Choline for Cognition — Acetylcholine, Alpha-GPC & CDP-Choline
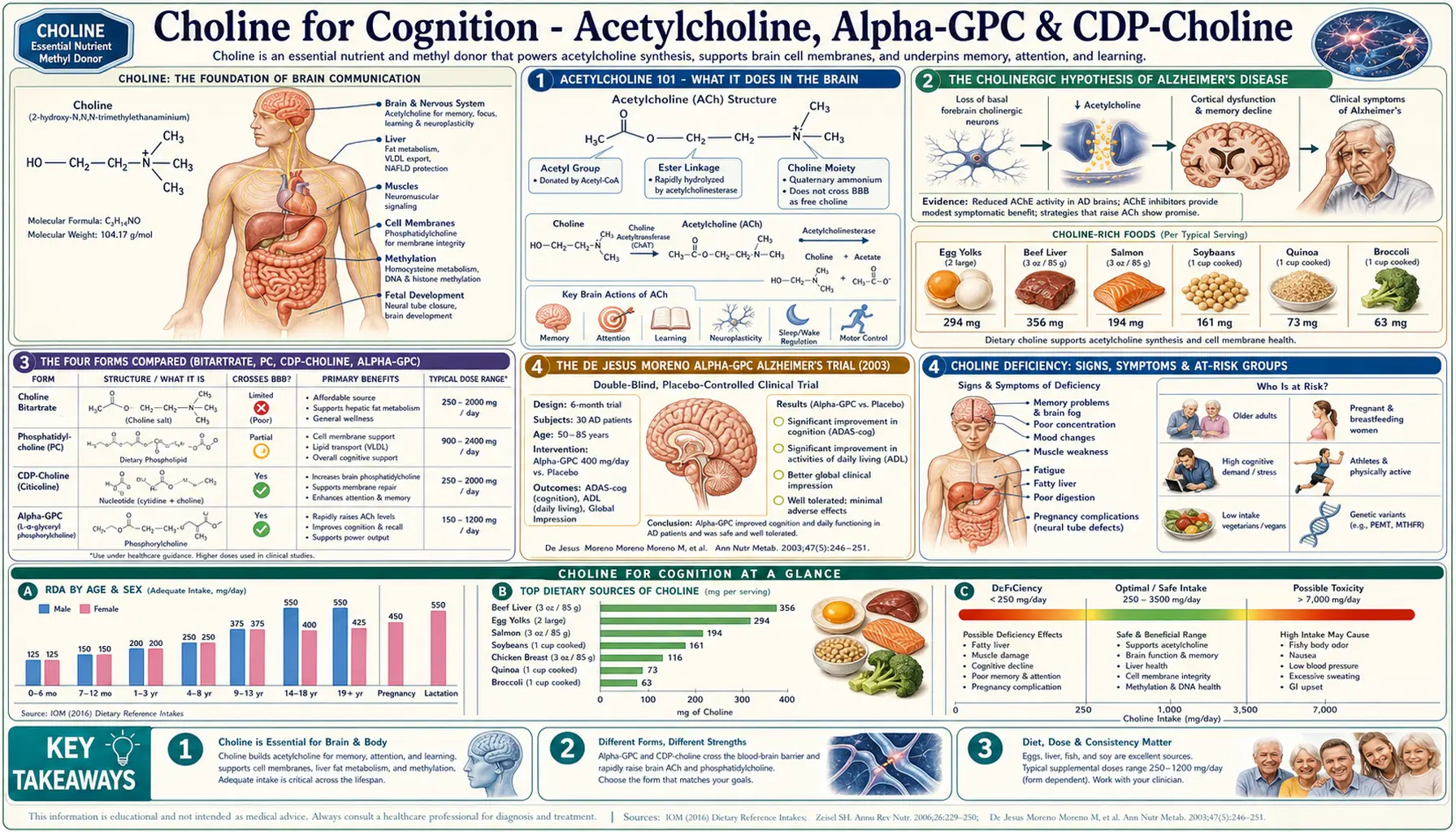
Choline is the rate-limiting precursor to acetylcholine, the neurotransmitter that governs attention, working memory, learning, REM sleep, and the parasympathetic nervous system. The two bioactive supplemental forms — Alpha-GPC (alpha-glyceryl phosphorylcholine) and CDP-choline (citicoline) — cross the blood-brain barrier far more efficiently than choline bitartrate and have generated clinical trial data for mild-to-moderate Alzheimer's disease (De Jesus Moreno 2003 multicenter RCT), vascular cognitive impairment (IDEALE 2013), elderly memory (Spiers 1996), and stroke recovery. This deep-dive walks through the trials, the four supplemental forms, the nootropic-stack rationale, and the pharmacokinetic case for choosing Alpha-GPC versus CDP-choline versus phosphatidylcholine versus bitartrate based on your goal.
