GLP-1 Receptor Agonists: Ozempic, Wegovy, Mounjaro, Zepbound — Mechanisms, Benefits, and Risks



Few classes of medication in modern history have reshaped public conversation about metabolic health as rapidly as the glucagon-like peptide-1 receptor agonists (GLP-1 RAs). Originally developed to help people with type 2 diabetes control blood sugar, drugs like semaglutide (Ozempic, Wegovy, Rybelsus) and the dual GIP/GLP-1 agonist tirzepatide (Mounjaro, Zepbound) have produced weight-loss results that were, until recently, only achievable through bariatric surgery. They have also demonstrated meaningful reductions in cardiovascular events, kidney disease progression, fatty liver inflammation, and obstructive sleep apnea severity, while ongoing studies examine their potential effects on alcohol use disorder, Parkinson’s disease, and Alzheimer’s dementia.
This article explains what these drugs are, how they interact with the body’s native appetite and glucose-regulation systems, what the clinical evidence shows across each major indication, what the real side-effect and safety profile looks like, who should avoid them, and what the key practical considerations — from muscle-mass preservation to rebound weight regain to compounded versions — mean for anyone considering treatment. As always, this information is educational and is not a substitute for evaluation by a qualified medical professional.
Interactive Visualization Hunger, Leptin & Why Diets Fight Back Watch the hunger neurons and the fullness neurons fight it out — then lose weight and see leptin fall, hunger climb and metabolism drop. It isn’t willpower. It’s a defended system. Launch →Table of Contents
- What GLP-1 Is — The Native Hormone
- How GLP-1 Receptor Agonists Work
- The Drug Lineup — Semaglutide, Tirzepatide, Liraglutide, and What’s Coming
- Type 2 Diabetes Control
- Weight Loss
- Cardiovascular Protection
- Kidney Disease
- Fatty Liver Disease (MASLD/MASH)
- Obstructive Sleep Apnea
- Addiction, Alcohol Use, and Neurological Research
- Side Effects and Risks
- Who Should Not Use GLP-1 Agonists
- Muscle Mass Loss and How to Prevent It
- Rebound Weight Regain After Stopping
- Compounded GLP-1s and the Legal Landscape
- Cost, Insurance, and Access
- Natural and Complementary Strategies
- The Bigger Picture for Healthcare
