GLP-1 Receptor Agonists — Natural GLP-1 Boosting Foods
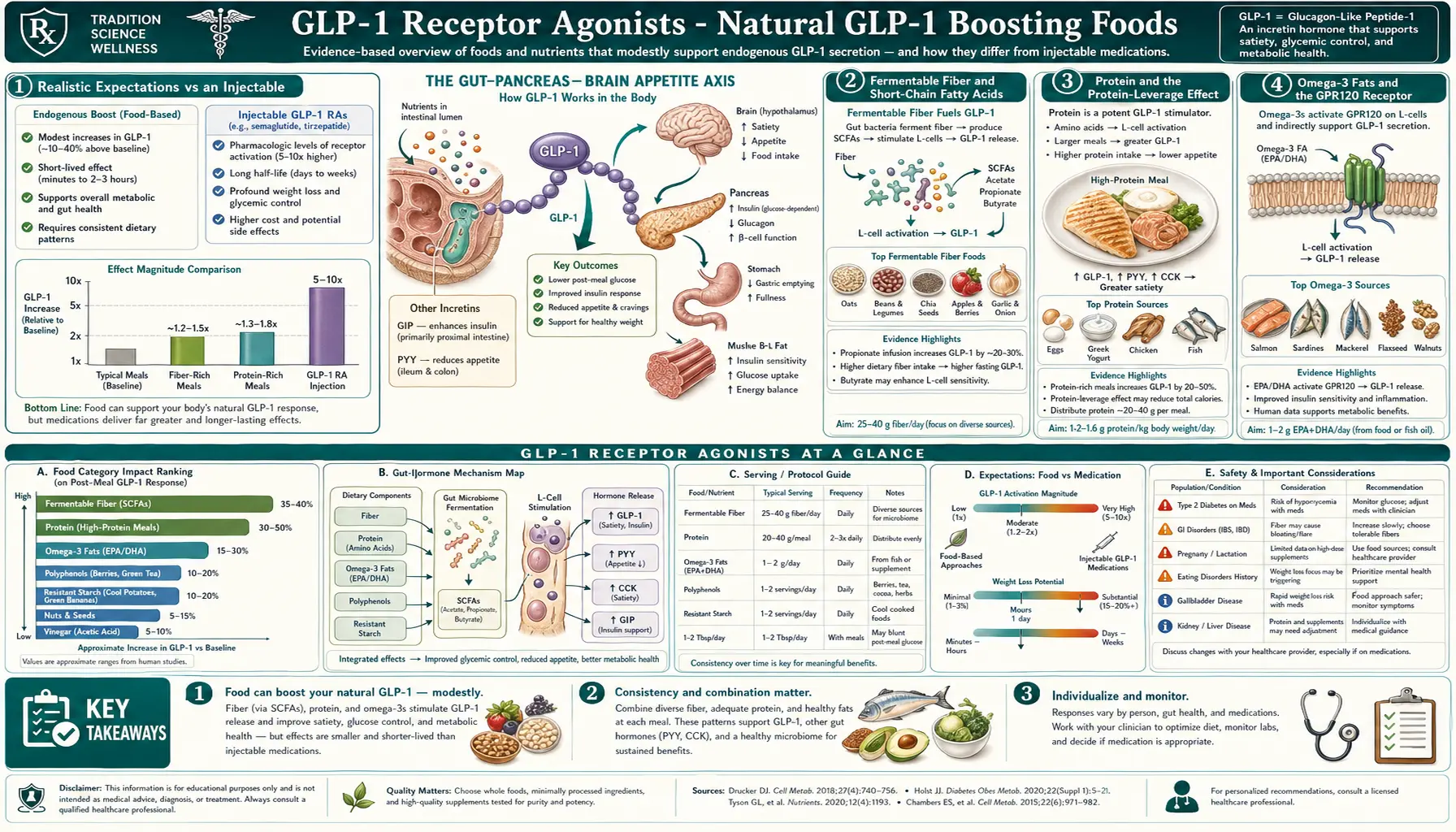
The native L-cells that secrete glucagon-like peptide 1 respond to specific dietary inputs — fermentable fiber via the short-chain-fatty-acid pathway, protein via direct amino acid sensing, omega-3 fats via the GPR120 receptor, bitter compounds via T2R bitter-taste receptors, bile acids via the TGR5 receptor, and certain polyphenols via multiple mechanisms. A food strategy that maximizes these stimuli typically produces post-prandial GLP-1 elevations of 2–4 fold above baseline (vs the 5–10 fold achieved by injectable agonists), translating to 2–5% body-weight reduction over months in trials of high-fiber, high-protein diets. This is much less than an injectable produces, but it is sustainable, safe, and synergistic with pharmacotherapy. This page covers the food categories with the strongest evidence, how to combine them in a daily eating pattern, and where the evidence is preliminary.
