GLP-1 Receptor Agonists — Side Effects and Cautions
GLP-1 receptor agonists carry an FDA black-box warning for medullary thyroid carcinoma based on rodent thyroid C-cell tumors, an absolute contraindication in patients with personal or family history of MTC or MEN-2 syndrome, a real but disputed pancreatitis signal, a well-documented gallbladder disease signal, a pre-operative aspiration risk that has changed anesthesia practice guidance, an emerging NAION (non-arteritic anterior ischemic optic neuropathy) ophthalmologic signal from JAMA Ophthalmology 2024, a substantial lean-mass loss component that requires resistance training and protein optimization, the near-universal nausea/vomiting cluster that drives 7–15% discontinuation, and an EMA-investigated suicidal-ideation signal that has not yet been confirmed in large pharmacovigilance studies. Layered onto these is the rebound problem — two thirds of weight regained within a year of discontinuation — that makes therapy effectively indefinite.
Interactive Visualization Hunger, Leptin & Why Diets Fight Back Watch the hunger neurons and the fullness neurons fight it out — then lose weight and see leptin fall, hunger climb and metabolism drop. It isn’t willpower. It’s a defended system. Launch →
Table of Contents
- Gastrointestinal Side Effects (Most Common)
- Thyroid C-Cell / Medullary Thyroid Carcinoma Warning
- Pancreatitis Signal
- Gastroparesis and Pre-Operative Aspiration
- Gallbladder Disease
- NAION (Anterior Ischemic Optic Neuropathy)
- Lean-Mass Loss
- Suicidal Ideation Signal (Disputed)
- Pregnancy, Lactation, and Renal Considerations
- Discontinuation and Rebound
- Key Research Papers
- Connections
- Featured Videos
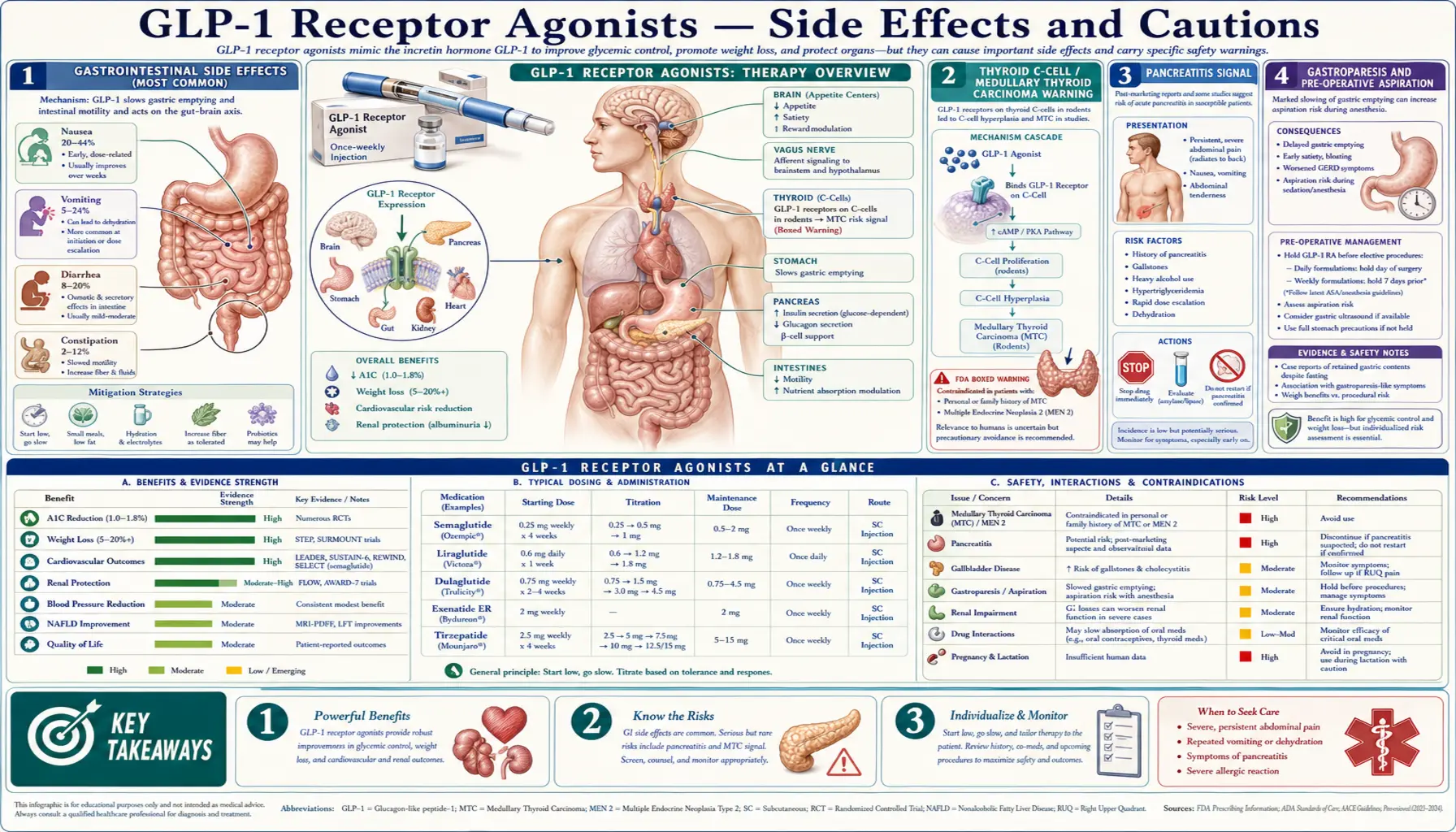
Gastrointestinal Side Effects (Most Common)
Nausea, vomiting, diarrhea, and constipation are by far the most common adverse events. Pooled trial data show nausea in 44–75% of patients, vomiting in 18–30%, diarrhea in 20–30%, and constipation in 17–25%. The frequency is highest during the 16–20 week dose-escalation phase and attenuates with continued exposure as gastric emptying tolerance develops. Severity is usually mild to moderate; severe GI symptoms accounting for trial discontinuation occur in 5–9% of patients.
