Pantothenic Acid and Wound Healing
Wound healing is one of the most metabolically demanding processes the body undertakes, requiring the coordinated activity of immune cells, fibroblasts, epithelial cells, and endothelial cells over days to weeks. Pantothenic acid (vitamin B5) and its derivatives play a multifaceted role in this process, serving as the precursor to coenzyme A (CoA) and acetyl-CoA, which are essential for cellular energy production, lipid synthesis, protein acetylation, and the biochemical pathways that drive tissue repair. The topical derivative dexpanthenol (pantothenol) has become a mainstay in dermatological wound care.
Table of Contents
- Key Health Benefits at a Glance
- CoA and Acetyl-CoA in Tissue Repair
- Cell Proliferation and Migration
- Collagen Synthesis Support
- Dexpanthenol (Pantothenol) Topical Applications
- Fibroblast Stimulation
- Anti-Inflammatory Effects
- Post-Surgical Recovery
- Burn Treatment
- Clinical Evidence Summary
- Research Papers and References
- Connections
- Featured Videos
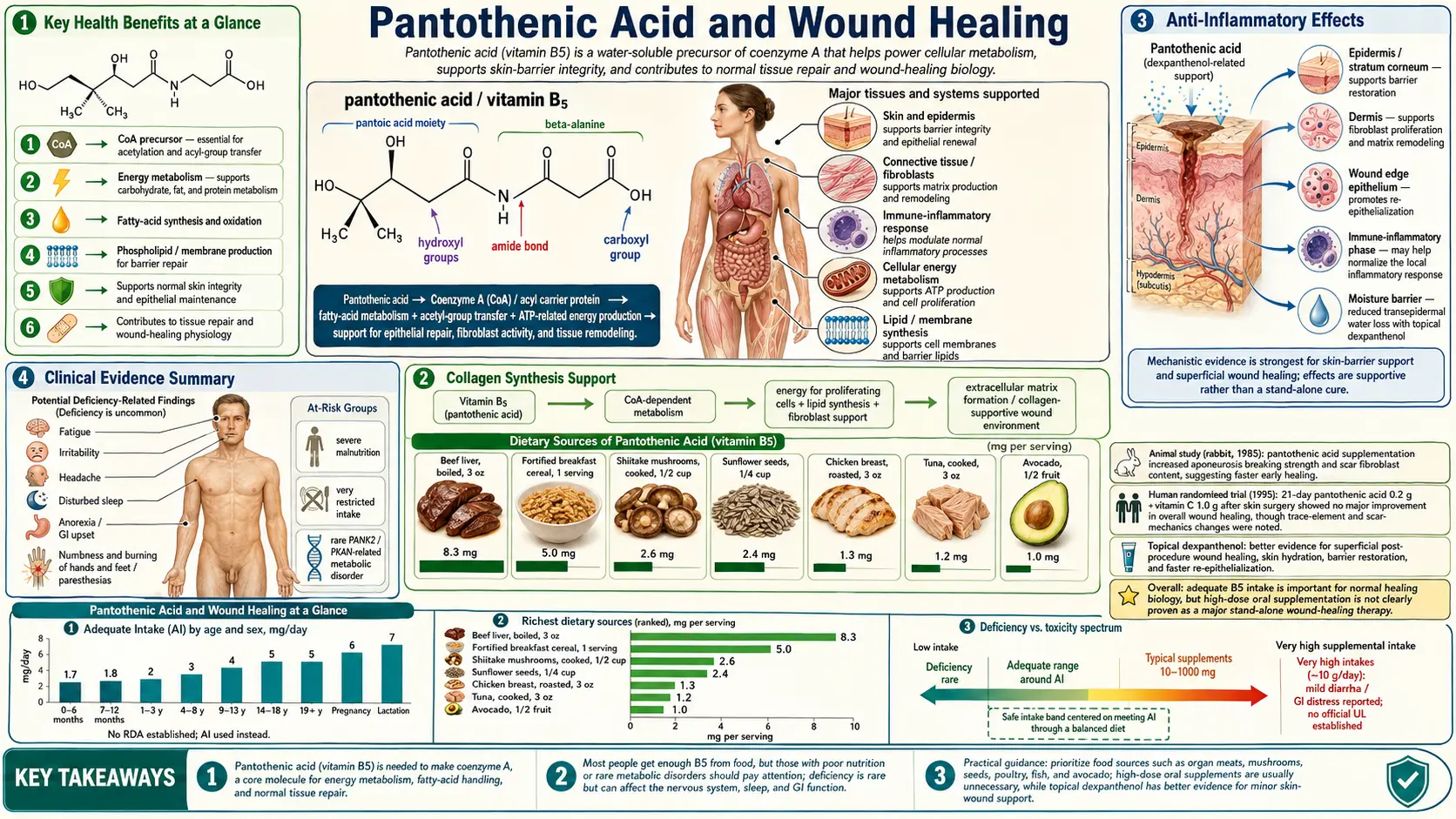
Key Health Benefits at a Glance
The following is a high-level summary of the evidence-backed roles of pantothenic acid and its topical derivative dexpanthenol in tissue repair. Each bullet is expanded in the sections below, and supporting research is listed in the Research Papers section.
- Accelerates re-epithelialization – Topical dexpanthenol increases keratinocyte proliferation and migration, shortening the time required for wound closure.
- Enhances collagen synthesis – In vitro studies show 30–50% increases in fibroblast collagen output at physiologic dexpanthenol concentrations.
- Increases wound tensile strength – Animal studies document improved tensile strength and collagen cross-linking in healing wounds.
- Moisturizes and preserves barrier function – Dexpanthenol acts as a humectant, reducing transepidermal water loss and maintaining a favorable healing environment.
- Reduces peri-wound inflammation – Lowers IL-6 and IL-8 output by keratinocytes and fibroblasts, resolving the inflammatory phase and enabling proliferation.