- Connections
- Research Papers
- Featured Videos
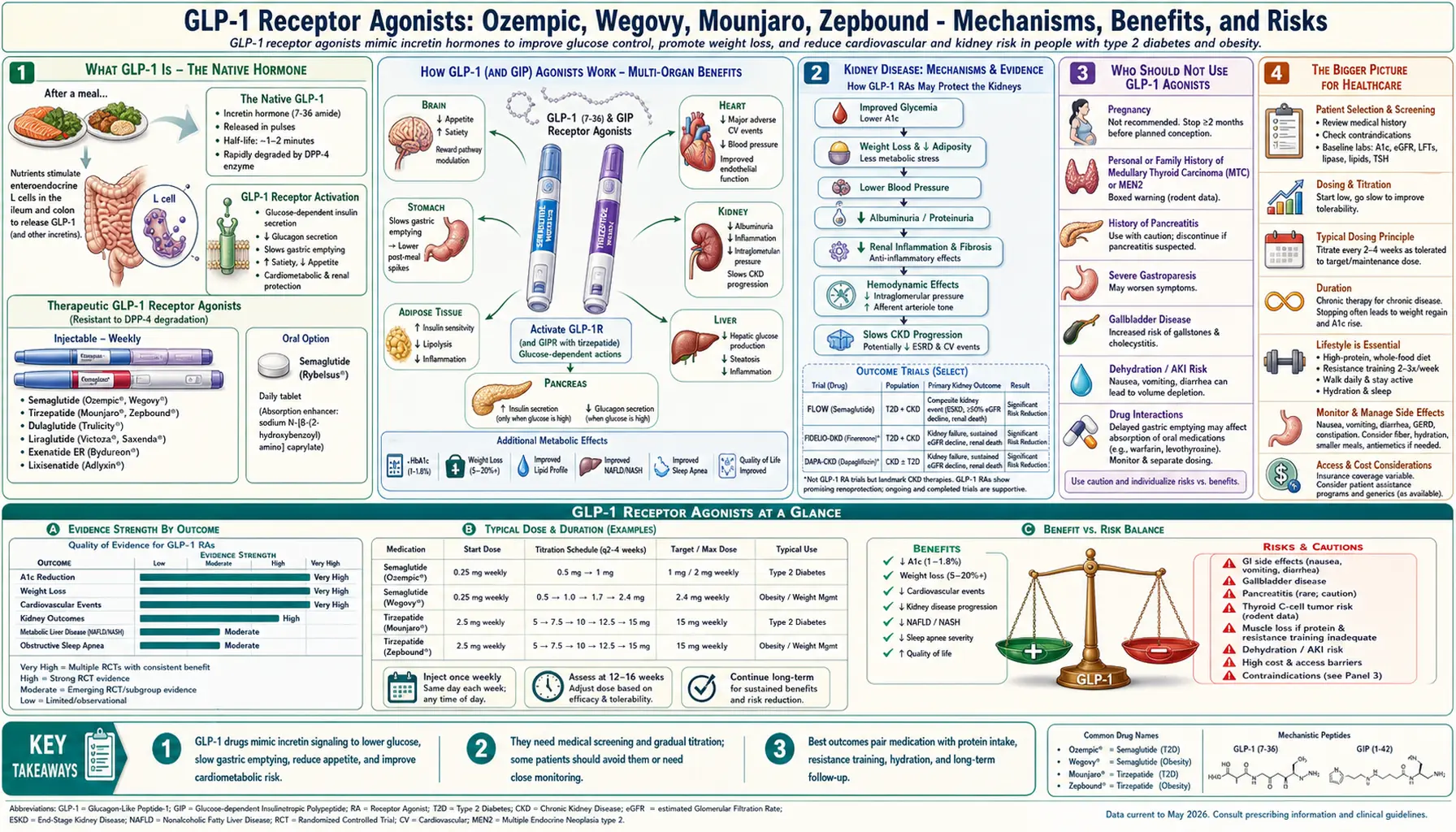
What GLP-1 Is — The Native Hormone
Glucagon-like peptide-1 (GLP-1) is an incretin hormone — a gut-derived peptide released by specialized L-cells in the ileum and colon in response to nutrient arrival, particularly carbohydrates, fats, and certain amino acids and bile acids. Within minutes of eating, GLP-1 rises in the bloodstream and participates in a tightly coordinated cascade of post-meal biological events: it signals the pancreas to release insulin in a glucose-dependent manner (meaning insulin release only occurs when blood sugar is actually elevated), it suppresses the counter-regulatory hormone glucagon, it slows the rate at which the stomach empties its contents into the small intestine, and — most importantly for appetite — it travels to the brainstem and hypothalamus, where it signals satiety and reduces the desire to continue eating.
In people with type 2 diabetes and many with obesity, endogenous GLP-1 signaling is blunted. The hormone is secreted less, its effect on the pancreas is weakened, and its satiety signal reaching the hypothalamus is attenuated. Native GLP-1 also has an extraordinarily short half-life — roughly one to two minutes — because it is rapidly inactivated by the enzyme dipeptidyl peptidase-4 (DPP-4). This means simply administering GLP-1 itself as a drug would require constant infusion to achieve a clinical effect. Pharmaceutical chemists solved this problem by engineering synthetic peptides that bind the GLP-1 receptor but resist DPP-4 degradation, giving them half-lives measured in hours or days rather than minutes.
How GLP-1 Receptor Agonists Work
A GLP-1 receptor agonist is a drug that binds the same receptor as the native hormone but stays active far longer. The major mechanisms, acting simultaneously, are:
- Central appetite suppression. The drug crosses into circumventricular regions of the brain such as the area postrema and the arcuate nucleus of the hypothalamus, activating pro-opiomelanocortin (POMC) neurons that generate satiety and reducing activity of neuropeptide-Y / agouti-related peptide neurons that drive hunger. Patients consistently report reduced “food noise” — the intrusive, pre-occupying thoughts about food that characterize obesity for many people.
