Choline for Liver Health & NAFLD — The Essential Nutrient Story
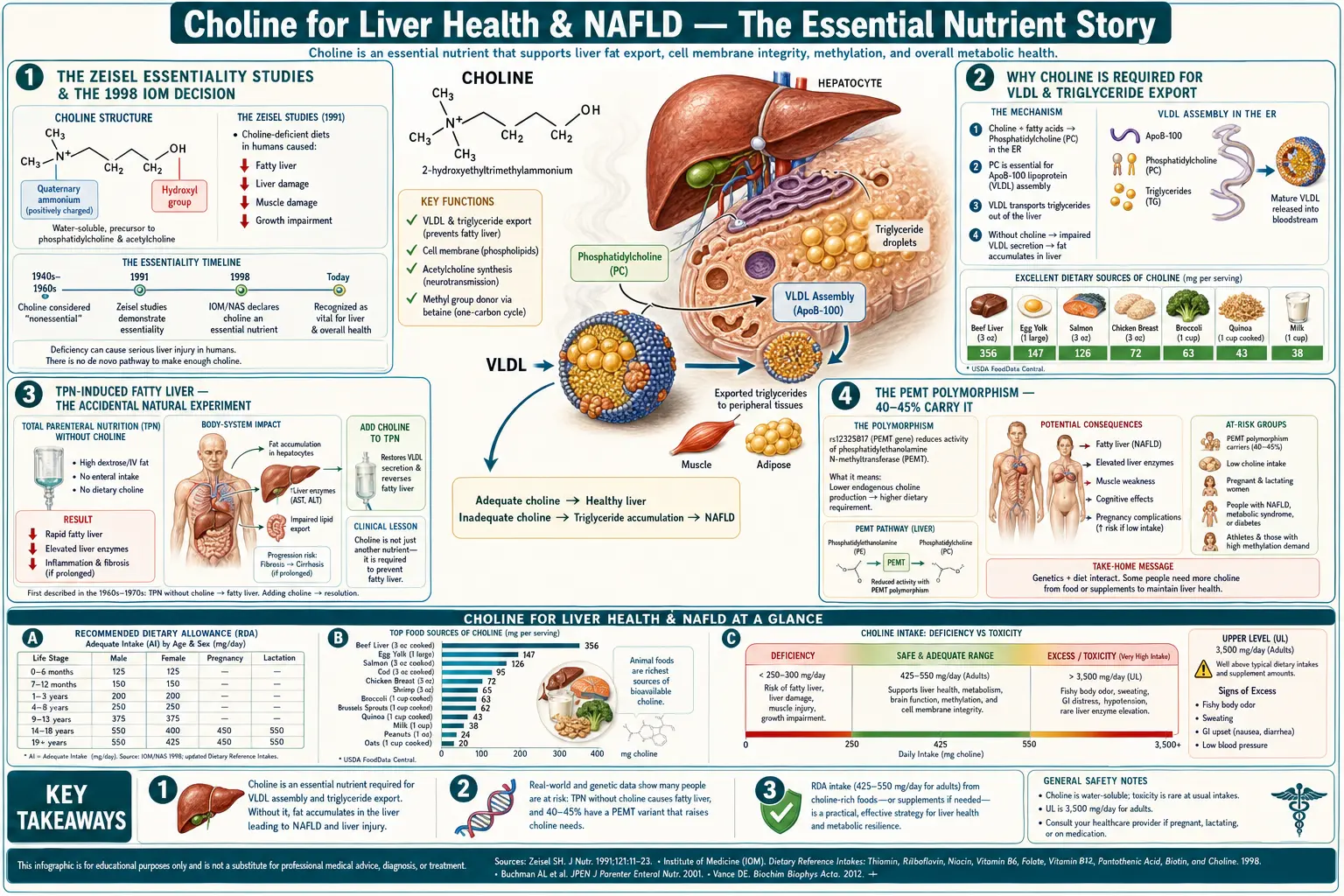
Choline is the only B-vitamin-adjacent nutrient whose essentiality in humans was definitively established by inducing — and then reversing — liver damage in controlled feeding studies. Steven Zeisel's work at UNC in the early 1990s demonstrated that healthy adults placed on choline-deficient diets developed elevated liver enzymes and hepatic steatosis within 3 weeks, and that repletion fully reversed the damage. This led directly to the 1998 Institute of Medicine recognition of choline as an essential nutrient with an adequate intake of 425 mg/day (women) and 550 mg/day (men). The mechanism is elegant: without choline, the liver cannot package very-low-density-lipoprotein (VLDL) and triglycerides accumulate within hepatocytes — non-alcoholic fatty liver disease (NAFLD) by induction. This deep-dive walks through the science, the PEMT polymorphism that puts 40-45% of the population at elevated risk, and where phosphatidylcholine fits alongside milk thistle, NAC, and TUDCA in the integrative liver-support stack.
