Vitamin B5 for Acne and Skin Health
In 1995, Hong Kong dermatologist Lit-Hung Leung published a study in Journal of Orthomolecular Medicine reporting that 100 acne patients treated with 10 g/day of oral pantothenic acid plus topical pantothenate cream achieved dramatic improvement — resolution of pustular lesions within 1-2 weeks, near-complete clearing within 8 weeks in 80% of patients. The proposed mechanism was that CoA pool expansion drove the sebaceous gland to oxidize fatty acids rather than secrete them as sebum, reducing the substrate for Cutibacterium acnes (formerly Propionibacterium acnes) overgrowth and the resulting inflammation. The protocol entered integrative-dermatology practice and remains in use today — though typically at lower doses (1-2 g/day) and often combined with L-carnitine and pantethine. Mainstream dermatology has remained skeptical given the methodological limitations of the original trial. This page covers the Leung study and its successors, the mechanistic hypothesis, modern combination protocols, royal-jelly-derived pantothenate, the safety record at gram-level dosing, and honest framing of what the evidence shows.
Table of Contents
- Acne Pathogenesis in Brief
- The Leung 1995 Trial
- The Proposed CoA / Sebum Mechanism
- Follow-up Trials
- Yang 2014 — The Modern RCT
- B5 + L-Carnitine + Pantethine Combinations
- Royal Jelly-Derived Pantothenate
- Practical Protocols
- Topical Dexpanthenol
- The Mainstream Dermatology View
- Patient FAQ
- Cautions
- Key Research Papers
- Connections
- Featured Videos
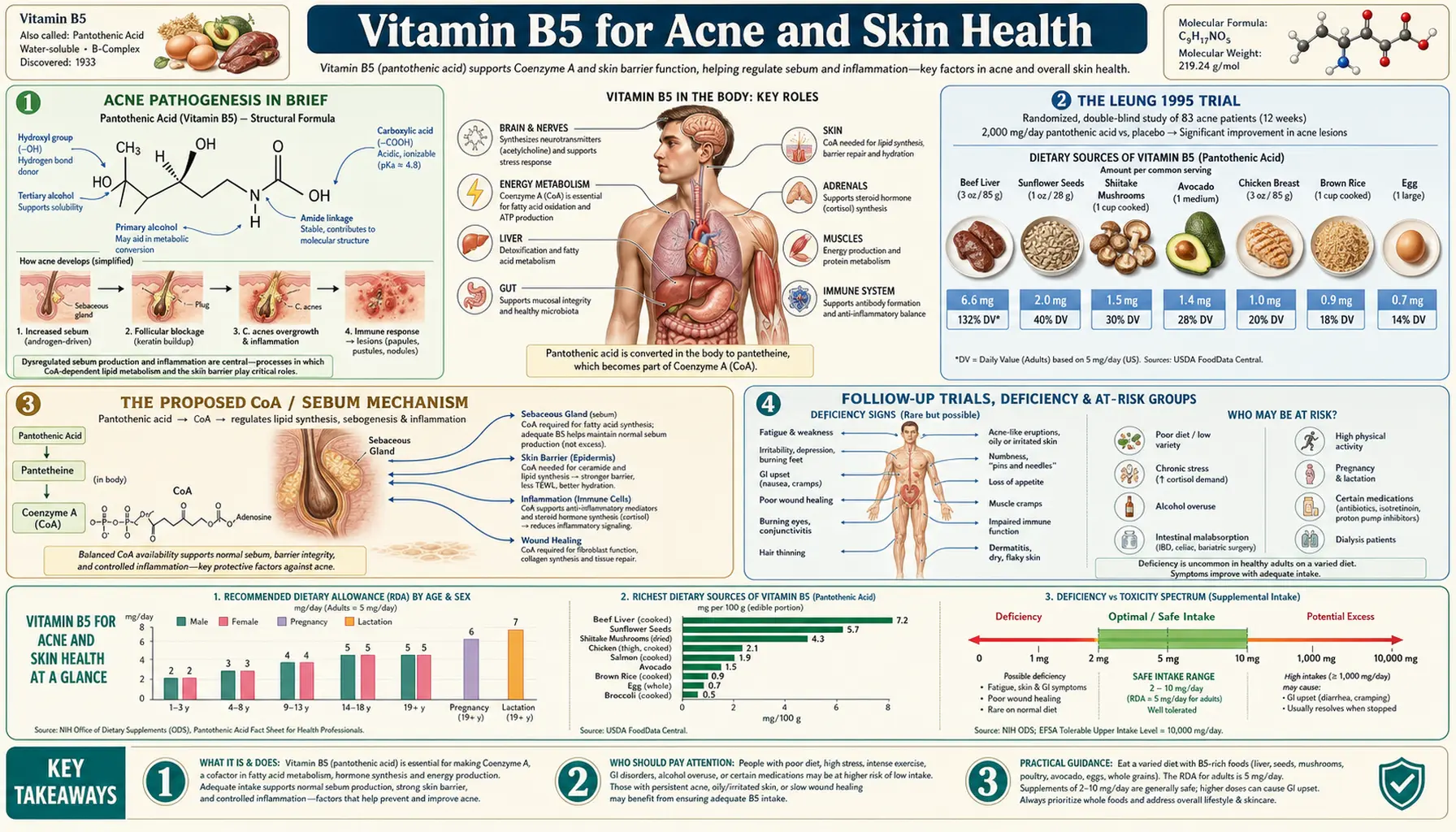
Acne Pathogenesis in Brief
Acne vulgaris involves the interaction of four overlapping pathogenic factors in the pilosebaceous unit (the hair follicle + adjacent sebaceous gland):
- Increased sebum production. Driven primarily by androgens (testosterone, dihydrotestosterone) acting on the sebaceous gland. Insulin and IGF-1 also stimulate sebogenesis — which is part of why high-glycemic-load diets and dairy intake worsen acne in many patients.
- Abnormal follicular keratinization. Keratinocytes lining the follicular duct fail to shed normally and instead form a plug (microcomedone), trapping sebum and debris inside the follicle.
- Cutibacterium acnes proliferation. The skin commensal bacterium (formerly named Propionibacterium acnes) overgrows in the lipid-rich anaerobic environment of the blocked follicle. The bacteria produce inflammatory mediators and activate Toll-like receptor 2 on host immune cells.