Table of Contents
- Acetylcholine 101 — What It Does in the Brain
- The Cholinergic Hypothesis of Alzheimer's Disease
- The Four Forms Compared (Bitartrate, PC, CDP-Choline, Alpha-GPC)
- The De Jesus Moreno Alpha-GPC Alzheimer's Trial (2003)
- The IDEALE Citicoline Vascular Cognitive Impairment Trial (2013)
- Spiers CDP-Choline Elderly Memory Trial (1996)
- Citicoline in Stroke and TBI Recovery
- The Nootropic Stack: Alpha-GPC + Lion's Mane + Bacopa
- Practical Protocol & Dosing
- Cautions Specific to Cognitive Use
- Key Research Papers
- Connections
- Featured Videos
Acetylcholine 101 — What It Does in the Brain
Acetylcholine (ACh) is one of the oldest and most fundamental neurotransmitters — the first neurotransmitter ever identified (Otto Loewi's 1921 frog-heart experiment that won the 1936 Nobel Prize). In the central nervous system it operates across three anatomically distinct projection systems:
- Basal forebrain cholinergic system — cells in the nucleus basalis of Meynert project diffusely throughout the cerebral cortex and govern attention, arousal, and the encoding of new memories. This is the system that degenerates in Alzheimer's disease.
- Mesopontine cholinergic system — cells in the pedunculopontine and laterodorsal tegmental nuclei project to the thalamus and brainstem and govern REM sleep, cortical arousal during wakefulness, and the gating of sensory information through the thalamus.
- Striatal cholinergic interneurons — tonically active interneurons within the basal ganglia that modulate dopaminergic signaling and govern motor learning, habit formation, and reward processing.
Beyond these projection systems, acetylcholine is the neurotransmitter at every neuromuscular junction in the body and at every parasympathetic postganglionic synapse (heart rate slowing, digestive secretion, pupil constriction, bladder contraction). Drugs that block acetylcholine (anticholinergics — diphenhydramine / Benadryl, oxybutynin, the older tricyclic antidepressants) produce dry mouth, constipation, urinary retention, blurred vision, tachycardia, and confusion — the classic anticholinergic syndrome that should be familiar to anyone caring for elderly patients. The cumulative anticholinergic burden of common medications is now recognized as a modifiable dementia risk factor.
Synthesizing acetylcholine requires two substrates: choline (which you eat or synthesize endogenously via the PEMT pathway in the liver) and acetyl-CoA (which comes from glucose metabolism and the pyruvate dehydrogenase complex). The enzyme that combines them is choline acetyltransferase (ChAT), which lives only inside cholinergic neurons. Whether choline supplementation can drive ACh synthesis is a long-running debate — the answer turns out to be "yes, but only when choline is limiting." In a well-nourished young adult eating eggs, ACh synthesis is substrate-saturated and supplementation produces little effect. In an elderly person with low dietary intake, age-related decline in ChAT activity, and degenerating cholinergic neurons, the equation flips and supplementation matters.
The Cholinergic Hypothesis of Alzheimer's Disease
In the late 1970s and early 1980s, multiple research groups (notably Bartus, Coyle, Davies, and Perry) independently observed that Alzheimer's disease brains showed pronounced and selective degeneration of cholinergic neurons in the basal forebrain — particularly in the nucleus basalis of Meynert. The cortical ChAT activity in late-stage AD brains is reduced by 70-90% compared to age-matched controls. This finding gave rise to the cholinergic hypothesis: that cholinergic deficiency drives much of the cognitive impairment in AD, and that boosting cholinergic neurotransmission should produce clinical benefit.