- Delayed gastric emptying. Food leaves the stomach more slowly, prolonging fullness after meals and reducing the post-meal blood-sugar spike. Over time, tachyphylaxis (tolerance) to this effect tends to develop, so early nausea often fades.
- Glucose-dependent insulin secretion. Pancreatic beta cells release more insulin in response to meal-related glucose rises, but only when glucose is high. This glucose-dependency is why GLP-1 RAs rarely cause hypoglycemia when used alone — unlike insulin or sulfonylureas.
- Glucagon suppression. Pancreatic alpha cells release less glucagon, reducing the liver’s production of glucose between meals.
- Effects on reward and cravings. GLP-1 receptors are also present in mesolimbic dopamine pathways. Activation there appears to reduce reward-driven overeating and, in emerging studies, reduce cravings for alcohol and nicotine.
Tirzepatide (Mounjaro, Zepbound) goes one step further by activating both the GLP-1 receptor and the receptor for glucose-dependent insulinotropic polypeptide (GIP), the other major incretin hormone. In head-to-head trials, this dual mechanism has produced greater weight loss and greater A1C reduction than single-agonist semaglutide at comparable doses.
The Drug Lineup — Semaglutide, Tirzepatide, Liraglutide, and What’s Coming
The currently available GLP-1 and related incretin drugs include:
- Semaglutide — weekly subcutaneous injection. Branded as Ozempic for type 2 diabetes, Wegovy for chronic weight management, and Rybelsus as an oral daily tablet. Developed by Novo Nordisk.
- Tirzepatide — weekly subcutaneous injection, dual GIP/GLP-1 agonist. Branded as Mounjaro for type 2 diabetes and Zepbound for chronic weight management and obstructive sleep apnea. Developed by Eli Lilly.
- Liraglutide — once-daily injection, first-generation. Branded as Victoza for diabetes and Saxenda for weight management. Produces more modest weight loss than the newer weekly drugs but is available as a generic in many markets, lowering cost.
- Dulaglutide (Trulicity), exenatide (Byetta, Bydureon), and lixisenatide (Adlyxin) — earlier GLP-1 RAs, largely eclipsed by semaglutide and tirzepatide on efficacy.
Several next-generation drugs are in late-stage trials. Retatrutide is a triple agonist targeting GLP-1, GIP, and the glucagon receptor, which in early data has produced weight loss approaching 24% of body weight. Oral semaglutide and oral tirzepatide in higher doses are in development to eliminate the need for injection. CagriSema, which combines semaglutide with the amylin analogue cagrilintide, is also advancing.
Type 2 Diabetes Control
GLP-1 RAs have become first-line or near-first-line therapy for type 2 diabetes, particularly in patients with cardiovascular disease, kidney disease, or obesity. In clinical trials, semaglutide and tirzepatide have lowered HbA1c by 1.5% to 2.5% on average — a magnitude comparable to or exceeding multiple older oral medications combined — while producing simultaneous weight loss, an advantage that sulfonylureas, insulin, and thiazolidinediones lack. Because GLP-1-stimulated insulin release is glucose-dependent, the risk of hypoglycemia as a monotherapy is low. Risk rises if these drugs are combined with insulin or sulfonylureas, and doses of those companion drugs often need to be reduced when a GLP-1 RA is added.
Weight Loss
In the STEP trial program for semaglutide 2.4 mg (Wegovy), participants without diabetes lost an average of 15% of their body weight over 68 weeks — roughly double the weight loss of prior-generation obesity medications. In the SURMOUNT-1 trial for tirzepatide 15 mg (Zepbound), participants lost an average of 21% of body weight over 72 weeks, with roughly 57% of patients on the highest dose losing at least one-fifth of their starting weight. For comparison, a Roux-en-Y gastric bypass typically produces 25 to 30 percent weight loss.
Weight loss from GLP-1 agonists is achieved primarily through reduced caloric intake. Measured energy intake in treated patients falls by roughly 30 to 40 percent without deliberate calorie-counting, an effect consistent with the mechanism of appetite suppression rather than any direct effect on metabolic rate. The drugs do not burn fat — they reduce the drive to overeat.
