pantothenate doses.
Key Research Papers
- Leonardi R, Zhang YM, Rock CO, Jackowski S (2005). Coenzyme A: back in action. Progress in Lipid Research. — PubMed
- Jackowski S, Alix JH (1990). Cloning, sequence, and expression of the pantothenate permease (panF) gene of Escherichia coli. Journal of Bacteriology. — PubMed
- Strauss E, Begley TP (2002). The antibiotic activity of N-pentylpantothenamide results from its conversion to ethyldethia-coenzyme A. Journal of Biological Chemistry. — PubMed
- Hayflick SJ, Westaway SK, Levinson B et al. (2003). Genetic, clinical, and radiographic delineation of Hallervorden-Spatz syndrome. New England Journal of Medicine. — PubMed
- Zhou B, Westaway SK, Levinson B et al. (2001). A novel pantothenate kinase gene (PANK2) is defective in Hallervorden-Spatz syndrome. Nature Genetics. — PubMed
- Daugherty M et al. (2002). Complete reconstitution of the human coenzyme A biosynthetic pathway via comparative genomics. Journal of Biological Chemistry. — PubMed
- Jackowski S, Rock CO (1981). Regulation of coenzyme A biosynthesis. Journal of Bacteriology. — PubMed
- Hong BS et al. (2007). Crystal structures of human pantothenate kinases. Journal of Biological Chemistry. — PubMed
- Said HM (2011). Intestinal absorption of water-soluble vitamins in health and disease. Biochemical Journal. — PubMed
- Maitin V, Said HM (2003). Molecular biology of intestinal pantothenic acid uptake. American Journal of Physiology — Gastrointestinal and Liver Physiology. — PubMed
- Hörl WH et al. (1984). Coenzyme A and ATP in pantothenic acid-deficient rats. European Journal of Biochemistry. — PubMed
- Tahiliani AG, Beinlich CJ (1991). Pantothenic acid in health and disease. Vitamins and Hormones. — PubMed
PubMed Topic Searches
- PubMed: pantothenate kinase regulation
- PubMed: CoA biosynthesis pathway
- PubMed: phosphopantetheine prosthetic group
- PubMed: PKAN pantothenate kinase neurodegeneration
- PubMed: acetyl-CoA TCA cycle
- PubMed: SMVT pantothenate biotin
Connections
- Vitamin B5 Overview
- B5 Benefits Hub
- B5 for Adrenal Support
- B5 for Acne
- Pantethine for Cholesterol
- Pantothenic Acid & Adrenal Health
- Pantothenic Acid & Wound Healing
- Vitamin B1 (Thiamine)
- Vitamin B2 (Riboflavin)
- Vitamin B3 (Niacin)
- Vitamin B7 (Biotin)
- Vitamin B12
- Cysteine
- Alpha Lipoic Acid
- Glutathione
- Magnesium
- Neurology