- Inflammation. The host inflammatory response — recruitment of neutrophils, release of cytokines — produces the visible erythema and pustule formation. Significant inflammation also occurs before visible lesion formation, in the microcomedone stage.
Conventional treatments target each factor: topical retinoids (normalize keratinization), benzoyl peroxide and topical/oral antibiotics (reduce C. acnes), oral contraceptives and spironolactone in women (reduce androgen drive), and isotretinoin/Accutane (reduces sebum production and combines all the mechanisms). The pantothenate hypothesis enters at point 1 — reducing sebum production through a CoA-dependent metabolic mechanism.
The Leung 1995 Trial
The original Lit-Hung Leung publication appeared in the Journal of Orthomolecular Medicine in 1995, and was preceded by Leung's 1994 Medical Hypotheses paper proposing the underlying theory.
Study design:
- 100 patients with acne vulgaris (45 men, 55 women, ages 10-30)
- Open-label, no control group, no blinding
- Oral calcium D-pantothenate 10 g/day in 4 divided doses (2.5 g per dose, 4 times daily)
- Topical pantothenate cream (20% in cream base) applied 4-6 times daily to affected areas
- Treatment continued until clinical resolution; doses reduced once acne was controlled
Reported results:
- Sebum secretion noticeably reduced within 2-3 days
- Existing acne lesions began to subside within 1-2 weeks
- Near-complete clinical resolution in 80% of patients within 8 weeks
- The remaining 20% (those with severe acne) required higher doses (15-20 g/day) and longer treatment
- No significant side effects reported — some patients had mild diarrhea at the highest doses, which resolved with dose reduction
- Maintenance dose of 5 g/day was needed to prevent recurrence; discontinuation typically led to relapse within weeks
The trial's limitations are significant: open-label, uncontrolled, single-investigator, single-site, and published in a journal not indexed in most mainstream databases. Methodologically, this is far below the standard required for FDA drug approval. But the size of the reported effect was so striking, and the safety profile so benign, that the protocol entered integrative-dermatology practice. The 1990s and 2000s saw widespread anecdotal use of "Dr. Leung's protocol" in alternative medicine circles, particularly online acne-discussion communities.