Interactive Visualization Hunger, Leptin & Why Diets Fight Back Watch the hunger neurons and the fullness neurons fight it out — then lose weight and see leptin fall, hunger climb and metabolism drop. It isn’t willpower. It’s a defended system. Launch →
Table of Contents
- Realistic Expectations vs an Injectable
- Fermentable Fiber and Short-Chain Fatty Acids
- Protein and the Protein-Leverage Effect
- Omega-3 Fats and the GPR120 Receptor
- Bitter Compounds and the TGR5 Bile Acid Receptor
- Polyphenols, Berberine, and Fermented Foods
- Meal Sequencing and Food Order
- A Sample High-GLP-1 Day of Eating
- Combining With Pharmacotherapy
- Key Research Papers
- Connections
- Featured Videos
Realistic Expectations vs an Injectable
Native post-prandial GLP-1 secretion in healthy adults peaks at about 20–40 pmol/L within 15–30 minutes of a meal and returns to baseline within 2–3 hours. A protein-rich, fiber-rich meal can roughly double this peak and modestly prolong the elevation, reaching ~40–80 pmol/L. By comparison, injectable semaglutide produces continuous plasma concentrations equivalent to ~150–200 pmol/L of GLP-1 receptor activation throughout the dosing week. The injectable is therefore an order of magnitude more powerful than even an optimally engineered diet.
The corresponding weight-loss expectations: dietary strategies that consistently elevate endogenous GLP-1 (high-fiber, high-protein, with bitter compounds and omega-3) produce 2–5% body-weight reduction over 6–12 months in trials, vs 15–22% for the injectable agonists. This is not nothing — 3% body-weight loss reduces progression to type 2 diabetes by ~30% in the Diabetes Prevention Program data — but the food approach should not be framed as a replacement for a $1,000-per-month injectable in patients with class-3 obesity. It is a complementary strategy that may suffice for some patients, that supports the effect of an injectable in others, and that maintains some of the metabolic benefit when an injectable is discontinued.
Fermentable Fiber and Short-Chain Fatty Acids
The most robust food-based GLP-1 stimulus is fermentable fiber. Soluble, fermentable fibers (inulin, oligofructose, beta-glucan, resistant starch, pectin) reach the colon undigested, where bacterial fermentation produces short-chain fatty acids (SCFAs): butyrate, propionate, and acetate. SCFAs activate the free fatty acid receptor 2 (FFAR2, also called GPR43) on L-cells, triggering GLP-1 secretion. The pathway was characterized in detail by Tolhurst et al. (Diabetes 2012). Patrice Cani's 2009 Diabetes paper documented that oligofructose supplementation increased post-prandial GLP-1 by ~30% in humans and reduced food intake.
High-impact fermentable fiber sources:
- Beta-glucan — oats and barley. A bowl of steel-cut oats provides 4–6 g beta-glucan. Repeatedly shown to elevate post-prandial GLP-1 and reduce subsequent meal intake.
- Inulin — chicory root (the highest natural source), Jerusalem artichokes, onions, garlic, leeks, asparagus, banana (especially green). Supplementation studies typically use 8–15 g/day, which is at the upper end of GI tolerance for most people.
- Resistant starch — cooked-and-cooled potatoes, cooked-and-cooled rice, green bananas, raw potato starch, legumes. Cooling cooked starches converts a portion to crystalline resistant starch that resists small-intestinal digestion.
- Pectin — apples, citrus peel, berries.
- Psyllium — husk or whole. Less fermented than inulin but partially so; primary action is bulk and viscosity, which also modestly extend GLP-1 signaling.
- Legumes — lentils, chickpeas, black beans, white beans. A heterogeneous mix of resistant starch, soluble fiber, and oligosaccharides; consistently associated with metabolic benefit.
Target intake: a typical American diet provides 10–15 g/day total fiber. Targeting 30–40 g/day with at least 10–15 g from fermentable sources requires daily attention. Build up gradually over 3–4 weeks to allow the gut microbiome to adapt and minimize bloating.
Protein and the Protein-Leverage Effect
Protein is the most satiating macronutrient on a per-calorie basis. The mechanism is multi-channel: direct amino acid sensing by L-cells via several G-protein-coupled receptors (CaSR, GPR142, T1R1/T1R3 umami receptors), elevated post-prandial peptide YY (PYY) and cholecystokinin (CCK) in parallel with GLP-1, and the hypothesis-driven "protein leverage" behavior in which animals (including humans) preferentially eat to a target protein intake and overeat carbohydrate/fat when protein density is low.