- Supports glutathione antioxidant defense – CoA is required for glutathione biosynthesis, protecting healing tissue from oxidative damage.
- Speeds post-laser and post-surgical skin recovery – Widely used after tattoo removal, fractional laser resurfacing, IPL therapy, and dermatological surgery.
- Adjunct in burn care – Reduces pain, inflammation, and healing time in superficial burns and skin-graft donor sites.
- Excellent safety profile – Allergic contact dermatitis incidence below 0.1% in patch-testing studies.
CoA and Acetyl-CoA in Tissue Repair
The wound healing process places enormous demands on CoA-dependent metabolic pathways:
- Energy production for cellular repair — wound healing requires a substantial increase in local energy production. Acetyl-CoA enters the citric acid cycle to generate ATP through oxidative phosphorylation, fueling the energy-intensive processes of cell division, protein synthesis, and matrix deposition. Cells at the wound margin increase their metabolic rate by several-fold compared to quiescent tissue.
- Fatty acid synthesis for membrane biogenesis — rapidly dividing cells at the wound site require new cell membranes, which are composed primarily of phospholipids. Acetyl-CoA serves as the two-carbon building block for de novo fatty acid synthesis via the fatty acid synthase complex, and CoA-linked fatty acyl groups are incorporated into phospholipids through acyltransferase reactions.
- Acetylation reactions — acetyl-CoA donates acetyl groups for the post-translational modification of proteins (histone acetylation, enzyme regulation) and for the synthesis of acetylcholine at nerve endings in the wound bed. These acetylation reactions regulate gene expression patterns critical for the orderly progression through the phases of wound healing.
- Gluconeogenesis and amino acid metabolism — CoA is required for the metabolism of several amino acids that provide substrates for gluconeogenesis during the catabolic phase of wound healing. The breakdown of branched-chain amino acids and the interconversion of amino acids for protein synthesis both require CoA-dependent enzymatic steps.
