Pantethine for Cholesterol and Lipid Management
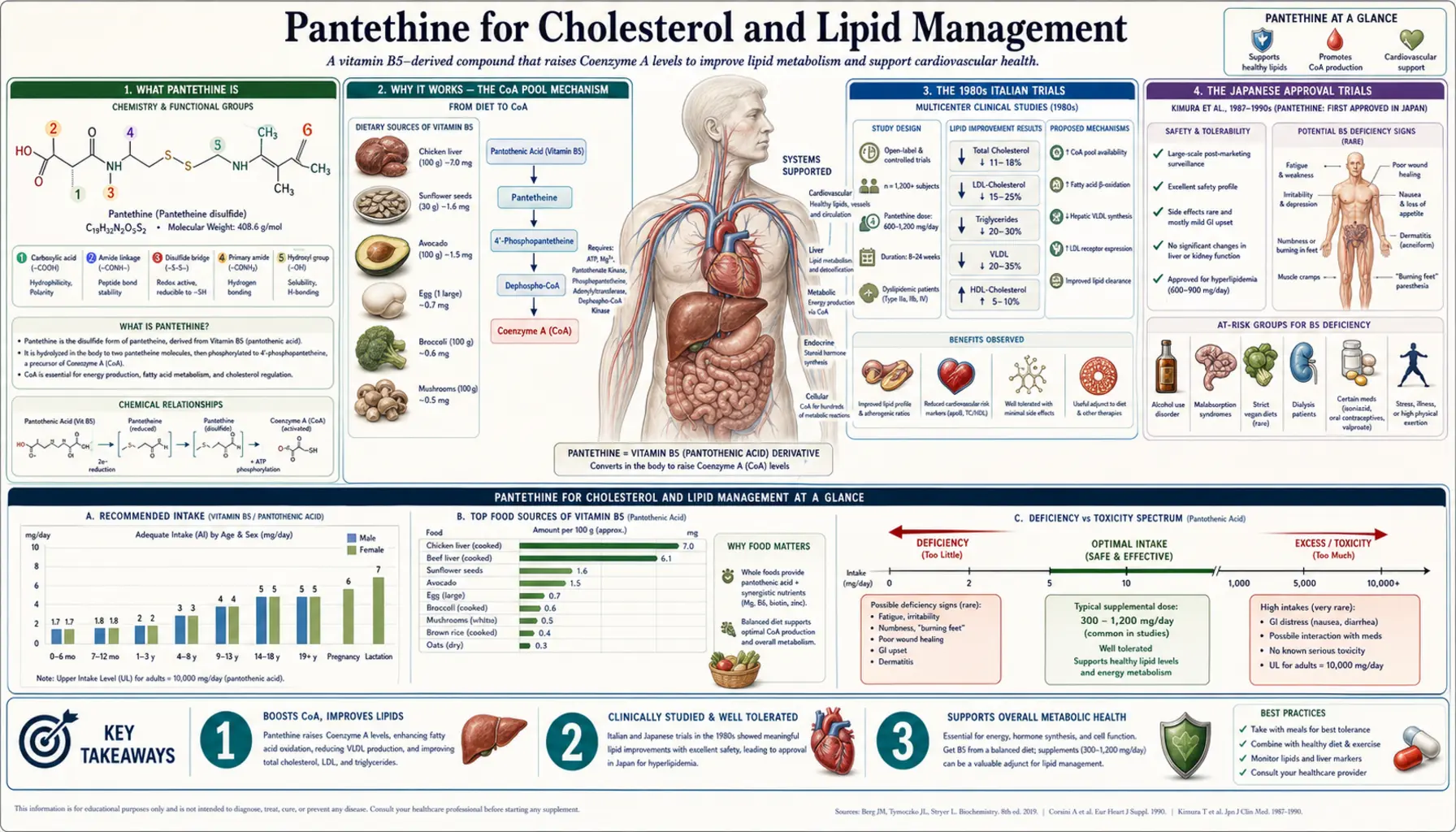
Pantethine is the disulfide dimer of pantotheine, a biosynthetic intermediate that sits one step past PANK (the rate-limiting enzyme of CoA biosynthesis) in the pathway from pantothenate to Coenzyme A. Because it bypasses the rate-limiting bottleneck, pantethine expands the cellular CoA pool more efficiently than pantothenate itself. Italian, Japanese, and (later) American clinical trials in the 1980s through 2010s consistently demonstrated that 600-900 mg/day of pantethine in divided doses reduces total cholesterol and LDL by approximately 10-15%, modestly raises HDL by ~10%, and reduces triglycerides by 15-20% in patients with mild-to-moderate dyslipidemia. The effect is smaller than statins (which typically achieve 30-50% LDL reduction at standard doses) but the safety profile is exceptional — no myopathy, no hepatotoxicity signal, no glycemic disturbance. Pantethine sits in modern lipidology as an adjunct or a niche alternative for statin-intolerant patients and patients with mild lipid abnormalities, not as a first-line therapy. This page walks through the trial data, the mechanism, the practical protocols, the head-to-head comparison with statins, and where pantethine reasonably fits in contemporary cardiovascular risk management.