Cardiovascular Protection
The SELECT trial, published in 2023, was the first large cardiovascular outcomes trial of a GLP-1 agonist in people with overweight or obesity but without diabetes. Over roughly three years, semaglutide 2.4 mg reduced the composite of cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke by 20% compared with placebo. This was a landmark result because it extended the case for GLP-1 therapy beyond glycemic control: the benefit appeared to begin before most participants had lost substantial weight, suggesting direct anti-inflammatory and vascular effects beyond weight reduction alone.
Earlier diabetes-outcomes trials — LEADER (liraglutide), SUSTAIN-6 (semaglutide injectable), and REWIND (dulaglutide) — had already shown significant reductions in major adverse cardiovascular events in people with diabetes. The FLOW trial and newer analyses suggest heart failure hospitalizations are also reduced, particularly in heart failure with preserved ejection fraction.
Kidney Disease
The FLOW trial, published in 2024, tested semaglutide in people with type 2 diabetes and chronic kidney disease and found a 24% reduction in the composite endpoint of kidney failure, substantial loss of kidney function, and death from cardiovascular or kidney causes. The magnitude of renal benefit places GLP-1 RAs alongside SGLT2 inhibitors (such as empagliflozin and dapagliflozin) as the second major drug class with clear disease-modifying effects on diabetic kidney disease. Mechanistically, the benefit appears to come from a combination of reduced glomerular hyperfiltration, reduced inflammation, lowered blood pressure, and improved glycemic and weight control.
Fatty Liver Disease (MASLD/MASH)
Metabolic dysfunction-associated steatotic liver disease (MASLD) — formerly called non-alcoholic fatty liver disease — and its inflammatory stage, MASH, are strongly tied to insulin resistance, visceral adiposity, and type 2 diabetes. GLP-1 RAs reduce liver fat content on MRI-proton density fat fraction imaging and have produced histological resolution of steatohepatitis in a substantial subset of patients in biopsy-controlled trials. Semaglutide and tirzepatide are both under investigation specifically for MASH, with tirzepatide having shown resolution of MASH without worsening of fibrosis in a significant proportion of patients in the SYNERGY-NASH trial.
Obstructive Sleep Apnea
In 2024, tirzepatide became the first pharmaceutical treatment to receive FDA approval for obstructive sleep apnea in adults with obesity, based on the SURMOUNT-OSA trial. Participants saw a roughly 50 percent reduction in apnea-hypopnea index (the key severity measure), alongside significant weight loss, blood pressure reduction, and improved sleep-related symptoms. For patients with moderate-to-severe OSA driven by obesity, this opens a pharmacological path that complements or partially replaces CPAP therapy.
Addiction, Alcohol Use, and Neurological Research
A striking off-target observation in real-world and emerging trial data is that people taking GLP-1 agonists often report reduced cravings for alcohol, nicotine, and other substances. Pharmacoepidemiologic studies have shown lower rates of alcohol-related hospital visits in patients on semaglutide; preliminary randomized trials suggest genuine reductions in heavy drinking. Research is also active in Parkinson’s disease, where earlier small trials of exenatide suggested possible slowing of motor decline, and in Alzheimer’s dementia, where the EVOKE and EVOKE Plus trials of oral semaglutide are testing cognitive and functional outcomes in early-stage patients. These remain investigational and no GLP-1 drug is approved for neurological indications as of this writing.
Side Effects and Risks
The most common adverse effects are gastrointestinal and usually mildest at the lowest dose and during early titration:
- Nausea, vomiting, and constipation. The most common reasons for discontinuation. Slow dose escalation, smaller meals, avoidance of high-fat or very rich foods, and adequate hydration all help.
- Diarrhea or delayed stomach emptying. Some patients develop persistent gastroparesis-like symptoms even after stopping the drug.
- Injection-site reactions. Mild redness or nodule formation, usually self-limiting.
- Gallbladder disease. Rapid weight loss from any cause, including these drugs, raises risk of cholelithiasis and acute cholecystitis.
- Acute pancreatitis. Rare but reported. People with prior pancreatitis should exercise caution.
- Thyroid C-cell tumors. Seen in rodent studies at high doses; a black-box warning applies. Human data do not clearly support an increased risk, but the drugs are contraindicated in people with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia type 2.