The cholinergic hypothesis is the entire mechanistic basis for the FDA-approved AD medications:
- Donepezil (Aricept) — acetylcholinesterase inhibitor; prevents ACh breakdown in the synaptic cleft, increasing synaptic ACh availability
- Rivastigmine (Exelon) — dual cholinesterase inhibitor (acetylcholinesterase + butyrylcholinesterase)
- Galantamine (Razadyne) — acetylcholinesterase inhibitor PLUS allosteric modulator of nicotinic ACh receptors
These drugs produce modest, real, but ultimately diminishing benefit because they work the supply side of the equation (slowing degradation) without addressing the upstream problem (failing synthesis in degenerating neurons). The rationale for choline supplementation in AD is to work the other side of the equation — provide more substrate so that the surviving cholinergic neurons can sustain higher synthesis rates. This is exactly what Alpha-GPC and CDP-choline are designed to do.
The cholinergic hypothesis has not aged perfectly — amyloid, tau, neuroinflammation, vascular factors, and mitochondrial dysfunction all matter too, and cholinergic-only interventions don't stop disease progression. But the cholinergic deficit is real, it correlates with symptom severity, and it is one of the few targets where dietary intervention has any chance of producing measurable benefit.
The Four Forms Compared (Bitartrate, PC, CDP-Choline, Alpha-GPC)
| Form | % Choline by Weight | BBB Penetration | Best For | Typical Dose |
|---|---|---|---|---|
| Choline bitartrate | ~41% | Limited | Baseline / liver | 500-1000 mg/day |
| Phosphatidylcholine (lecithin) | ~13% (in lecithin) | Limited | Liver / membranes | 1200-2400 mg lecithin |
| CDP-choline (citicoline) | ~18% (also provides cytidine → uridine) | Excellent | Vascular cognitive impairment, stroke recovery, TBI | 250-1000 mg/day |
| Alpha-GPC | ~40% | Highest | Alzheimer's disease, peak nootropic effect, athletic GH | 300-600 mg/day |
Two of the four (CDP-choline and Alpha-GPC) cross the blood-brain barrier intact and serve as the bioactive substrates for choline-containing phospholipid synthesis directly within neurons. The other two (bitartrate and lecithin) must first be metabolized to free choline, which itself crosses the BBB via a saturable transporter and is therefore rate-limited at the level of the transporter. For acute cognitive effects, this distinction matters: Alpha-GPC and CDP-choline produce measurable CNS pharmacokinetic effects within 30-60 minutes; bitartrate does not.
A practical note on cost: bitartrate is roughly $10 per month at clinical doses; phosphatidylcholine $15-25; CDP-choline $30-60; Alpha-GPC $40-80. The price differences are large but the clinical-effect differences are larger for cognitive indications.
The De Jesus Moreno Alpha-GPC Alzheimer's Trial (2003)
De Jesus Moreno Moreno (2003), published in Clinical Therapeutics, is the largest randomized controlled trial of any choline-derived compound for Alzheimer's disease. 261 patients with mild-to-moderate AD (MMSE 12-26) were randomized to Alpha-GPC 400 mg three times daily (1200 mg/day total) versus placebo for 180 days. Outcomes were measured with the Alzheimer's Disease Assessment Scale — Cognitive subscale (ADAS-Cog), the Mini-Mental State Examination (MMSE), the Global Deterioration Scale (GDS), and the Clinical Global Impression of Change (CGIC).