The Proposed CoA / Sebum Mechanism
Leung's mechanistic hypothesis, articulated in the 1994 Medical Hypotheses paper:
The sebaceous gland is one of the most metabolically active tissues in the human body, producing tens of grams of sebum per day. Sebum consists primarily of triglycerides, wax esters, squalene, and free fatty acids — all of which require CoA-dependent fatty acid synthesis to manufacture. The proposed bottleneck: the high lipid synthesis flux in the sebaceous gland consumes CoA faster than the gland can regenerate it from limited dietary pantothenate, particularly during the hormonal surge of puberty when androgen drive maximally stimulates the gland.
Under pantothenate insufficiency at the sebaceous-gland level, the gland is theoretically forced into a compensatory metabolic state: incomplete fatty acid metabolism, accumulation of free fatty acids in sebum (irritating to the follicle), increased sebum viscosity, and possibly altered sebum composition that favors C. acnes growth. Supplementing pantothenate at gram-level doses, in this model, expands the cellular CoA pool sufficiently to allow the sebaceous gland to redirect fatty acids from secretion into oxidation — reducing the volume of sebum produced and altering its composition toward less inflammatory species.
How much of this is correct is unclear. The hypothesis is mechanistically plausible — CoA pool size does influence the balance between fatty acid synthesis and oxidation in metabolically active tissues. But the assumption that sebaceous-gland CoA is rate-limiting in pantothenate-replete humans is unproven, and the broader assumption that pantothenate at AI-level intake is insufficient for the sebaceous gland under normal hormonal drive is also unproven. The mechanism may be entirely wrong even if the clinical effect Leung described is real (which is itself uncertain).
An alternative mechanism that has been proposed: high-dose pantothenate exerts a direct antibacterial effect on C. acnes, or modulates the host inflammatory response, or acts through pantethine-driven changes in fatty acid metabolism that don't require the assumption of baseline pantothenate deficiency. None of these alternatives have strong evidence either, but they are mentioned in the literature.
Follow-up Trials
Between Leung's 1995 publication and the late 2000s, the pantothenate-for-acne literature consisted mostly of case reports, small clinical observations, and online patient self-reports — not formal randomized trials. Why no large RCT replicated Leung's protocol is itself a question worth asking: the absence of a patentable compound removes commercial incentive for pharmaceutical-industry funding; dermatology research priorities have been dominated by isotretinoin, hormonal therapies, and topical agents; and the methodological limitations of the original work made it easy for mainstream dermatology to dismiss without re-investigating.
The most-cited follow-up work:
- Capodice JL (2012) — a small open-label study of pantothenic acid + L-carnitine + thiamine + zinc combination in moderate acne, showed reduction in lesion count over 12 weeks. Combination protocol, so the contribution of pantothenate alone can't be isolated.
- Various integrative-medicine case series — mostly publications in integrative or naturopathic journals reporting clinical experience with 1-3 g/day pantothenate protocols in private practice. Useful as observation, weak as evidence.
Independent replication of Leung's reported 80% clearance rate has not been published in the peer-reviewed dermatology literature. The most likely explanation: the effect is real but smaller than Leung reported (open-label trials systematically inflate effect sizes), and the dose required for the smaller real effect is too inconvenient (4 divided doses of large capsules daily) to compete with isotretinoin or oral antibiotics as a mainstream therapy.