Practical mitigations: slow titration (the standard 4-week dose-step schedule, with permission to extend if symptoms are prominent); smaller meals; lower fat and lower fiber content during titration; avoiding the late-evening meal; staying upright after eating; and adequate hydration. Many physicians use anti-emetics (ondansetron, promethazine) during the worst weeks of titration, accepting the trade-off of constipation. If symptoms remain intolerable at a given dose, stepping back one dose and re-titrating more slowly is the standard approach.
Thyroid C-Cell / Medullary Thyroid Carcinoma Warning
All injectable GLP-1 receptor agonists in the United States (liraglutide, exenatide ER, dulaglutide, semaglutide, tirzepatide) carry an FDA black-box warning for medullary thyroid carcinoma (MTC) and an absolute contraindication in patients with personal or family history of MTC or multiple endocrine neoplasia syndrome type 2 (MEN-2). The warning is based on the finding that prolonged GLP-1 receptor agonist exposure caused thyroid C-cell hyperplasia and C-cell tumors (both benign and malignant) in rats and mice across multiple studies (Bjerre Knudsen 2010, Endocrinology).
The translation of this rodent finding to human risk is debated. Rodent thyroid C-cells express GLP-1 receptor abundantly, whereas human thyroid C-cells express it at much lower density. Post-marketing pharmacovigilance has not produced consistent evidence of an MTC signal in humans. A 2023 French cohort study (Bezin et al., Diabetes Care) found a modest association between GLP-1 RA exposure and thyroid cancer (HR ~1.6 for all thyroid cancer, ~1.8 for MTC), but interpretation is complicated by surveillance bias and a small absolute number of MTC cases.
The practical clinical posture: ask about personal or family history of MTC or MEN-2 before prescribing; if present, choose a different drug class; for any patient on therapy who develops a thyroid nodule, hoarseness, dysphagia, or persistent neck mass, work up promptly with ultrasound and calcitonin measurement. Routine baseline or surveillance calcitonin in the general patient population is not recommended.
Pancreatitis Signal
An acute pancreatitis signal has been the most contentious GLP-1 RA safety question since the class was introduced. Early case-control studies (Singh, JAMA Intern Med 2013) reported approximately twofold increased risk of pancreatitis hospitalization with exenatide or sitagliptin. Subsequent meta-analyses of randomized trials (LEADER, SUSTAIN-6, EXSCEL, REWIND, PIONEER 6) found numerically more pancreatitis events on GLP-1 RA than placebo but with absolute risk increases of less than 1 per 1,000 patient-years and confidence intervals that crossed 1.0. The 2023 Sodhi JAMA paper using IQVIA real-world data reported a 9.1-fold increase in pancreatitis with GLP-1 RA vs bupropion-naltrexone for obesity, reigniting the debate.
Mechanism is plausible: GLP-1 receptors are expressed on the exocrine pancreas and pancreatic ductal cells, and chronic activation could drive low-grade ductal proliferation. The practical clinical posture: patients with a history of pancreatitis should be advised that the residual risk on GLP-1 RA is uncertain and probably increased, and an alternative drug class should be considered. For any patient on therapy who develops persistent severe upper abdominal pain, the drug should be held and lipase / amylase / imaging obtained promptly. Acute pancreatitis on a GLP-1 RA is an indication to discontinue and not rechallenge.