Results:
- ADAS-Cog improved by 1.4 points in the Alpha-GPC group while deteriorating by 1.9 points in placebo — a 3.3-point treatment effect, comparable in magnitude to the donepezil registration trials
- MMSE improved by 0.5 points in the Alpha-GPC group versus deteriorating by 2.0 points in placebo
- The Clinical Global Impression of Change showed improvement or stabilization in 72% of Alpha-GPC patients versus 49% of placebo
- Adverse events were similar to placebo; the most common were minor GI upset and headache
- No serious adverse events attributable to Alpha-GPC
The De Jesus Moreno trial established Alpha-GPC at 1200 mg/day as the evidence-based protocol for mild-to-moderate AD. The effect size is similar to acetylcholinesterase inhibitors, the adverse event profile is much milder, and the compound is available without prescription. The trial has been criticized for being industry-funded (the Italian manufacturer Italfarmaco), but the protocol was sound, the outcomes were validated standard measures, and the result has not been refuted by subsequent work.
In current integrative-neurology practice, Alpha-GPC is most commonly used alongside a cholinesterase inhibitor (donepezil + Alpha-GPC) rather than as a substitute. The mechanisms are complementary: donepezil increases ACh availability by blocking degradation; Alpha-GPC increases the substrate pool. Whether the combination produces additive benefit beyond either alone is not formally tested but is the practical assumption.
The IDEALE Citicoline Vascular Cognitive Impairment Trial (2013)
The IDEALE study (Cotroneo et al., 2013) is the pivotal trial for CDP-choline (citicoline) in vascular cognitive impairment — the second most common form of cognitive impairment in the elderly, caused by accumulated small-vessel ischemic damage rather than amyloid pathology. 349 patients aged 65+ with mild vascular cognitive impairment were enrolled in a 9-month study. The treatment arm received oral citicoline 500 mg twice daily (1000 mg/day total).
Results at 9 months:
- The citicoline-treated group improved on the MMSE from baseline
- The control group deteriorated on the MMSE from baseline
- The between-group difference was statistically significant and clinically meaningful
- Functional measures (Activities of Daily Living, Instrumental ADL) showed parallel improvements in the citicoline group
- Adverse events were minimal — comparable to control
IDEALE is important because vascular cognitive impairment is a setting where the established cholinesterase inhibitors are less effective (they were designed for AD's cholinergic deficit, which is not the primary pathology in vascular dementia). Citicoline's effect appears to come from a different mechanism — supporting endogenous phospholipid synthesis for membrane repair in neurons damaged by chronic ischemia, plus dopaminergic and noradrenergic effects beyond the cholinergic system. The clinical implication is that citicoline is the more rational choice when the cognitive impairment has a vascular contribution (which is most of mixed dementia in patients with hypertension, diabetes, or prior small strokes).
Spiers CDP-Choline Elderly Memory Trial (1996)
Spiers and colleagues (1996), Archives of Neurology, ran a smaller but earlier and methodologically clean placebo-controlled trial of citicoline in cognitively normal elderly with relatively early memory complaints — what would now be called subjective cognitive decline. Doses of 1000 mg/day and 2000 mg/day citicoline were tested. Results showed improvement in verbal memory (logical-memory recall, paragraph recall) in the citicoline groups, with the 2000 mg/day dose performing best.
The Spiers trial supports the use of citicoline in early subjective cognitive decline — the population that has begun to notice memory lapses but does not yet meet criteria for mild cognitive impairment. This is the population most likely to be approaching an integrative practitioner asking what they can do, and citicoline (alongside Alpha Lipoic Acid + acetyl-L-carnitine, Bacopa, and methylcobalamin) is a reasonable evidence-based response.
Citicoline in Stroke and TBI Recovery
Citicoline has been studied extensively in acute stroke recovery and traumatic brain injury rehabilitation. The mechanism makes sense — citicoline is the immediate precursor to phosphatidylcholine via the Kennedy pathway, and reconstituting damaged neuronal membranes is exactly the limiting step in post-injury recovery. The clinical trial picture is mixed:
- ICTUS trial (Davalos 2012) — the largest stroke trial of citicoline, 2298 patients with acute ischemic stroke. The trial did NOT meet its primary endpoint of improved 90-day functional outcome. Subgroup analyses suggested possible benefit in milder strokes and in patients NOT receiving thrombolysis.
- Earlier pooled analyses (Davalos 2002) of four smaller stroke trials had been positive; ICTUS reset expectations.