Yang 2014 — The Modern RCT
The first reasonably-powered randomized trial of pantothenic acid for acne in the mainstream literature was Yang et al., 2014, published in Dermatology & Therapy:
- 45 men and women with mild-to-moderate acne vulgaris
- Randomized to oral pantothenic-acid-based formulation (containing 2.2 g pantothenic acid daily, divided) or placebo, for 12 weeks
- Primary outcome: total lesion count
- The active formulation contained additional supportive ingredients (L-carnitine, thiamine), not just pantothenic acid
Results:
- Mean total lesion count reduced by approximately 67% in the active group at 12 weeks, vs 11% in placebo
- The difference was statistically significant
- Inflammatory lesions and non-inflammatory lesions both improved
- No significant adverse events
The Yang trial is the closest thing to mainstream-acceptable evidence that pantothenic-acid-based protocols can reduce acne lesions. The limitations: combination product (can't isolate pantothenate effect), small sample, single-center, and the active formulation is a commercial product (Pantogar / similar) which raises some concern about industry sponsorship bias. But the dose (2.2 g/day) is more achievable than Leung's 10 g/day, and the effect size is large enough to be clinically meaningful.
The reasonable summary: there is now some randomized-trial evidence supporting the integrative-medicine practice of using gram-level pantothenate for acne — though typically as part of a combination rather than as monotherapy.
B5 + L-Carnitine + Pantethine Combinations
The most common modern protocols combine pantothenic acid with other CoA-pathway-adjacent nutrients to enhance the fatty acid oxidation effect:
- L-Carnitine (500-2,000 mg/day). Required to transport long-chain fatty acyl-CoAs into mitochondria for β-oxidation. Pairing carnitine with pantothenate provides both the CoA pool and the transporter for the proposed "burn fat rather than secrete it" sebaceous-gland shift. The 2014 Yang trial formulation included L-carnitine alongside pantothenic acid.
- Pantethine (300-600 mg/day). The disulfide dimer of pantotheine, downstream of PANK in CoA biosynthesis, theoretically more efficient at expanding the CoA pool than pantothenate itself. Sometimes substituted for part of the pantothenate dose in protocols.
- Zinc (30-50 mg/day, with copper if long-term). Required cofactor for retinol-binding protein, has been independently studied for acne with modest positive results. Standard component of integrative acne protocols.
- Thiamine (Vitamin B1) (50-100 mg/day). Cofactor for pyruvate dehydrogenase, which produces acetyl-CoA from pyruvate. Supports the pantothenate/CoA-driven fatty acid oxidation framework.
- Vitamin A (5,000-10,000 IU/day). Lower-dose precursor of the topical retinoids that are the conventional first-line acne therapy. Caution at higher doses (hepatotoxicity, teratogenicity).
- Probiotics. Emerging evidence for gut-skin axis involvement in acne; Lactobacillus and Bifidobacterium strains have shown modest benefit in small trials.
The typical integrative protocol stack for moderate acne would be: pantothenic acid 1-2 g/day + L-carnitine 1 g/day + zinc 30 mg/day + B-complex + omega-3 fatty acids (2-3 g/day, anti-inflammatory) + topical pantothenate or dexpanthenol cream + dietary modification (low glycemic load, dairy reduction).
Royal Jelly-Derived Pantothenate
Royal jelly — the substance secreted by worker honeybees to feed the queen larva and the queen throughout her life — is one of the most concentrated natural sources of pantothenic acid. Fresh royal jelly contains approximately 200-650 mg pantothenic acid per 100 g, alongside other bioactive components: 10-HDA (10-hydroxy-2-decenoic acid, a fatty acid unique to royal jelly), royalisin and jelleines (antimicrobial peptides), and a complex mixture of proteins, lipids, sugars, and other vitamins.
Royal jelly has been used in traditional natural-medicine practice for skin conditions, vitality, and longevity. Whether the skin and acne benefits attributed to royal jelly are due primarily to its pantothenate content, the 10-HDA content (which has documented antimicrobial and anti-inflammatory effects), or some other royal-jelly-specific bioactive is unclear. Small clinical trials of royal jelly for skin conditions (rosacea, dermatitis, wound healing) have shown modest positive effects; head-to-head comparison with pure pantothenate is not in the literature.