Table of Contents
- What Pantethine Is
- Why It Works — The CoA Pool Mechanism
- The 1980s Italian Trials
- The Japanese Approval Trials
- Rumberger 2011 — The Modern US RCT
- Pooled Effect Sizes Summary
- Pantethine vs Statins
- Practical Protocols
- Who Benefits Most
- Where Pantethine Fits in Modern Lipidology
- Patient FAQ
- Cautions
- Key Research Papers
- Connections
- Featured Videos
What Pantethine Is
Pantethine is a stable, orally absorbable form of pantotheine — specifically, two molecules of pantotheine joined by a disulfide bond between their cysteamine-derived thiol groups. The molecule is one biosynthetic step closer to Coenzyme A than pantothenic acid itself. The chemistry, schematically:
- Pantothenate (Vitamin B5) →
[PANK phosphorylates] → 4'-phosphopantothenate →
[PPCS attaches cysteine] → 4'-phosphopantothenoylcysteine →
[PPCDC decarboxylates] → 4'-phosphopantetheine →
[COASY adenylylates] → dephospho-CoA →
[COASY phosphorylates] → Coenzyme A
Pantotheine sits between the PPCDC step and the COASY step in the pathway — specifically, it is the dephosphorylated form of 4'-phosphopantetheine, formed when CoA is degraded and the phosphate is removed before the molecule is recycled back to pantothenate or to CoA again. In supplement form, two pantotheines are joined as a disulfide for chemical stability (pantotheine alone is unstable in air because the free thiol oxidizes; the disulfide is stable). The disulfide is rapidly reduced to two pantotheine molecules in the body, where they can either be phosphorylated by pantothenate kinase (PANK) directly or, in some tissues, be incorporated into the CoA biosynthesis pathway at a downstream step.
Key point: pantethine bypasses the PANK rate-limiting step. This is why pantethine produces clinical effects (most notably on lipid metabolism) that pantothenate itself does not produce at comparable doses. The same total nutritional contribution to CoA biosynthesis, but delivered past the regulatory bottleneck, has different functional consequences.
Why It Works — The CoA Pool Mechanism
The accepted mechanistic hypothesis for pantethine's lipid-modifying effect: pantethine expands the cellular pool of free CoA (and especially of mitochondrial CoA), which produces two downstream consequences on lipid metabolism:
1. HMG-CoA Reductase Regulation
HMG-CoA reductase is the rate-limiting enzyme of cholesterol biosynthesis — the same enzyme statin drugs inhibit. The enzyme is allosterically regulated by the CoA pool: free CoA inhibits, while elevated upstream substrate (HMG-CoA) activates. By expanding the free CoA pool, pantethine produces a modest reduction in HMG-CoA reductase activity, lowering hepatic cholesterol synthesis. The magnitude of the inhibition is far smaller than statin-mediated inhibition (statins are potent direct inhibitors at the catalytic site; pantethine produces gentle allosteric modulation), which is why pantethine's LDL-lowering effect is 10-15% rather than statins' 30-50%.