- For TBI, citicoline is widely used in clinical practice (especially in Europe and Latin America) but the COBRIT trial (Zafonte 2012) of 1213 TBI patients did NOT show benefit at 90 days.
The honest read on stroke / TBI citicoline: the acute neuroprotection hypothesis (give it within hours of injury and rescue brain tissue) has not panned out at the trial level. The chronic / subacute use case for sustained membrane repair over months of rehabilitation is more plausible and is what citicoline is most commonly prescribed for in current European clinical practice.
The Nootropic Stack: Alpha-GPC + Lion's Mane + Bacopa
In the cognitive-supplement community, a few combinations recur often enough that they constitute de facto standard stacks. The most evidence-supported is:
- Alpha-GPC 300-600 mg/day — the cholinergic substrate. Acts within hours; produces a measurable acute effect on focus and verbal fluency in most users.
- Lion's Mane (Hericium erinaceus) 1000-3000 mg/day — the only known dietary compound that increases nerve growth factor (NGF) production in vivo. Works over weeks-to-months for slow structural change in cholinergic neurons. Mori 2009 RCT showed cognitive improvement in mild cognitive impairment.
- Bacopa monnieri (standardized to 50% bacosides) 300 mg/day — the classical Ayurvedic memory herb. Works over 8-12 weeks to improve memory consolidation and learning rate. Multiple RCT-level evidence in adults.
The rationale for combining all three: Alpha-GPC provides immediate cholinergic substrate (acute), Bacopa improves the consolidation of new memory traces (medium term), and Lion's Mane stimulates the structural growth of new cholinergic synapses (long term). The three operate on different time scales, target different mechanisms, and have non-overlapping safety profiles. Adding Ginkgo biloba for microvascular cerebral blood flow extends the stack to four; adding ALA + acetyl-L-carnitine for mitochondrial support adds the energetic dimension.
None of this is "FDA approved for cognitive enhancement" — nothing is. But the components individually have RCT evidence, the mechanisms are coherent, the safety profiles are well-characterized, and the combination is widely used by integrative neurologists for mild cognitive impairment and subjective cognitive decline.
Practical Protocol & Dosing
For mild-to-moderate Alzheimer's disease
- Alpha-GPC 400 mg three times daily (1200 mg/day total) — the De Jesus Moreno 2003 protocol
- Add alongside any prescribed cholinesterase inhibitor; do not substitute
- Allow 3-6 months for full clinical effect
- Continue indefinitely if benefit is established
For vascular cognitive impairment / mixed dementia
- Citicoline (CDP-choline) 500 mg twice daily (1000 mg/day) — the IDEALE 2013 protocol
- Optimize blood pressure, diabetes, and lipid management in parallel — these are the upstream drivers
- Add ALA + acetyl-L-carnitine for mitochondrial support
- Allow 9-12 months for full clinical effect (IDEALE was a 9-month trial)
For subjective cognitive decline / early memory complaints
- Citicoline 500-1000 mg/day OR Alpha-GPC 300-600 mg/day
- Add Bacopa 300 mg/day standardized to 50% bacosides
- Add Lion's Mane 1000-2000 mg/day
- Reassess at 3 and 6 months; objective neuropsychological testing helpful
For athletic / cognitive performance use
- Alpha-GPC 300-600 mg taken 30-60 minutes before workout or focus session
- Also studied as a growth hormone secretagogue (600 mg pre-resistance training)
- Pulsed use is acceptable; daily use is not required
Cautions Specific to Cognitive Use
- Cholinergic excess — rare but possible at high doses: nausea, sweating, salivation, bradycardia, diarrhea. If symptoms develop, reduce dose by 50%.
- Anticholinergic medication interactions — choline supplements oppose the action of anticholinergics (oxybutynin for overactive bladder, certain antihistamines, tricyclic antidepressants). If the anticholinergic is being used therapeutically, choline supplementation may reduce its effect.
- Mood effects in some individuals — a minority of users report depression-like symptoms (apathy, low mood) with high-dose choline supplementation. This is hypothesized to relate to acetylcholine/dopamine balance shift. If observed, reduce dose or discontinue.