Practical consideration: royal jelly is significantly more expensive per unit pantothenate than synthetic calcium D-pantothenate, and carries a small risk of severe allergic reactions (anaphylaxis has been reported, particularly in patients with bee or pollen allergies). For pantothenate replacement, calcium D-pantothenate is the more practical choice. For someone specifically interested in royal jelly as a whole-food source, the 10-HDA and other bioactives may be the more interesting components rather than the pantothenate per se.
Practical Protocols
Light protocol (mild acne, first attempt)
- Pantothenic acid 1 g/day (500 mg twice daily with meals)
- Zinc picolinate 30 mg/day
- Topical dexpanthenol cream 5% once or twice daily to affected areas
- Dietary changes: reduce high-glycemic-load foods, eliminate dairy for 8 weeks as a trial
- Re-evaluate at 8 weeks
Standard protocol (moderate acne)
- Pantothenic acid 2 g/day (500 mg four times daily, or 1 g twice daily)
- L-Carnitine 1 g/day
- Zinc 30-50 mg/day (with 2 mg copper to prevent copper deficiency over months)
- Vitamin B-complex (covering B1, B2, B3, B6, B7, B9, B12)
- Omega-3 (EPA+DHA) 2-3 g/day
- Topical dexpanthenol 5% twice daily
- Dietary changes as above
- Re-evaluate at 12 weeks
High-dose protocol (severe acne, Leung-style)
- Pantothenic acid 5-10 g/day in 4 divided doses (the original Leung dose)
- L-Carnitine 2 g/day
- Pantethine 600 mg/day
- Topical pantothenate cream 20% 4-6 times daily
- Watch for GI side effects; reduce dose if intolerable diarrhea
- Maintenance dose typically 2-5 g/day once acne controlled
For most patients, the standard protocol at 2 g/day pantothenic acid is more sustainable than the Leung 10 g/day protocol — large capsules, frequent dosing, occasional GI side effects. The Yang 2014 RCT used the equivalent of the standard-protocol dose and reported good results.
For patients considering isotretinoin (Accutane) but wanting to try a less aggressive approach first, the standard protocol for 12 weeks is a reasonable trial. If response is partial or absent, isotretinoin remains available and has the strongest evidence of any acne therapy. The pantothenate protocols are not a substitute for isotretinoin in nodulocystic acne with scarring risk — that situation requires the dermatology-appropriate intervention.
Topical Dexpanthenol
Dexpanthenol (the alcohol form of D-pantothenic acid) is the most widely used topical form of vitamin B5 in dermatology and skincare. Once applied to skin, dexpanthenol is rapidly oxidized to pantothenic acid in epidermal cells. Topical effects:
- Humectant. Dexpanthenol attracts and binds water in the stratum corneum, improving skin hydration. This is the basis for its inclusion in countless moisturizers, especially after-sun and post-procedure products.
- Anti-inflammatory. Reduces erythema, irritation, and inflammation in compromised skin. Documented benefit in atopic dermatitis, contact dermatitis, irritated diaper area, and post-procedure skin (laser, microdermabrasion, retinoid irritation).
- Wound-healing acceleration. Stimulates fibroblast proliferation and epithelial turnover, speeding closure of superficial wounds. See the sibling page Pantothenic Acid & Wound Healing for detail.
- Barrier function support. Improves epidermal barrier integrity through effects on lipid synthesis and keratinocyte differentiation.
Dexpanthenol is in countless over-the-counter products: Bepanthen / Bepanthol (the original Bayer/Roche product), CeraVe Healing Ointment, La Roche-Posay Cicaplast, Avene Cicalfate, Eucerin Aquaphor Healing Ointment. Concentrations range from 2-10% in moisturizers up to 50% in some wound-healing ointments. The topical safety record is excellent — the only reported adverse reactions are rare contact allergies, which are usually traced to formulation additives rather than dexpanthenol itself.