2. Enhanced Fatty Acid β-Oxidation
Fatty acid β-oxidation in mitochondria depends on a steady supply of free CoA at the start of each round of chain shortening. When the mitochondrial CoA pool is expanded by pantethine supplementation, the rate-limiting step of long-chain fatty acid oxidation is relieved, and the cell oxidizes fatty acids more efficiently. The clinical consequence is a reduction in triglyceride synthesis (less substrate available for storage) and an elevation in HDL (the lipoprotein that carries cholesterol from peripheral tissues back to liver, partly driven by improved fatty acid handling).
The combination of reduced cholesterol synthesis + enhanced fatty acid oxidation produces the characteristic pantethine lipid profile change: LDL down, total cholesterol down, triglycerides down significantly, HDL up modestly. This is roughly the same pattern as fibrates produce (gemfibrozil, fenofibrate) but driven by different molecular targets.
Other Proposed Effects
- Reduced lipid peroxidation. Pantethine's thiol chemistry (free or as the disulfide) provides modest antioxidant activity that may reduce oxidative modification of LDL particles, the proximate event in atherogenesis.
- Reduced platelet aggregation. Some early studies reported reduced platelet aggregation on pantethine, which would be cardiovascular-protective independent of the lipid effect.
- Reduced fatty liver. Multiple animal studies and some human studies show pantethine reduces hepatic steatosis — consistent with the enhanced fatty acid oxidation mechanism.
The 1980s Italian Trials
Pantethine's lipid-lowering effect was first established in a series of Italian clinical trials in the 1980s, primarily at the University of Bologna and various centers across northern Italy. The Italian government approved pantethine as a prescription lipid-modifying agent in 1979, which is why so much of the early literature comes from Italian-language journals.
Gaddi et al. (1984)
One of the foundational trials. Patients with type II and IIb hyperlipoproteinemia received pantethine 900 mg/day for varying durations. Results showed consistent reductions in total cholesterol (~15%), LDL cholesterol (~10-15%), and triglycerides (~15-25%), with a modest HDL increase. Effects were apparent within 2 months and stabilized by 4 months.
Bertolini et al. (1986)
Pantethine in patients with hypercholesterolemia. 600 mg/day produced comparable lipid changes to the 900 mg/day Gaddi protocol. Confirmed that 600 mg/day was an adequate clinical dose.
Arsenio et al. (1986)
Specifically addressed triglyceride reduction and HDL elevation. 900 mg/day for 6 months. Triglycerides fell by 25-30% in patients with elevated baseline triglycerides; HDL rose by approximately 10-12%. Particularly relevant for the metabolic-syndrome lipid phenotype (high TG, low HDL) that has become the dominant lipid pattern of concern in modern populations.
Da Col et al. (1985)
Open trial in hyperlipidemic diabetics — relevant given that diabetic dyslipidemia (high triglycerides, low HDL, small dense LDL particles) is the lipid pattern most associated with cardiovascular risk in the post-statin era. Pantethine reduced triglycerides and total cholesterol without affecting glycemic control adversely.
The Italian trial body, taken collectively, established 600-900 mg/day pantethine as a clinically meaningful lipid-modifying intervention. The trials were generally small (typically 20-60 patients each), open-label or single-blind, often industry-sponsored, and predated modern reporting standards — but they were consistent in direction and effect size, and they were the basis on which European regulators approved pantethine as a prescription cardiovascular agent.
The Japanese Approval Trials
Pantethine has a longer and stronger clinical history in Japan than in Western countries. The original development was actually done by Japanese pharmaceutical research in the 1950s-60s — pantethine reached the Japanese market as a prescription drug for dyslipidemia, hepatic steatosis, and related metabolic conditions decades before its Italian re-emergence.