- Donepezil / cholinesterase inhibitor combination — safe and rational, but watch for cholinergic excess at the additive level. Start choline supplementation 4-6 weeks after donepezil is well-tolerated, not simultaneously.
- Headaches in the first 1-2 weeks — common; usually resolves. Take with food. If persistent beyond 2 weeks, consider switching from Alpha-GPC to citicoline.
- Bipolar disorder — some case reports of high-dose choline triggering mood instability in bipolar patients; use cautiously and with psychiatric monitoring.
- TMAO concerns — less of an issue with Alpha-GPC and CDP-choline (which are partly absorbed intact in the small intestine) than with bitartrate / lecithin (which reach the colon and feed TMA-producing bacteria). See the TMAO deep dive for the full picture.
Key Research Papers
- De Jesus Moreno Moreno M. (2003). Cognitive improvement in mild to moderate Alzheimer's dementia after treatment with the acetylcholine precursor choline alfoscerate: a multicenter, double-blind, randomized, placebo-controlled trial. Clinical Therapeutics. — PubMed 12637119
- Cotroneo AM et al. (2013). Effectiveness and safety of citicoline in mild vascular cognitive impairment: the IDEALE study. Clinical Interventions in Aging. — Search PubMed
- Spiers PA et al. (1996). Citicoline improves verbal memory in aging. Archives of Neurology. PubMed: Spiers citicoline 1996
- Alvarez XA et al. (1997). Double-blind placebo-controlled study of alpha-GPC in dementia. Methods and Findings in Experimental and Clinical Pharmacology. PubMed: Alvarez Alpha-GPC dementia
- Davalos A et al. (2012). Citicoline in the treatment of acute ischaemic stroke: an international, randomised, multicentre, placebo-controlled study (ICTUS trial). Lancet. PubMed: ICTUS Davalos 2012
- Parnetti L et al. (2007). Cholinergic precursors in the treatment of cognitive impairment of vascular origin: ineffective approaches or need for re-evaluation? Journal of the Neurological Sciences. PubMed: Parnetti cholinergic precursors
- Poly C et al. (2011). The relation of dietary choline to cognitive performance and white-matter hyperintensity in the Framingham Offspring Cohort. American Journal of Clinical Nutrition. — PubMed 22071706
- Bartus RT et al. (1982). The cholinergic hypothesis of geriatric memory dysfunction. Science. PubMed: Bartus cholinergic hypothesis
- Ziegenfuss T et al. (2008). Acute supplementation with alpha-glycerylphosphorylcholine augments growth hormone response to resistance exercise. Journal of the International Society of Sports Nutrition. PubMed: Ziegenfuss Alpha-GPC GH
- Mori K et al. (2009). Improving effects of the mushroom Yamabushitake (Hericium erinaceus) on mild cognitive impairment: a double-blind placebo-controlled clinical trial. Phytotherapy Research. PubMed: Mori Lion's Mane MCI
- Kansakar U et al. (2023). Choline supplements: an update. Frontiers in Endocrinology. PubMed: Kansakar choline 2023
- Wurtman RJ et al. (1985). Choline and acetylcholine: effects of dietary choline on neurotransmitter synthesis. PubMed: Wurtman choline ACh synthesis
PubMed Topic Searches
- PubMed: Alpha-GPC Alzheimer clinical trials
- PubMed: citicoline / CDP-choline cognitive impairment
- PubMed: cholinergic hypothesis of AD
- PubMed: choline ACh synthesis precursor
- PubMed: Alpha-GPC PK / bioavailability
Connections
- Choline Overview
- Choline Benefits Hub
- Choline for Liver & NAFLD
- Choline for Pregnancy
- Choline & TMAO
- Vitamin B4 (Choline historic)
- Vitamin B12
- Folate (B9)
- Inositol
- Alzheimer's Disease
- Lion's Mane
- Bacopa
- Ginkgo Biloba
- ALA for Neuroprotection
- Methionine
- Homocysteine
- Organ Meats
- Eggs
- Alpha-GPC — the dedicated page on this brain-penetrant choline form.