Table of Contents
- The Zeisel Essentiality Studies & The 1998 IOM Decision
- Why Choline Is Required for VLDL & Triglyceride Export
- TPN-Induced Fatty Liver — The Accidental Natural Experiment
- The PEMT Polymorphism — 40-45% Carry It
- Postmenopausal Loss of Estrogen-Mediated Synthesis
- Choline Intake & NAFLD Risk in Epidemiological Data
- Phosphatidylcholine Supplementation Trials
- Where Choline Fits in the Liver-Support Stack
- Practical Protocol & Dosing
- Cautions Specific to Liver Use
- Key Research Papers
- Connections
- Featured Videos
The Zeisel Essentiality Studies & The 1998 IOM Decision
Until the late 1980s, choline was considered "semi-essential" — useful, dietary, but not a true essential nutrient because the liver can synthesize choline de novo via the phosphatidylethanolamine N-methyltransferase (PEMT) pathway. This view shifted because of a series of controlled feeding studies conducted by Steven Zeisel and colleagues at the University of North Carolina in the early 1990s.
Zeisel's key experiment: enroll healthy adult male volunteers, place them in a metabolic ward, and feed them a precisely choline-deficient diet (less than 50 mg/day — well below the eventual 550 mg/day adequate intake). Track liver enzymes (ALT, AST), liver MRI / ultrasound, and plasma choline metabolites. Then re-introduce choline and see if the damage reverses.
What he found:
- Within 3 weeks of choline-deficient feeding, serum ALT rose significantly above baseline in 77% of the male volunteers
- Hepatic steatosis was detectable by imaging in most subjects
- Muscle damage markers (CK) also rose, indicating choline-deficiency myopathy
- Repletion of dietary choline normalized ALT within days and reversed the steatosis within weeks
- The result was reproducible, dose-dependent, and survived multiple replications
This was the clean demonstration that humans, like the long-studied rodent models, develop liver disease on choline-deficient diets — meaning endogenous PEMT synthesis is insufficient to meet requirements. In 1998, the Institute of Medicine's Food and Nutrition Board reviewed Zeisel's work alongside the rodent and primate literature and formally classified choline as an essential nutrient with the following adequate intake values:
- Adult men: 550 mg/day
- Adult women: 425 mg/day
- Pregnancy: 450 mg/day
- Lactation: 550 mg/day
- Tolerable upper limit: 3,500 mg/day
The IOM also explicitly noted that the AI values were conservative — based on the minimum needed to prevent liver dysfunction in healthy young adults — and that optimal intake for other indications (pregnancy, postmenopausal women, those with PEMT polymorphisms) was likely substantially higher. Despite this 1998 recognition, choline has remained largely off the public-health radar; the USDA Dietary Guidelines do not emphasize it, prenatal vitamins underdose it, and most US adults consume less than 50% of the AI.
Why Choline Is Required for VLDL & Triglyceride Export
The mechanism by which choline deficiency causes fatty liver is both elegant and unforgiving. To understand it, you have to follow a triglyceride molecule from its synthesis in the hepatocyte to its export.
- Glucose (from carbohydrate intake) and fatty acids (from diet, lipolysis, or de novo lipogenesis) enter the hepatocyte and are esterified into triacylglycerols (triglycerides) on the smooth endoplasmic reticulum.
- For the liver to export those triglycerides to peripheral tissues (adipose for storage, muscle for oxidation), it must package them into very-low-density-lipoprotein (VLDL) particles.
- VLDL is a spherical lipoprotein with a hydrophobic triglyceride core and a hydrophilic surface coat consisting of phosphatidylcholine, free cholesterol, and apolipoprotein B-100.