Key Japanese trials and observations:
- Multiple multi-center trials in the 1960s-70s established pantethine's safety and efficacy for hyperlipidemia in Japanese populations
- Studies in alcoholic fatty liver showed pantethine reduced hepatic triglyceride content
- Use in diabetic dyslipidemia was particularly well-studied
- Pantethine remains an approved pharmaceutical in Japan with a long-established safety record — one of the few "natural" molecules that achieved formal Japanese drug approval rather than supplement status
The cross-cultural validation matters: the Italian and Japanese trials independently confirmed similar effect sizes (10-15% LDL reduction, 15-25% TG reduction, ~10% HDL elevation) in different populations and different research traditions. This raises the confidence that the effect is real and reproducible, even though individual trials are small by modern statin-trial standards.
Rumberger 2011 — The Modern US RCT
The most methodologically rigorous modern trial of pantethine in a Western population was Rumberger et al., published in Nutrition Research in 2011 and a follow-up in 2014.
Study design:
- 120 subjects (primarily American, mixed ethnicity) with low-to-moderate cardiovascular risk and elevated LDL
- Randomized, double-blind, placebo-controlled
- Pantethine 600 mg/day (Pantesin formulation) vs placebo
- 16-week treatment period
- Patients were on a TLC (Therapeutic Lifestyle Changes) diet throughout, similar to NCEP guidelines
Results:
- Total cholesterol reduced by approximately 6% vs placebo
- LDL cholesterol reduced by approximately 11% vs placebo
- Non-HDL cholesterol reduced by approximately 8% vs placebo
- HDL changes were modest and not significantly different from placebo
- Triglyceride changes were modest in this low-baseline-TG population (the effect is larger when baseline TG is elevated)
- Safety profile was excellent — no significant adverse events, no myopathy signal, no liver function changes
A follow-up Rumberger publication in 2014 added apolipoprotein B and lipoprotein subfraction data, showing pantethine reduced small dense LDL particle concentration — the atherogenic LDL subtype — in addition to total LDL.
Rumberger 2011 effectively confirmed the older Italian and Japanese results in a modern American population using contemporary research standards. The effect sizes were slightly smaller than the Italian trials reported (probably because of the more rigorous placebo control and the diet baseline), but the direction and approximate magnitude were consistent. This was the trial that brought pantethine into modern American integrative-cardiology practice.
Pooled Effect Sizes Summary
| Lipid Parameter | Expected Change (600-900 mg/day pantethine, 4-6 months) |
|---|---|
| Total cholesterol | −10 to −15% |
| LDL cholesterol | −10 to −15% |
| HDL cholesterol | +5 to +10% |
| Triglycerides | −15 to −25% (larger effect at higher baseline) |
| Apolipoprotein B | −8 to −12% |
| Small dense LDL particle count | Reduced (Rumberger 2014) |
| Time to maximal effect | 4-6 months |
| Effect persists with continued use | Yes (no tachyphylaxis) |
| Effect reverses on discontinuation | Yes — typically within 2-4 weeks |
Pantethine vs Statins
| Aspect | Pantethine | Atorvastatin / Rosuvastatin |
|---|---|---|
| LDL reduction | 10-15% | 30-55% |
| Triglyceride reduction | 15-25% (better at higher baseline) | 10-25% |
| HDL change | +5 to +10% | +5 to +10% |
| CV outcome data | None — no hard endpoint trials | Extensive — mortality, MI, stroke reductions in large RCTs |
| Myopathy risk | None documented | ~5% mild, ~0.1% severe (rhabdomyolysis very rare) |
| Hepatotoxicity | None documented | Rare LFT elevations |
| Glycemic effect | Neutral or modestly favorable | Small increase in diabetes incidence (well-documented but small effect) |
| CoQ10 depletion | No — pantethine actually supports mitochondrial function | Yes — statins reduce endogenous CoQ10 (clinical significance debated) |
| Cost (US, monthly) | $25-50 | $5-15 (generic) |
| Insurance coverage (US) | Not covered — OTC supplement | Generally covered |
The clinical bottom line: pantethine's LDL-lowering effect is about one-third the magnitude of moderate-intensity statin therapy. For patients at high cardiovascular risk who need substantial LDL reduction (post-MI, diabetic with established CHD, familial hypercholesterolemia), pantethine is not adequate as monotherapy — the statins' established mortality benefit in those populations is too important to forgo. For patients at low-to-moderate risk who want modest LDL reduction without statins, who are statin-intolerant, or who are in primary prevention with a borderline risk profile, pantethine is a reasonable option.