- Aspiration risk during anesthesia. Because gastric emptying is delayed, many surgical guidelines now recommend holding the drug for at least one week before procedures requiring general anesthesia.
- Diabetic retinopathy progression. Observed in people with pre-existing retinopathy during rapid glycemic normalization; not unique to GLP-1 RAs.
- Mood changes and suicidality. Post-marketing signals prompted regulatory reviews. The European Medicines Agency and FDA have not concluded that a causal link exists, but patients with significant psychiatric history should be monitored.
Who Should Not Use GLP-1 Agonists
These drugs are generally avoided in:
- People with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia type 2 (MEN2).
- People with a history of pancreatitis, particularly recurrent or unresolved.
- People with active or severe gastroparesis or other serious gastrointestinal motility disorders.
- Pregnancy and breastfeeding. GLP-1 RAs should be discontinued at least two months before a planned pregnancy because of their long half-life.
- Children below the age ranges studied in trials, absent specific pediatric indications (liraglutide and semaglutide have some adolescent approvals).
- People with low baseline body weight, eating disorders, or other conditions where further appetite reduction or weight loss is clinically inappropriate.
Muscle Mass Loss and How to Prevent It
One of the most important — and widely under-discussed — issues with GLP-1 therapy is that weight lost is not purely fat. In rapid weight-loss trials, roughly 25 to 40 percent of the mass lost is lean body tissue, including skeletal muscle. In older adults or those already at risk of sarcopenia, this can worsen functional capacity, insulin sensitivity, and long-term metabolic health.
Evidence-based strategies to preserve muscle during treatment:
- Resistance training. At least two to three sessions per week covering all major muscle groups. This is the single most important intervention and can reduce lean-mass loss by roughly half in controlled studies.
- Adequate protein intake. Aim for approximately 1.2 to 1.6 grams of protein per kilogram of goal body weight daily, distributed across meals. Because appetite is reduced, this often requires deliberate planning — protein-first meals, shakes, or high-protein foods.
- Sufficient total calories. Avoid extreme voluntary restriction on top of the drug’s already substantial appetite suppression.
- Creatine monohydrate. Roughly 3 to 5 grams daily supports muscle mass and performance during caloric deficit and is well-studied and inexpensive.
- Leucine-rich amino acids. Leucine is the primary amino-acid trigger for muscle protein synthesis; whey protein and animal proteins are rich sources.
Rebound Weight Regain After Stopping
When GLP-1 therapy is stopped, the underlying biology of appetite regulation returns to its pre-treatment setpoint. In the STEP 4 and STEP 1 extension trials, participants who discontinued semaglutide regained roughly two-thirds of their lost weight within one year. This pattern mirrors the regain seen after most non-surgical weight interventions and reflects the fact that obesity is a chronic, relapsing condition rather than a one-time event.
The practical implication is that, for many patients, GLP-1 therapy is likely to be a long-term or lifelong medication rather than a short course. Minimum-effective-dose strategies — tapering down to the lowest dose that maintains weight loss — are being studied but have limited evidence so far. Intensive lifestyle support during and after the drug significantly improves maintenance outcomes.
Compounded GLP-1s and the Legal Landscape
During the 2022–2024 shortage of semaglutide and tirzepatide, U.S. compounding pharmacies were permitted to prepare custom versions of these drugs under FDA rules that apply when a brand-name drug is on the official shortage list. This produced a parallel market of compounded injectables, often paired with vitamin B12 or other additives, sold through telemedicine platforms at a fraction of brand-name pricing.
With the FDA removing both semaglutide and tirzepatide from their shortage lists in 2024 and 2025, the legal basis for routine large-scale compounding has narrowed significantly. Compounded versions may still be produced for individual patients with specific documented clinical needs, but large telehealth compounders face ongoing legal and regulatory pressure. Quality concerns — including inconsistent dosing, contamination, and use of unapproved salt forms — have been documented in some compounded products. Patients considering these options should verify the pharmacy’s credentials, understand what active ingredient form is being used, and recognize that safety and efficacy data for branded drugs do not directly transfer to compounded versions.