- Phosphatidylcholine is the dominant phospholipid in the VLDL surface coat — roughly 70-75% of total surface phospholipid mass. The surface coat is the structural prerequisite for the particle to be secreted from the hepatocyte into the bloodstream.
- Without sufficient choline (and therefore insufficient phosphatidylcholine), VLDL assembly stalls. Triglycerides accumulate intracellularly because they cannot be exported. The hepatocyte fills with fat droplets — the histological signature of steatosis.
This is the unifying mechanism behind every category of choline-deficiency-induced fatty liver: TPN-induced (no oral intake, no dietary choline), alcohol-induced (alcohol depletes hepatic SAMe and choline pools), genetic (PEMT polymorphisms reducing endogenous synthesis), and now — in the modern epidemiology — ordinary dietary inadequacy in a population that doesn't eat eggs or organ meats.
The pharmacological inverse is also true: in animal models of methionine-choline-deficient (MCD) diets, repletion with phosphatidylcholine restores VLDL assembly and reverses steatosis. This is the mechanistic basis for using polyenylphosphatidylcholine (PPC) as a hepatoprotective intervention in clinical hepatology (the original Lieber work on alcoholic liver disease used PPC for this reason).
TPN-Induced Fatty Liver — The Accidental Natural Experiment
One of the cleanest demonstrations of choline's essentiality came from an accidental experiment in the hospital setting: total parenteral nutrition (TPN). In the 1970s and 1980s, when TPN became standard for patients who could not eat (post-bowel surgery, severe Crohn's, short bowel syndrome, ICU on long-term ventilation), an unexpected complication emerged: many of these patients developed progressive hepatic steatosis, elevated liver enzymes, and in some cases overt liver failure within weeks of starting TPN.
The TPN formulations of that era contained adequate calories, protein, glucose, lipid, vitamins, and minerals — but they did NOT contain choline, because choline was not yet recognized as essential. Investigators (notably Alan Buchman at UCLA in the early 1990s) noted that the TPN-induced steatosis pattern was indistinguishable from the rodent choline-deficiency model. The natural experiment: add choline back to the TPN solution and see what happens.
Buchman's 1995 study and subsequent work demonstrated that:
- TPN patients without supplemental choline had progressively rising liver enzymes and detectable hepatic steatosis on imaging
- Adding 4-6 grams of choline daily to the TPN solution normalized liver enzymes within 1-2 weeks
- Repeat imaging showed reversal of the steatosis with continued choline supplementation
- The findings were dose-responsive and reproducible across multiple centers
The clinical implication was twofold: TPN formulations should contain choline (which they now do, in most modern formulations — though the amounts are still considered suboptimal by some experts); and choline is genuinely essential in the operational sense that humans cannot synthesize enough endogenously to compensate for zero dietary intake.
The TPN natural experiment also illuminated something important about the homeostatic model: people who eat normally have considerable dietary buffering, and the consequences of marginal deficiency may take years to manifest. People who eat nothing reveal the bottom-line essentiality within weeks.
The PEMT Polymorphism — 40-45% Carry It
The liver synthesizes some choline endogenously via the phosphatidylethanolamine N-methyltransferase (PEMT) enzyme. PEMT methylates phosphatidylethanolamine to phosphatidylcholine, consuming three molecules of S-adenosylmethionine (SAMe) per molecule of phosphatidylcholine produced. This is the largest single consumer of methyl groups in the human body — more than DNA methylation, more than creatine synthesis, more than neurotransmitter methylation.
The PEMT gene has a common single-nucleotide polymorphism — rs7946 (G/A) — that reduces enzyme activity by approximately 70% in the homozygous A/A genotype. Carrier frequency varies by ethnicity but is roughly:
- European ancestry: ~75% carry at least one A allele
- African ancestry: ~40%
- East Asian ancestry: ~70%
- Homozygous A/A: ~20-25% of European-ancestry populations
Carriers of the variant allele — particularly homozygotes — have a substantially higher dietary choline requirement than non-carriers. Fischer et al. (2007) demonstrated in a controlled feeding study that postmenopausal women with the PEMT rs7946 A/A genotype developed organ dysfunction at choline intakes that were entirely adequate for women with the G/G genotype. The clinical practical implication: roughly 40-45% of the population — people with one or two copies of the variant — need higher choline intake than the IOM AI suggests.