The biggest functional difference between pantethine and statins is not the effect size on LDL — it's the absence of hard cardiovascular outcome trials for pantethine. Statins have repeatedly demonstrated reductions in MI, stroke, and mortality across multiple populations. Pantethine has only shown lipid-level changes; no trial has been powered to detect a cardiovascular event reduction. Whether the lipid changes pantethine produces translate proportionally into clinical outcomes is a reasonable hypothesis but not proven.
Practical Protocols
Standard protocol (mild-moderate dyslipidemia)
- Pantethine 300 mg three times daily (900 mg/day total) — the Italian-trial dose
- OR Pantethine 300 mg twice daily (600 mg/day total) — the Rumberger US trial dose
- Take with meals to optimize absorption
- Concurrent TLC diet (reduced saturated fat, increased fiber, weight management)
- Re-check lipid panel at 12 weeks; full effect by 4-6 months
Triglyceride-focused protocol
- Pantethine 600-900 mg/day in divided doses
- Add omega-3 (EPA+DHA) 2-3 g/day — the strongest natural triglyceride-lowering combination
- Berberine 500 mg twice daily can further reduce TG and LDL with complementary mechanism
- Aggressive carbohydrate reduction (carbohydrate restriction is the most effective intervention for elevated TG)
Statin-intolerant patient protocol
- Pantethine 600 mg/day
- Plant sterols (1.5-2 g/day) — additive LDL-lowering through reduced cholesterol absorption
- Red yeast rice (1.2-2.4 g/day standardized to monacolin K) — a natural source of monacolin K (chemically identical to lovastatin); use cautiously and only in mild cases, since it carries some of the same myopathy risk as pharmaceutical statins
- Berberine 500 mg twice daily
- Bergamot extract (500-1000 mg/day standardized to flavonoids) — another complementary lipid-lowering compound
Combination with statin (lower statin dose)
- Some patients on a statin can reduce the statin dose by adding pantethine 600 mg/day, achieving similar lipid control with less statin exposure and lower myopathy risk
- This is an off-label combination but is used in practice. Discuss with prescribing physician.
Forms and brands: Pantesin is the most-studied pantethine ingredient (used in Rumberger 2011). Multiple supplement brands sell pantethine in 300 mg or 450 mg capsules. The product should specify pantethine (not pantothenic acid) and ideally indicate the Pantesin or similar pharmacopeial-grade source.
Who Benefits Most
Pantethine produces the most clinically meaningful benefit in:
- Mild-to-moderate hypercholesterolemia (LDL 130-190 mg/dL) where a 10-15% reduction is enough to bring LDL to target without statin therapy
- Mixed dyslipidemia with high triglycerides — the TG-lowering effect is largest when baseline TG is >150 mg/dL. Patients with TG 200-500 mg/dL often see meaningful reductions.
- Metabolic syndrome lipid phenotype (high TG, low HDL, small dense LDL) — pantethine addresses all three abnormalities
- Diabetic dyslipidemia — pantethine improves lipids without adversely affecting glucose control, and may modestly improve fatty liver
- Statin-intolerant patients who have stopped a statin because of muscle symptoms or other side effects but still need lipid management
- Patients in primary prevention with borderline risk who want to avoid pharmaceutical therapy if possible
- Patients with non-alcoholic fatty liver disease (NAFLD) — the mitochondrial fatty acid oxidation effect addresses the underlying pathology
Pantethine is not adequate for:
- Patients with established cardiovascular disease (post-MI, post-stroke, established CHD) who need maximal LDL reduction
- Familial hypercholesterolemia (heterozygous or homozygous), which requires substantial LDL reduction beyond what pantethine achieves
- Patients with very high baseline LDL (>190 mg/dL) without other intervention
- Acute lipid management post-cardiac event — the clinical benefit of statins in this setting is too well-established and too large to forgo for a smaller alternative
Where Pantethine Fits in Modern Lipidology
Pantethine occupies a specific and reasonable niche in contemporary cardiovascular risk management:
- Adjunct to lifestyle in primary prevention. The first-line intervention for elevated lipids in primary prevention remains diet, exercise, weight management, and addressing metabolic factors. Pantethine sits as a low-risk pharmacologic adjunct for patients who have done the lifestyle work but still have lipid abnormalities that would benefit from further reduction.