Gastroparesis and Pre-Operative Aspiration
The same delayed gastric emptying that drives satiety also creates an aspiration risk during anesthesia. Beginning in 2022, multiple case reports of retained gastric content despite extended pre-operative fasting were published in patients on semaglutide or tirzepatide, with several reports of intraoperative aspiration leading to pneumonia or death. Sherwin et al. (2023) documented residual gastric content on ultrasound in patients fasted to current ASA guidelines while on GLP-1 RA.
The American Society of Anesthesiologists issued guidance in mid-2023 (updated in 2024) recommending:
- Daily GLP-1 RA (liraglutide): hold for at least 24 hours before elective surgery requiring sedation or general anesthesia.
- Weekly GLP-1 RA (semaglutide, dulaglutide, tirzepatide, exenatide ER): hold for at least 7 days — one full dosing interval — before elective surgery.
- If unable to hold: consider treating as a "full stomach" with rapid-sequence induction, gastric ultrasound assessment, or postponement.
- Endoscopy: particularly upper endoscopy and colonoscopy require similar consideration; clear-liquid diet for 24 hours before procedure is often added.
Patients must inform anesthesia providers in advance of any GLP-1 RA use; the medication is often not in primary care med-list summaries forwarded to the surgical team and is frequently missed.
Gallbladder Disease
GLP-1 receptor agonists modestly but consistently increase risk of cholelithiasis (gallstones), cholecystitis, and biliary disease requiring intervention. The Faillie 2022 JAMA Intern Med meta-analysis pooled 76 randomized trials (over 100,000 patients) and found a relative risk of 1.37 for any gallbladder or biliary disease, with a number-needed-to-harm of approximately 250 over the trial durations.
The mechanism is twofold. First, rapid weight loss from any cause (diet, surgery, drug) increases gallstone formation by mobilizing cholesterol from adipose tissue, supersaturating bile, and slowing gallbladder emptying. Second, GLP-1 receptors are expressed on the gallbladder itself, and pharmacological GLP-1 stimulation reduces gallbladder contractility independently of weight loss.
Practical posture: counsel patients about the symptom pattern of biliary colic (post-prandial right upper quadrant pain, especially after fatty meals), and obtain ultrasound for any persistent or recurrent RUQ pain. Ursodiol prophylaxis is sometimes used in patients undergoing very rapid weight loss but is not standard for routine GLP-1 RA use.
NAION (Anterior Ischemic Optic Neuropathy)
Hathaway et al. (JAMA Ophthalmology 2024) published a retrospective cohort study of 16,827 patients from a Massachusetts hospital system showing that semaglutide users had a roughly 4-fold higher incidence of non-arteritic anterior ischemic optic neuropathy (NAION) compared to non-users with similar baseline characteristics. NAION is a sudden, usually painless, monocular vision loss caused by ischemia of the optic nerve head, and is the second most common cause of optic neuropathy in adults after glaucoma.
The signal is preliminary and the absolute incidence remains low (estimated 2–9 per 100,000 person-years in the general population, perhaps quadrupled in semaglutide users), but it has prompted formal regulatory review. A potential mechanism is rapid reduction in nocturnal blood pressure or in serum glucose, both of which can compromise optic nerve perfusion in the susceptible "disc-at-risk" anatomy (small cup-to-disc ratio). Patients who have already had NAION in one eye are at very high risk of contralateral involvement and should probably avoid GLP-1 RA exposure.
Practical posture: ask about prior NAION before prescribing; for any patient who develops sudden monocular vision change, refer for urgent ophthalmologic evaluation and consider holding therapy pending diagnosis. Routine ophthalmology surveillance is not currently recommended.
Lean-Mass Loss
As discussed on Weight Loss Studies, approximately 25–40% of the total weight lost on a GLP-1 RA is lean (non-fat) mass — muscle, organ, and water. For a 30 kg total loss, this is 8–12 kg of lean mass, including a substantial fraction of skeletal muscle. This is not unique to GLP-1 agonists (any large weight loss does this), but the magnitude of the total loss makes the absolute lean loss large in elderly patients and increases sarcopenia risk.
The countermeasures are well-established but require active intervention:
- Resistance training — the single best-validated intervention. Two to three sessions per week with progressive overload across the major muscle groups (squat / hinge / push / pull pattern). A trainer or formal program is justified for most patients.
- Protein intake — the standard 0.8 g/kg RDA is inadequate during active weight loss. Target 1.2–1.6 g/kg/day, weighted toward 30–40 g per meal across 3–4 meals. Whey or casein protein supplementation is reasonable if dietary intake is constrained by reduced appetite.
- Vitamin D and creatine — both support muscle protein synthesis and are inexpensive adjuncts.
- Periodic body composition assessment — DEXA or bioimpedance to track fat-mass loss vs lean-mass loss; if lean mass is declining excessively, dose reduction may be appropriate.