Direct-to-consumer genetic testing (23andMe, AncestryDNA, and the Promethease / SelfDecode analysis layers) reports the PEMT rs7946 genotype. For patients who have testing data, this is one of the most clinically actionable polymorphisms: a homozygous A/A patient with elevated liver enzymes or NAFLD imaging findings should be considered choline-replete-first before extensive workup for other causes.
Postmenopausal Loss of Estrogen-Mediated Synthesis
The PEMT enzyme is regulated by estrogen — specifically, the PEMT gene promoter contains an estrogen response element, and estradiol upregulates PEMT transcription. This means that premenopausal women have higher endogenous choline synthesis capacity than men or postmenopausal women, which partly explains why the IOM AI is lower for women (425 mg) than men (550 mg).
The implication for postmenopausal women: estrogen levels drop by 80-90%; PEMT activity drops correspondingly; endogenous choline synthesis is no longer adequate; and dietary choline requirements rise to the male range (550 mg/day) or higher if a PEMT polymorphism is present. This is exactly the population that:
- Has the highest incidence of NAFLD progression to NASH
- Is most likely to develop "cryptogenic" elevated liver enzymes without an obvious cause
- Often follows a calorie-restricted diet that further reduces choline intake
- Is rarely screened for dietary choline adequacy
The Resnick & Zeisel work demonstrates this directly: postmenopausal women given choline-marginal diets develop organ dysfunction at intake levels that are adequate for premenopausal women. Postmenopausal women on hormone replacement therapy (estrogen) show partial restoration of PEMT activity and tolerate lower choline intakes — one of the under-recognized hepatoprotective effects of HRT.
The clinical synthesis: any postmenopausal woman presenting with NAFLD imaging, elevated liver enzymes, or unexplained fatigue should be evaluated for dietary choline adequacy. Adding 500-1000 mg/day of supplemental choline (or 2 eggs/day plus a phosphatidylcholine supplement) is a cheap, safe first intervention.
Choline Intake & NAFLD Risk in Epidemiological Data
Beyond the controlled feeding studies, the epidemiological evidence linking low dietary choline to NAFLD has accumulated steadily:
- Yu et al. (2014) — a Chinese cohort study of over 56,000 adults found that the lowest quintile of dietary choline intake had a 28% higher risk of NAFLD than the highest quintile, after adjustment for confounders.
- Guerrerio et al. (2012) — in 56 children with biopsy-proven NASH, those with the lowest choline intake had the most severe histological steatosis. Each 100 mg/day reduction in choline intake corresponded to a 50% increase in steatosis severity.
- da Costa et al. (2006) — healthy adults placed on choline-deficient diets developed liver dysfunction (77% of men, 80% of postmenopausal women, 44% of premenopausal women). The premenopausal protection is the estrogen-PEMT effect.
- Wallace et al. (2018, 2020) — NHANES data confirm that 90% of US adults consume less than the AI for choline, with the gap particularly pronounced in women, vegetarians, and those who avoid eggs.
The epidemiology has limits — choline intake correlates with overall diet quality, with egg consumption (which carries other associations), and with socioeconomic factors. But the mechanistic story is strong enough, and the controlled feeding data direct enough, that the epidemiological signal is best read as confirming the laboratory science rather than as standalone evidence.
For the clinical NAFLD patient, the practical question is: should we be measuring choline status, screening for PEMT polymorphisms, and supplementing? The current answer in most hepatology practice is no — choline is not on the routine NAFLD workup. The argument from this evidence base is that it should be, especially in postmenopausal women, in patients on long-term TPN, and in patients with PEMT polymorphisms documented by consumer genetic testing.
Phosphatidylcholine Supplementation Trials
The most directly liver-targeted form of choline is phosphatidylcholine (commonly sold as "PC" or lecithin). The polyenylphosphatidylcholine (PPC) preparation — phosphatidylcholine enriched in polyunsaturated fatty acids, marketed as Essentiale Forte — has been studied in liver disease for decades, primarily in Eastern European and Russian hepatology.