- Alternative for statin-intolerant patients. The roughly 5-10% of patients who cannot tolerate any statin (true statin myopathy, severe statin-associated muscle symptoms) need alternative lipid management. Ezetimibe, PCSK9 inhibitors, and bempedoic acid are pharmacologic options; pantethine is a reasonable adjunct or alternative in mild cases.
- Combination therapy. Some patients are well-controlled on a low-dose statin + pantethine combination who would otherwise need higher statin doses. This reduces statin exposure and may reduce side effects.
- Triglyceride-dominant phenotype. The TG-lowering effect is one of pantethine's strongest, particularly relevant in metabolic-syndrome populations where the lipid abnormality is dominated by TG and small dense LDL rather than absolute LDL elevation.
- NAFLD adjunct. The mitochondrial fatty acid oxidation effect that drives the lipid changes also addresses hepatic steatosis. Pantethine has a long Japanese clinical history specifically for fatty liver disease.
What pantethine is not: a replacement for statins in established cardiovascular disease, a "natural alternative" that has equivalent outcomes data to statins, or a sufficient intervention for severe dyslipidemia. Honest positioning is important — both for patient safety (don't forgo statins when they're indicated) and for the integrative-medicine community's long-term credibility.
Patient FAQ
Q: Can pantethine replace my statin?
Depends entirely on your cardiovascular risk profile. If you have established coronary artery disease, post-MI, or stroke history, your statin is doing more than just lowering LDL — it's reducing your risk of another event with strong outcome trial evidence. Don't stop your statin to substitute pantethine in those settings. If you are in primary prevention with mild lipid elevation and no established disease, an attempt at pantethine + lifestyle is reasonable, with re-evaluation in 4-6 months.
Q: How long until I see results?
Lipid panel improvement typically appears at 8-12 weeks; full effect by 4-6 months. Re-check labs at 12 weeks; if no movement at all by then, the response is likely to be limited and you may want to add other interventions or reconsider.
Q: Will I get the statin "muscle aches" from pantethine?
No. Pantethine has no documented myopathy or muscle-symptom signal across all the trials. The mechanism is completely different from statins.
Q: Is the 600 mg or 900 mg dose better?
The trials suggest 600 mg/day is the minimum clinically effective dose; 900 mg/day produces modestly larger effects but the dose-response curve flattens. 600 mg/day is the standard, divided into 300 mg twice daily or 200 mg three times daily.
Q: Should I take it with my statin?
You can; there are no significant interactions. The combination is sometimes used to achieve target lipid levels with a lower statin dose. Discuss with your prescriber.
Q: What about red yeast rice or other natural alternatives?
Red yeast rice contains monacolin K, which is chemically identical to lovastatin — effectively a "natural statin." It has the same potential for myopathy, hepatotoxicity, and drug interactions as pharmaceutical statins, just at typically lower doses. Don't combine red yeast rice with a prescription statin (double dose). Pantethine is mechanistically different and combines safely with all the statin-pathway interventions.
Q: Will it affect my blood sugar?
No adverse effect; possibly mildly favorable in diabetic populations. Pantethine does not have the small diabetes-incidence increase seen with statins.
Cautions
- Don't substitute for statins in established cardiovascular disease. If you have had an MI, stroke, or have established CAD, your statin is preventing another event with strong evidence. Pantethine does not have outcome trial data and should not replace statin therapy in this setting.
- GI side effects. Mild loose stools or stomach upset can occur, particularly when starting. Take with food; split the dose across the day.
- Mild thiol odor. Some patients notice a faint sulfurous odor in breath or urine on pantethine — this is the disulfide chemistry and is harmless.
- Pregnancy and lactation. Limited safety data at pharmacologic doses. Avoid pantethine supplementation in pregnancy unless directed by a physician with experience in this area.