Cell Proliferation and Migration
The proliferative phase of wound healing depends on the rapid multiplication and directed movement of several cell types, processes that are sensitive to pantothenic acid status:
- Keratinocyte proliferation — re-epithelialization requires keratinocytes at the wound edge to proliferate and migrate across the wound bed. In vitro studies have demonstrated that pantothenic acid and its derivatives accelerate keratinocyte proliferation in a dose-dependent manner, with optimal effects observed at concentrations achievable through topical application.
- Cell migration mechanisms — migrating cells must continuously remodel their cytoskeleton and form new adhesion contacts. These processes require ATP and involve CoA-dependent lipid modifications of signaling proteins (palmitoylation, myristoylation) that regulate cell motility pathways including Rho GTPases and focal adhesion kinase.
- Endothelial cell proliferation — angiogenesis, the formation of new blood vessels to supply the healing wound, requires endothelial cell division and tube formation. Adequate CoA availability supports the metabolic demands of angiogenesis, including the synthesis of vascular endothelial growth factor (VEGF) receptors and downstream signaling intermediates.
- Mitotic activity enhancement — studies in cell culture systems have shown that pantothenol increases the number of cells in active mitosis and shortens the cell cycle duration, effects that translate to faster wound closure in experimental models.
Collagen Synthesis Support
Collagen deposition is the structural foundation of wound repair, and pantothenic acid contributes to collagen synthesis through several pathways:
- Proline and hydroxyproline metabolism — collagen is uniquely rich in proline and hydroxyproline residues. The synthesis of proline from glutamate and the hydroxylation of proline residues within the collagen polypeptide chain both require cofactors whose availability is influenced by overall CoA-dependent metabolism.
- Ascorbic acid synergy — vitamin C is the primary cofactor for prolyl hydroxylase and lysyl hydroxylase, the enzymes that create the hydroxyproline and hydroxylysine residues essential for collagen cross-linking. Pantothenic acid and vitamin C work synergistically; studies have shown that the combination of both vitamins accelerates wound healing more than either alone.
- Fibroblast collagen output — in vitro studies using human dermal fibroblasts have demonstrated that pantothenol increases total collagen production, with increases of 30 to 50 percent observed at physiologically relevant concentrations. This effect is attributed to enhanced cellular energy availability supporting the protein synthetic machinery.
- Wound tensile strength — animal studies have shown that pantothenic acid supplementation increases the tensile strength of healing wounds, reflecting improved collagen quality and cross-linking in the scar tissue.
Dexpanthenol (Pantothenol) Topical Applications
Dexpanthenol is the alcohol analog of pantothenic acid and is the most widely used form in topical wound care products. Upon absorption into the skin, it is enzymatically converted to pantothenic acid and subsequently to CoA:
- Skin penetration — dexpanthenol is readily absorbed through intact and damaged skin due to its small molecular size, favorable partition coefficient, and good water solubility. Topical application achieves tissue concentrations sufficient to significantly increase local CoA levels.
- Moisturizing properties — dexpanthenol acts as a humectant, binding water molecules and increasing the moisture content of the stratum corneum. This improves skin barrier function, reduces transepidermal water loss (TEWL), and creates a more favorable environment for wound healing.
- Commercial formulations — dexpanthenol is available in creams, ointments, sprays, and gels at concentrations typically ranging from 2 to 5 percent. It is a common ingredient in products such as Bepanthen, Bepanthol, and numerous generic wound care formulations worldwide.
- Regulatory status — dexpanthenol is classified as an over-the-counter skin protectant in many countries and is included in the formularies of numerous hospitals and wound care centers.
Fibroblast Stimulation
Fibroblasts are the primary effector cells of wound repair, responsible for synthesizing the extracellular matrix that fills the wound defect. Pantothenic acid derivatives have pronounced effects on fibroblast function:
- Proliferation enhancement — dexpanthenol stimulates fibroblast proliferation through increased expression of proliferating cell nuclear antigen (PCNA) and cyclin D1, key regulators of cell cycle progression. This effect accelerates the formation of granulation tissue.