Cost, Insurance, and Access
U.S. list prices for branded GLP-1 RAs remain in the range of $1,000 to $1,400 per month without insurance or manufacturer programs, making access a central policy question. Medicare currently covers these drugs for diabetes but not for weight loss alone, though CMS has begun paying for them when prescribed for cardiovascular risk reduction in people with obesity following the SELECT trial result. Many employer-sponsored commercial plans now cover weight-loss indications, often with step-therapy requirements and BMI thresholds. Manufacturer savings cards and patient-assistance programs can substantially reduce out-of-pocket cost for the insured. Internationally, prices vary by roughly five- to tenfold between the U.S. and comparable high-income countries, driving substantial cross-border purchasing.
Natural and Complementary Strategies
No natural product replicates the magnitude of GLP-1 RA effects, but several approaches meaningfully support endogenous GLP-1 signaling, metabolic health, and appetite regulation. These can be useful adjuncts during therapy, stepdown strategies after discontinuation, or first-line interventions for those who prefer a non-pharmacological approach.
- Fiber, especially viscous soluble fiber. Beta-glucans from oats and barley, psyllium, and acacia fiber all stimulate L-cell GLP-1 release through short-chain fatty acid production by gut microbes.
- Protein-forward meals. Protein is the strongest macronutrient trigger for native GLP-1 and has the highest satiety-per-calorie of any macronutrient.
- Fermented foods and probiotics. Specific strains influence incretin secretion and insulin sensitivity.
- Berberine. Often called “nature’s Ozempic” in popular media — an overstatement, but it does improve insulin sensitivity, modestly lower HbA1c, and support blood-sugar control through AMPK activation. See our dedicated Berberine article for detail.
- Polyphenol-rich foods. Olive oil, green tea, dark chocolate, and berries support postprandial glucose control and incretin response.
- Strength training and sleep. Both independently improve insulin sensitivity and appetite regulation.
- Time-restricted eating. Compressing the eating window to 8–10 hours supports metabolic flexibility in many people. See Fasting.
The Bigger Picture for Healthcare
GLP-1 receptor agonists are reshaping the pharmaceutical landscape in a way that has few recent precedents. They represent the first drug class to produce surgery-comparable weight loss with acceptable outpatient safety, and their cardiovascular, renal, and hepatic benefits suggest they are treating something deeper than body weight — likely the metabolic-inflammatory axis that connects obesity, diabetes, cardiovascular disease, kidney disease, and fatty liver disease into a single clinical phenotype.
The unresolved questions are significant. Long-term effects over decades of use remain uncharacterized. The fiscal impact on healthcare systems if these drugs become standard of care for the entire population with BMI over 30 is enormous. Muscle preservation protocols are under-implemented. Rebound regain after discontinuation remains a dominant clinical reality. And the off-target benefits — if confirmed — in addiction, neurodegeneration, and even cancer biology could transform how these drugs are positioned.
For individuals, the sensible framework is to treat GLP-1 agonists as powerful tools that work best when paired with resistance training, adequate protein, whole-food nutrition, sleep, and a realistic expectation that durable weight loss typically requires durable therapy. The decision to start or stay on treatment is a nuanced clinical conversation between patient and clinician, informed by individual risk, benefit, preference, and life context.
Connections
- Hunger, Leptin & Why Diets Fight Back — interactive animation
- Lactulose
- Berberine
- Fasting
- Diabetes
- Obesity
- Kidney Disease
- Obstructive Sleep Apnea
- Blood Sugar
- Cardiovascular Disease
- Non-Alcoholic Fatty Liver Disease
- NAD/NMN
- Hemoglobin A1C
- Longevity Protocols
- Anti-Inflammatory Diet
- Fasting Insulin
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Lipid Panel
- Insulin Resistance
Research Papers
- Semaglutide and weight loss — PubMed search
- Tirzepatide clinical trials — PubMed search
- GLP-1 agonists and cardiovascular outcomes — PubMed search
- GLP-1 agonists and kidney disease (FLOW) — PubMed search
- GLP-1 agonists in MASH/fatty liver — PubMed search
- Semaglutide and alcohol use disorder — PubMed search
- GLP-1 agonists and muscle mass loss — PubMed search
- Weight regain after GLP-1 discontinuation — PubMed search