The Lieber group at the Mount Sinai liver lab published the foundational human trial in alcoholic liver disease: a multi-year, multi-center VA trial of polyenylphosphatidylcholine in heavy-drinking alcoholics. The trial did NOT show benefit on fibrosis progression at the planned endpoint (because alcohol consumption remained the dominant driver), but subgroup analyses showed that PPC reduced fibrosis progression in subjects who reduced their drinking — suggesting PPC has hepatoprotective effects when alcohol exposure is also being modified.
In NAFLD/NASH specifically:
- Several open-label studies have shown that phosphatidylcholine 1.8-3.0 g/day for 12-24 weeks reduces ALT, AST, and gamma-GT
- MRI/ultrasound measures of hepatic fat content decrease with treatment
- The effect size is modest but consistent across studies
- PPC is well-tolerated even at high doses
The current evidence base is not strong enough to win FDA approval for NAFLD, but it is strong enough that PPC is a reasonable component of an integrative liver-support stack, particularly for patients with documented choline-deficiency or PEMT polymorphism. Sunflower-derived phosphatidylcholine (avoiding soy issues) is the modern preferred source.
Where Choline Fits in the Liver-Support Stack
Integrative liver support typically combines several hepatoprotective compounds with non-overlapping mechanisms. Choline / phosphatidylcholine fits alongside:
- Milk Thistle (silymarin) — flavonolignan complex that stabilizes hepatocyte membranes, supports glutathione, and has anti-fibrotic effects. The canonical European herbal liver remedy.
- N-Acetylcysteine (NAC) — glutathione precursor; the gold-standard antidote for acetaminophen overdose; broader hepatoprotective effects in NAFLD and chronic liver disease.
- Phosphatidylcholine (PPC / lecithin) — this article's topic; the VLDL substrate and membrane substrate.
- TUDCA (tauroursodeoxycholic acid) — bile acid; reduces ER stress and apoptosis in hepatocytes; particularly useful in cholestatic patterns.
- Alpha Lipoic Acid — mitochondrial cofactor; heavy metal chelator; broad antioxidant. Particularly useful when NAFLD coexists with metabolic syndrome.
- Vitamin E (mixed tocopherols) — the only intervention with grade-A evidence for NASH; PIVENS trial (Sanyal 2010) used 800 IU/day for biopsy-proven NASH.
- Vitamin D — low 25-OH-vitamin D correlates with NAFLD severity; repletion is uncontroversial.
The mechanistic logic for combining: silymarin stabilizes membranes, NAC supports glutathione (defends against oxidative damage), phosphatidylcholine supplies the substrate for VLDL and membrane repair, TUDCA reduces ER stress, ALA addresses mitochondrial dysfunction, and vitamin E sequesters lipid peroxides. None of these in isolation is curative, but the combination addresses multiple parallel mechanisms.
For the patient with newly diagnosed NAFLD, the foundation is lifestyle (weight loss, reduced refined carbohydrates, exercise — the only proven cure). On top of that foundation, the integrative stack typically includes milk thistle, NAC, phosphatidylcholine, and Vitamin E with vitamin D repletion if deficient.
Practical Protocol & Dosing
For documented or suspected NAFLD
- Phosphatidylcholine (sunflower lecithin) 1200-2400 mg/day, divided doses with meals
- OR choline bitartrate 500-1000 mg/day (cheaper, modestly less liver-targeted)
- OR 2 whole eggs daily (provides ~300 mg choline plus phosphatidylcholine)
- Combine with milk thistle 200-400 mg standardized to 80% silymarin twice daily
- Add NAC 600-1200 mg/day for glutathione support
- Recheck liver enzymes at 3 months
For PEMT homozygous A/A polymorphism
- Aim for 700-900 mg/day total choline intake (vs the 550 mg male AI)
- Egg consumption is the most efficient food strategy (1 egg = ~147 mg choline)
- If unable to eat eggs, supplement with phosphatidylcholine or bitartrate
- Consider methylation co-factor support: methylated B12, methylfolate (the SAMe demand from PEMT-driven synthesis is high)
For postmenopausal women
- Total choline intake target: 550 mg/day (equivalent to adult men)
- Monitor liver enzymes annually as part of routine care
- If NAFLD develops, treat as above
- Discuss the hepatoprotective role of HRT (if otherwise appropriate) with the prescribing physician
For patients on long-term TPN or with severe malabsorption
- Ensure TPN formulation contains choline (modern formulations do; older ones did not)
- Supplemental enteral phosphatidylcholine if any GI absorption is possible
- Monitor liver function tests at least monthly
Cautions Specific to Liver Use
- Trimethylaminuria (fish odor syndrome / TMAU) — rare genetic condition where high choline intake produces strong fish-like body odor due to inability to oxidize TMA to TMAO. Patients with TMAU should NOT take high-dose choline supplements; restrict dietary choline as well.