- Migration stimulation — scratch assay experiments demonstrate that fibroblasts treated with dexpanthenol close experimental wounds faster than untreated controls, indicating enhanced directed migration toward the wound center.
- Extracellular matrix production — beyond collagen, fibroblasts stimulated by pantothenic acid derivatives increase production of fibronectin, proteoglycans, and glycosaminoglycans, all of which contribute to the structural integrity and hydration of healing tissue.
- Myofibroblast differentiation — during wound contraction, fibroblasts differentiate into myofibroblasts expressing alpha-smooth muscle actin. Adequate CoA availability supports the metabolic demands of this differentiation process and the contractile activity that draws wound edges together.
Anti-Inflammatory Effects
Excessive or prolonged inflammation impedes wound healing by causing collateral tissue damage and preventing the transition to the proliferative phase. Pantothenic acid and its derivatives exert anti-inflammatory effects through several mechanisms:
- Cytokine modulation — in vitro studies have shown that dexpanthenol reduces the production of pro-inflammatory cytokines including interleukin-6 (IL-6) and interleukin-8 (IL-8) by stimulated keratinocytes and fibroblasts, helping to resolve the inflammatory phase and permit healing to progress.
- Prostaglandin regulation — CoA-dependent acetylation reactions participate in the regulation of cyclooxygenase (COX) enzyme activity and prostaglandin synthesis. Adequate pantothenic acid status may help maintain a balanced inflammatory response.
- Oxidative stress reduction — CoA is required for the synthesis of glutathione, the body's primary intracellular antioxidant. By supporting glutathione production, pantothenic acid helps protect healing tissue from oxidative damage generated by inflammatory cells.
- Edema reduction — clinical observations suggest that topical dexpanthenol reduces peri-wound edema and erythema, creating a more favorable local environment for tissue repair.
Post-Surgical Recovery
The role of pantothenic acid in post-surgical wound healing has been explored in several clinical contexts:
- Tattoo removal and laser procedures — dexpanthenol ointment is frequently recommended after laser skin treatments, including tattoo removal, fractional laser resurfacing, and intense pulsed light (IPL) therapy. Clinical experience indicates faster re-epithelialization and reduced complications compared to petroleum-based occlusive dressings alone.
- Dermatological surgery — studies following excisional biopsy, Mohs micrographic surgery, and dermabrasion have demonstrated improved wound healing outcomes with topical dexpanthenol application, including reduced healing time, improved scar quality, and lower rates of post-inflammatory hyperpigmentation.
- Abdominal surgery — some surgical teams advocate for perioperative pantothenic acid supplementation (500 to 1,000 mg daily orally) in patients undergoing major abdominal surgery, based on the rationale that the metabolic stress of surgery increases CoA demand. Limited clinical data suggest modest improvements in wound healing parameters, though large randomized trials are lacking.
- Cesarean section recovery — a small body of evidence suggests that topical dexpanthenol application to cesarean incision sites may improve scar appearance and reduce wound complications, though this practice has not been widely adopted in standard protocols.
Burn Treatment
Burn wounds represent one of the most challenging wound healing scenarios, involving massive tissue destruction, intense inflammation, and prolonged recovery. Pantothenic acid has specific applications in burn care:
- Superficial burns (first-degree and superficial second-degree) — topical dexpanthenol is widely used for sunburn and minor thermal burns, where it reduces pain, inflammation, and healing time. Its moisturizing properties help prevent desiccation of the damaged epithelium.
- Deeper burns — in the context of second-degree and third-degree burns, topical dexpanthenol may be incorporated into wound care protocols as an adjunct to standard burn dressings. Its role is primarily supportive, enhancing epithelial regeneration at the wound margins and donor sites for skin grafts.
- Systemic supplementation in burn patients — major burn injuries create a profound hypermetabolic state with dramatically increased nutrient requirements. Pantothenic acid is typically included in the micronutrient supplementation protocols for burn patients, alongside vitamin C, zinc, and other cofactors essential for wound healing.