- Drug interactions. No significant interactions documented. Safe to combine with statins, ezetimibe, fibrates, PCSK9 inhibitors, bempedoic acid, niacin, omega-3, plant sterols.
- Monitor your actual lipids. Don't assume the effect is happening — check your labs at 12 weeks. About 70% of patients respond; 30% have minimal response despite consistent use.
- Address the underlying lifestyle. Pantethine works best as part of a comprehensive lifestyle approach (diet, exercise, weight management, sleep). It is not a license to ignore the upstream metabolic drivers.
- Biotin competition. Like pantothenate, pantethine shares the SMVT transporter with biotin. Long-term high-dose use may modestly reduce biotin absorption; add 300-500 µg biotin daily if on the protocol >6 months.
Key Research Papers
- Gaddi A, Descovich GC, Noseda G et al. (1984). Controlled evaluation of pantethine, a natural hypolipidemic compound, in patients with different forms of hyperlipoproteinemia. Atherosclerosis. — PubMed
- Bertolini S, Donati C, Elicio N et al. (1986). Lipoprotein changes induced by pantethine in hyperlipoproteinemic patients: adults and children. International Journal of Clinical Pharmacology, Therapy, and Toxicology. — PubMed
- Arsenio L, Bodria P, Magnati G, Strata A, Trovato R (1986). Effectiveness of long-term treatment with pantethine in patients with dyslipidemia. Clinical Therapeutics. — PubMed
- Da Col PG et al. (1985). Pantethine in the treatment of hypercholesterolemia: a randomized double-blind trial vs tiadenol. Current Therapeutic Research. — PubMed
- Rumberger JA, Napolitano J, Azumano I, Kamiya T, Evans M (2011). Pantethine, a derivative of vitamin B(5) used as a nutritional supplement, favorably alters low-density lipoprotein cholesterol metabolism in low- to moderate-cardiovascular risk North American subjects: a triple-blinded placebo and diet-controlled investigation. Nutrition Research. — PubMed
- Evans M, Rumberger JA, Azumano I, Napolitano JJ, Citrolo D, Kamiya T (2014). Pantethine, a derivative of vitamin B5, favorably alters total, LDL and non-HDL cholesterol in low to moderate cardiovascular risk subjects eligible for statin therapy: a triple-blinded placebo and diet-controlled investigation. Vascular Health and Risk Management. — PubMed
- Coronel F, Tornero F, Torrente J et al. (1991). Treatment of hyperlipemia in diabetic patients on dialysis with a physiological substance. American Journal of Nephrology. — PubMed
- Cattin L et al. (1985). The treatment of hypercholesterolemia: a comparative study between pantethine and bezafibrate. Current Therapeutic Research. — PubMed
- Carrara P, Matturri L, Galbussera M, Lovati MR, Franceschini G, Sirtori CR (1984). Pantethine reduces plasma cholesterol and the severity of arterial lesions in experimental hypercholesterolemic rabbits. Atherosclerosis. — PubMed
- Wittwer CT et al. (1989). Hepatic uptake of pantothenate and pantethine in rats. Journal of Nutrition. — PubMed
- Tonutti L et al. (1991). Pantethine in subjects with type IIa hyperlipidaemia. European Journal of Clinical Research. — PubMed
- Pins JJ, Keenan JM (2006). Dietary and nutraceutical options for managing the hypertriglyceridemic patient. Progress in Cardiovascular Nursing. — PubMed
PubMed Topic Searches
- PubMed: pantethine cholesterol
- PubMed: pantethine LDL HDL TG
- PubMed: pantethine NAFLD
- PubMed: pantethine statin intolerance
- PubMed: pantethine HMG-CoA reductase
- PubMed: pantesin cardiovascular
Connections
- Vitamin B5 Overview
- B5 Benefits Hub
- CoA Biosynthesis
- Adrenal Support
- Acne & Skin
- Cholesterol
- Cardiology
- Metabolic Syndrome
- Diabetes
- NAFLD (Fatty Liver)
- Lipid Panel
- Apolipoprotein B
- LDL Particle Number
- Berberine
- CoQ10