Suicidal Ideation Signal (Disputed)
In mid-2023, the European Medicines Agency announced an investigation into reports of suicidal ideation and self-harm among patients on GLP-1 receptor agonists, prompted by 150 spontaneous reports from Iceland. Subsequent large pharmacovigilance studies have not consistently confirmed an elevated risk — a 2024 analysis of 1.6 million patients (Wang et al., Nat Med 2024) found no increased risk of suicidal ideation and a numerically lower risk than comparator weight-loss treatments. The EMA concluded in mid-2024 that available evidence does not support a causal link, while continuing surveillance.
The clinical posture is to ask about mood symptoms, depression history, and any suicidal ideation at baseline and at each follow-up while a patient is on therapy, particularly during the early titration phase. Patients with active major depressive disorder or recent suicidal ideation merit closer monitoring; the medication does not need to be avoided, but the threshold to refer to mental health support should be low.
Pregnancy, Lactation, and Renal Considerations
GLP-1 receptor agonists are not recommended in pregnancy. Animal teratogenicity data are limited but include skeletal and visceral malformations at high doses. The medication should be discontinued at least 2 months before a planned pregnancy (to allow drug washout for the long-acting agents) and avoided during breastfeeding. Patients of reproductive age should use reliable contraception. The medication can paradoxically restore ovulatory cycles in women with PCOS, increasing unintended-pregnancy risk for those who had assumed they were infertile.
Renal considerations: severe vomiting and diarrhea from titration can produce dehydration and acute kidney injury, particularly in patients also on ACE-inhibitors, ARBs, NSAIDs, or diuretics. Patients should be counseled to hold the medication and seek medical attention for severe persistent GI symptoms. The medication itself is not nephrotoxic, and FLOW trial data demonstrate a renal-protective effect — the harm is from volume depletion, not direct toxicity.
Discontinuation and Rebound
STEP-4 (Rubino, JAMA 2021) and SURMOUNT-4 (Aronne, JAMA 2024) both demonstrated that discontinuation of GLP-1 receptor agonist therapy is followed by regain of approximately two thirds of lost weight over 12 months. The biological mechanism is unavoidable — the central appetite suppression and delayed gastric emptying that drove the weight loss reverse when receptor stimulation ends. This is the same defended-weight-set-point biology that defeats nearly all dieting; the drug overrides it while present but does not reset the set-point.
The implication: GLP-1 receptor agonist therapy for obesity is an indefinite treatment, comparable in framing to statin therapy for dyslipidemia or antihypertensive therapy for hypertension. Patients should be counseled at the outset that the medication will most likely be continued long-term. Insurance coverage gaps, cost, supply shortages, and adverse-event-driven discontinuation all create real-world reasons for stopping; each carries a high probability of regain.
The active research questions concern strategies to make discontinuation less catastrophic — gradual taper rather than abrupt stop, combination with intensive behavioral therapy during taper, transition to lower-dose maintenance, or transition to alternative agents. None of these is yet supported by strong trial data.
Key Research Papers
- Bjerre Knudsen L et al., GLP-1 RA rodent thyroid C-cell tumors (Endocrinology 2010) — Search PubMed
- Bezin J et al., GLP-1 RAs and thyroid cancer (Diabetes Care 2023) — Search PubMed
- Singh S et al., incretin therapy and acute pancreatitis (JAMA Intern Med 2013) — PubMed: Singh 2013
- Sodhi M et al., GLP-1 RAs and adverse GI events for weight loss (JAMA 2023) — PubMed: Sodhi JAMA 2023
- Sherwin M et al., GLP-1 RAs and residual gastric content (Anesthesiology 2023) — Search PubMed
- Hathaway JT et al., semaglutide and NAION (JAMA Ophthalmol 2024) — PubMed: Hathaway 2024
- Faillie JL et al., GLP-1 RAs and gallbladder disease meta-analysis (JAMA Intern Med 2022) — PubMed: Faillie 2022
- McGowan BM et al., body composition with semaglutide (Diabetes Obes Metab 2024) — Search PubMed
- Rubino D et al., STEP-4 withdrawal trial (JAMA 2021) — Search PubMed
- Aronne LJ et al., SURMOUNT-4 withdrawal trial (JAMA 2024) — PubMed: Aronne 2024
- Wang W et al., semaglutide and suicidal ideation (Nat Med 2024) — Search PubMed
- ASA guidance on GLP-1 RA and elective surgery 2023 — Search PubMed
Connections
- Hunger, Leptin & Why Diets Fight Back — interactive animation
- GLP-1 Benefits Hub
- Mechanism & Insulin Response
- Weight Loss Studies
- Natural GLP-1 Boosting Foods
- GLP-1 Receptor Agonists (Hub)
- Type 2 Diabetes
- Obesity
- Gastroparesis
- Pancreatitis
- MEN-2 Syndrome
- Medullary Thyroid Carcinoma
- NAION
- Gallstones