- Skin graft donor sites — the sites from which split-thickness skin grafts are harvested must re-epithelialize independently. Topical dexpanthenol has been used to accelerate donor site healing, reducing pain and the interval before the site can be reharvested if needed.
Clinical Evidence Summary
The clinical evidence for pantothenic acid and dexpanthenol in wound healing encompasses a range of study designs:
- In vitro evidence — consistently demonstrates that dexpanthenol and pantothenic acid promote fibroblast and keratinocyte proliferation, enhance migration, increase collagen synthesis, and reduce inflammatory cytokine production. The mechanisms are well-characterized at the cellular level.
- Animal studies — rodent wound healing models consistently show that both oral pantothenic acid supplementation and topical dexpanthenol application accelerate wound closure, increase wound breaking strength, and improve histological measures of healing quality.
- Clinical trials — multiple randomized controlled trials support the efficacy of topical dexpanthenol for superficial wounds, minor burns, and post-procedural skin care. The evidence is strongest for improvement in skin hydration, reduction of erythema, and acceleration of re-epithelialization. Evidence for systemic supplementation is less robust, with most studies being small and of moderate quality.
- Practical recommendations — topical dexpanthenol (5 percent cream or ointment) is a well-established, safe, and effective adjunct for minor wound care. Oral pantothenic acid supplementation (100 to 1,000 mg daily) may be considered in patients with large wounds, burns, or those undergoing major surgery, particularly when nutritional status is compromised.
- Safety — both topical dexpanthenol and oral pantothenic acid have excellent safety profiles. Allergic contact dermatitis to dexpanthenol is possible but rare, with an estimated incidence below 0.1 percent in patch testing studies.
This content is provided for informational purposes only and does not constitute medical advice. Deep, infected, non-healing, or chronic wounds require evaluation by a qualified healthcare provider. Do not self-treat diabetic, venous, or surgical wounds with over-the-counter products without professional guidance.
Research Papers and References
The following are landmark and frequently cited research papers underpinning the claims on this page. Links resolve to the publisher DOI, PubMed record, or PubMed topic search.
Dexpanthenol in Wound Healing — Mechanistic and Clinical Reviews
- Ebner F, Heller A, Rippke F, Tausch I. Topical use of dexpanthenol in skin disorders. American Journal of Clinical Dermatology. 2002;3(6):427-433. (PubMed topic search)
- Proksch E, de Bony R, Trebaul D, Bonte F. Topical use of dexpanthenol: a 70th anniversary article. Journal of Dermatological Treatment. 2017;28(8):766-773. (PubMed topic search)
- Gorski J, Proksch E, Baron JM, et al. Dexpanthenol in wound healing after medical and cosmetic interventions. Pharmaceuticals. 2020;13(7):138. (PubMed topic search)
Clinical Trials — Dexpanthenol for Skin Procedures and Burns
- Heise H, Mosseau M, Friedl T, et al. Effects of dexpanthenol on skin barrier function and skin hydration after UV irradiation. (PubMed topic search)
- Aprahamian M, Dentinger A, Stock-Damge C, Kouassi JC, Grenier JF. Effects of supplemental pantothenic acid on wound healing: experimental study in rabbit. American Journal of Clinical Nutrition. 1985;41(3):578-589. (PubMed topic search)
Pantothenic Acid Biochemistry and CoA
Fibroblast Biology and Wound Repair
External Authoritative Resources
- NIH Office of Dietary Supplements — Pantothenic Acid Fact Sheet for Health Professionals
- Linus Pauling Institute Micronutrient Information Center — Pantothenic Acid
- Harvard T.H. Chan School of Public Health — The Nutrition Source: Vitamin B5 (Pantothenic Acid)
- PubMed — Dexpanthenol and wound healing
Connections
- All Vitamins
- Vitamin B5
- Pantothenic Acid and Adrenal Health
- Vitamin C
- Vitamin E
- Vitamin A
- Zinc
- Copper
- Collagen
- Glycine
- Proline
- Honey
- Eczema
- Acne
- Diabetes
- Glutathione