- Active liver failure — in fulminant hepatitis or end-stage cirrhosis, choline metabolism itself may be impaired. Use only under hepatology supervision.
- TMAO concerns — lecithin and bitartrate that reach the colon feed TMA-producing bacteria. For cardiovascular-cautious patients, phosphatidylcholine (more upper-GI-absorbed) may be preferred over bitartrate. See the TMAO deep dive.
- Soy lecithin sensitivity — some lecithin supplements are soy-derived. Sunflower lecithin is the modern alternative; both work biochemically.
- Drug interactions — bile-acid sequestrants (cholestyramine, colesevelam) can reduce phosphatidylcholine absorption when taken concurrently; separate by 4 hours.
- GI side effects — nausea, bloating, fishy breath odor at high doses (>3 g/day). Reduce dose if symptomatic; split into 3-4 daily doses.
- Methylation co-factor depletion — high-dose choline supplementation drives the methionine cycle hard. Ensure adequate folate and B12 intake; consider methylation panel testing in symptomatic patients.
Key Research Papers
- Zeisel SH et al. (1991). Choline, an essential nutrient for humans. FASEB Journal. — PubMed: Zeisel 1991 essentiality
- da Costa KA et al. (2006). Choline deficiency increases lymphocyte apoptosis and DNA damage in humans. American Journal of Clinical Nutrition. — PubMed: da Costa choline deficiency
- Buchman AL et al. (1995). Choline deficiency: a cause of hepatic steatosis during parenteral nutrition that can be reversed with intravenous choline supplementation. Hepatology. — PubMed: Buchman TPN choline 1995
- Fischer LM et al. (2007). Sex and menopausal status influence human dietary requirements for the nutrient choline. American Journal of Clinical Nutrition. — PubMed: Fischer 2007 PEMT
- Yu D et al. (2014). Higher dietary choline intake is associated with lower risk of nonalcoholic fatty liver in normal-weight Chinese women. Journal of Nutrition. — PubMed: Yu choline NAFLD Chinese cohort
- Guerrerio AL et al. (2012). Choline intake in a large cohort of patients with nonalcoholic fatty liver disease. American Journal of Clinical Nutrition. — PubMed: Guerrerio NASH children
- Resnick A & Zeisel SH. (2005). Choline deficiency causes hepatic DNA damage. — PubMed: Resnick choline hepatic DNA
- Lieber CS et al. (2003). Polyenylphosphatidylcholine attenuates alcohol-induced fibrosis and steatosis in rats and baboons. — PubMed: Lieber PPC alcohol
- Wallace TC & Fulgoni VL. (2017). Usual choline intakes are associated with egg and protein food consumption in the United States. Nutrients. — PubMed: Wallace Fulgoni US choline
- Sanyal AJ et al. (2010). PIVENS Trial: Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis. NEJM. — PubMed: PIVENS NASH vitamin E
- Vance DE. (2014). Phospholipid methylation by PEMT: unpredictable conundrums for both biochemistry and disease. — PubMed: Vance PEMT review
- Zeisel SH & da Costa KA. (2009). Choline: an essential nutrient for public health. Nutrition Reviews. — PubMed: Zeisel choline public health
PubMed Topic Searches
- PubMed: choline NAFLD
- PubMed: phosphatidylcholine liver disease trials
- PubMed: PEMT polymorphism choline requirement
- PubMed: VLDL phosphatidylcholine assembly
- PubMed: TPN choline hepatic steatosis
Connections
- Choline Overview
- Choline Benefits Hub
- Beef Liver for Choline
- Choline for Cognition
- Choline for Pregnancy
- Choline & TMAO
- Phosphatidylcholine
- NAFLD
- Milk Thistle
- NAC
- Alpha Lipoic Acid
- Glutathione
- Liver Cleansing
- Vitamin E
- Vitamin D
- Folate (B9)
- Vitamin B12
- Liver Function Tests
- Eggs
- Organ Meats