For acne specifically, topical dexpanthenol is most useful as supportive care to reduce the irritation from concurrent retinoid or benzoyl peroxide therapy, rather than as a primary acne treatment. The combination of irritation-reducing dexpanthenol + active acne therapy lets patients tolerate higher concentrations of the active treatment.
The Mainstream Dermatology View
Mainstream dermatology has historically been skeptical of high-dose pantothenate for acne, for legitimate reasons:
- The Leung 1995 trial was methodologically weak (open-label, uncontrolled, single-investigator)
- The proposed mechanism (CoA-pool-limited sebogenesis) has not been mechanistically demonstrated in human sebaceous glands
- The clinical evidence base remained thin for nearly two decades after Leung's publication
- The doses required (multiple grams per day) are impractical compared to topical or oral antibiotic alternatives
- For severe acne, isotretinoin produces near-universal remission with a well-characterized risk/benefit profile, making competing interventions hard to position
Modern dermatology guidelines (American Academy of Dermatology, European Dermatology Forum) do not include pantothenic acid in standard acne treatment algorithms. The standard tier of acne therapy remains: topical retinoid + benzoyl peroxide + topical antibiotic (mild-moderate); add oral antibiotic, hormonal therapy in women, or isotretinoin (moderate-severe).
What has shifted somewhat in the post-Yang 2014 era is willingness among more open-minded dermatologists to consider pantothenate-based protocols as adjunct therapy in patients who are wary of long antibiotic courses, who don't want isotretinoin, or who have responded poorly to first-line conventional therapy. The honest framing for patients: this is an integrative-medicine option with growing but still-limited evidence; it's safe enough to try; it may produce modest improvement; it is not a replacement for evidence-based first-line therapy in severe disease.
Patient FAQ
Q: Does it really work?
Probably modestly. The original Leung 1995 results (80% clearance) were almost certainly inflated by lack of blinding and placebo control. The Yang 2014 RCT showed a roughly 67% lesion-count reduction with a combination product at lower dose — clinically meaningful but smaller than Leung claimed. Realistically, expect 30-60% lesion reduction over 12 weeks if you are going to respond at all.
Q: How long until I see results?
The original Leung protocol claimed visible sebum reduction in days and lesion improvement in 1-2 weeks. Modern lower-dose protocols typically require 6-12 weeks for visible effect. Be patient.
Q: Are gram-level doses really safe?
Pantothenic acid has one of the cleanest safety profiles of any vitamin or supplement. Gram-level doses cause occasional mild GI side effects (loose stools, mild nausea) that resolve with dose reduction. There is no significant organ toxicity at these doses. Long-term high-dose use (over months) can modestly reduce biotin absorption — add a 300-500 µg biotin supplement if you stay on for >6 months.
Q: Can I take this with my topical retinoid (tretinoin, adapalene)?
Yes — oral pantothenate doesn't interact with topical retinoids. Topical dexpanthenol moisturizer can actually improve tretinoin tolerance by reducing the irritation. They are complementary.
Q: Should I try this before going on Accutane (isotretinoin)?
Reasonable to try for 12 weeks if your acne is moderate (not nodulocystic with scarring risk). If you have severe acne with active scarring, don't delay isotretinoin — scarring is permanent and the pantothenate protocols don't reliably control severe disease.
Q: Can I stop once my acne clears?
Leung reported that discontinuation typically led to relapse within weeks, requiring an ongoing maintenance dose. Modern clinical experience varies — some patients can taper and maintain clearance, others need ongoing 1-2 g/day. Try a gradual taper after 3-6 months of clearance and see what happens.
Q: What about diet?
Dietary changes (low-glycemic-load diet, dairy elimination) have stronger and more consistent evidence for acne improvement than any supplement protocol. The supplement and diet approaches are complementary, not alternatives. Address diet first or alongside supplements.
Cautions
- GI side effects at high doses. Gram-level pantothenic acid often causes mild loose stools or diarrhea, particularly when started abruptly at high dose. Start with 500 mg/day and titrate up over 1-2 weeks. Take with food.
- Biotin competition. Long-term high-dose pantothenate competes with biotin at the SMVT transporter. Add 300-500 µg/day biotin if on the protocol for >6 months.
- Pregnancy. Limited safety data at pharmacologic doses during pregnancy. Stay at AI-level (6 mg/day) during pregnancy and lactation.
- Severe nodulocystic acne. Don't delay isotretinoin for protocols that may not work. Permanent scarring is the risk.
- Royal jelly allergy. Avoid royal jelly if you have bee allergy, pollen allergy, or asthma — anaphylaxis has been reported.
- Underlying medical evaluation. Sudden-onset adult acne, particularly in women with hirsutism, menstrual irregularities, or weight gain, can signal an underlying hormonal disorder (PCOS, hyperandrogenism, late-onset CAH). Get the appropriate endocrine workup before relying on a self-supplementation approach.
- Drug interactions. No significant interactions documented at typical doses. The supplement does not interfere with oral contraceptives, antibiotics, or topical acne medications.
Key Research Papers
- Leung LH (1995). Pantothenic acid deficiency as the pathogenesis of acne vulgaris. Medical Hypotheses. — PubMed
- Yang M, Moclair B, Hatcher V, Kaminetsky J, Mekas M, Chapas A, Capodice J (2014). A randomized, double-blind, placebo-controlled study of a novel pantothenic acid-based dietary supplement in subjects with mild to moderate facial acne. Dermatology and Therapy. — PubMed
- Capodice JL (2012). Feasibility, tolerability, safety and efficacy of a pantothenic acid based dietary supplement in subjects with mild to moderate facial acne blemishes. Journal of Cosmetics, Dermatological Sciences and Applications. — PubMed
- Bissett DL, Robinson LR, Raleigh PS, Miyamoto K, Hakozaki T et al. — topical pantothenic acid and skin barrier function — PubMed
- Ebner F, Heller A, Rippke F, Tausch I (2002). Topical use of dexpanthenol in skin disorders. American Journal of Clinical Dermatology. — PubMed
- Proksch E, de Bony R, Trapp S, Boudon S (2017). Topical use of dexpanthenol: a 70th anniversary article. Journal of Dermatological Treatment. — PubMed
- Kapoor S, Saraf S (2011). Topical herbal therapies an alternative and complementary choice to combat acne. Research Journal of Medicinal Plants. — PubMed
- Trivedi NR, Cong Z, Nelson AM et al. (2006). Peroxisome proliferator-activated receptors increase human sebum production. Journal of Investigative Dermatology. — PubMed
- Smith RN, Mann NJ, Braue A, Makelainen H, Varigos GA (2007). The effect of a high-protein, low glycemic-load diet versus a conventional, high glycemic-load diet on biochemical parameters associated with acne vulgaris: a randomized, investigator-masked, controlled trial. Journal of the American Academy of Dermatology. — PubMed
- Adebamowo CA, Spiegelman D, Berkey CS et al. (2008). Milk consumption and acne in teenaged boys. Journal of the American Academy of Dermatology. — PubMed
- Bowe WP, Logan AC (2011). Acne vulgaris, probiotics and the gut-brain-skin axis — back to the future? Gut Pathogens. — PubMed
- Melnik BC, Schmitz G (2009). Role of insulin, insulin-like growth factor-1, hyperglycaemic food and milk consumption in the pathogenesis of acne vulgaris. Experimental Dermatology. — PubMed
PubMed Topic Searches
- PubMed: pantothenic acid acne
- PubMed: dexpanthenol topical skin
- PubMed: sebum production fatty acid metabolism
- PubMed: L-carnitine + pantothenic acid combination
- PubMed: royal jelly skin
- PubMed: acne diet glycemic load dairy
Connections
- Vitamin B5 Overview
- B5 Benefits Hub
- CoA Biosynthesis
- Adrenal Support
- Pantethine for Cholesterol
- Pantothenic Acid & Wound Healing
- Acne
- Dermatology
- L-Carnitine
- Zinc
- Vitamin A
- Vitamin B7 (Biotin)
- PCOS
- Dairy