Karra et al. (Diabetologia 2009) and many subsequent studies have documented that a meal with 30–40 g of protein produces a substantially higher post-prandial GLP-1 elevation than an isocaloric meal with 10–15 g protein. Whey protein produces the largest acute response (rapid amino acid absorption peak), casein produces a more sustained response, and animal-vs-plant protein differences are modest at equivalent leucine content.
Practical targets:
- Total daily protein: 1.2–1.6 g/kg body weight, distributed across 3–4 meals.
- Per-meal target: 30–40 g protein, the threshold at which leucine reliably triggers muscle protein synthesis and GLP-1 secretion in non-elderly adults; up to 50 g for elderly patients to overcome anabolic resistance.
- Best per-calorie protein density: egg whites, whey isolate, cod, white fish, chicken breast, lean beef sirloin, Greek yogurt, cottage cheese, tofu, edamame, tempeh.
- Whey or casein supplementation: 25–30 g of whey isolate at breakfast is a low-friction way to ensure protein-target meals without cooking; particularly useful for patients on appetite-suppressing GLP-1 agonists who otherwise struggle to consume enough protein.
Omega-3 Fats and the GPR120 Receptor
Long-chain fatty acids stimulate L-cell GLP-1 secretion via the GPR120 receptor (also called FFAR4). The receptor was characterized by Hirasawa et al. (Nat Med 2005); it has higher affinity for omega-3 fatty acids (EPA, DHA, alpha-linolenic acid) than for saturated or monounsaturated fats. GPR120 activation also has independent anti-inflammatory effects in macrophages, which may contribute to the metabolic benefits of omega-3 intake beyond GLP-1 stimulation.
High-impact omega-3 food sources:
- Salmon — 1.5–2.5 g EPA+DHA per 100 g serving. Wild Alaskan or Atlantic farmed both effective.
- Sardines — 1.0–2.0 g EPA+DHA per 100 g; small-fish low-mercury choice with calcium and vitamin D.
- Herring — 1.7–2.0 g EPA+DHA per 100 g.
- Mackerel — 2.5–5 g per 100 g (highest of any commonly eaten fish).
- Anchovies — 1.5 g EPA+DHA per 100 g.
- Walnuts, flaxseed, chia — alpha-linolenic acid (ALA) which is converted to EPA at low efficiency (5–10%) in humans; useful but not equivalent to direct EPA/DHA from fish.
Target: two to three servings of oily fish per week, or 1–2 g/day of EPA+DHA from supplementation. Thomsen et al. (Am J Clin Nutr 1999) showed that olive-oil-rich meals also elevate post-prandial GLP-1 (via different long-chain monounsaturated fat signaling), supporting the broader Mediterranean dietary pattern as a GLP-1-friendly approach.
Bitter Compounds and the TGR5 Bile Acid Receptor
L-cells express bitter taste receptors (T2R family) — the same receptors that detect bitterness on the tongue — on the luminal membrane. Iwasaki et al. (Cell Metab 2018) and subsequent work have established that ingestion of bitter compounds drives a measurable GLP-1 release independent of caloric intake, an evolutionary defense response against potentially toxic plant alkaloids that became repurposed for metabolic regulation.
L-cells also express the TGR5 receptor (Thomas et al., Cell Metab 2009), a G-protein-coupled receptor activated by bile acids. Bile acid-rich meals (which trigger gallbladder contraction and deliver bile acids to the intestine) provide an indirect TGR5-mediated GLP-1 stimulus. Berberine, a botanical alkaloid, is a TGR5 agonist and a documented GLP-1 secretagogue (Yu et al., Phytomedicine 2018).
Practical bitter / TGR5-active foods:
- Coffee — chlorogenic acid and roast-derived bitter compounds. Acute and chronic coffee consumption is associated with reduced type 2 diabetes risk in multiple cohorts.
- Bitter greens — arugula, radicchio, endive, dandelion greens, watercress, mustard greens.
- Cruciferous vegetables — kale, broccoli rabe, Brussels sprouts.
- Hops (in beer) and gentian (in digestive aperitifs / bitters)
- Berberine 500 mg twice daily — documented to elevate post-prandial GLP-1 and improve glycemic control; the most evidence-supported botanical GLP-1 secretagogue.
- Bile-acid-rich meals — eggs and meats rich in cholesterol drive larger gallbladder contractions and thus larger TGR5 signal.
- Apple cider vinegar — some evidence of post-prandial glucose and GLP-1 effect, mechanism less clear; 1–2 tbsp with meals is the typical dose.
Polyphenols, Berberine, and Fermented Foods
Multiple polyphenols have documented effects on GLP-1 secretion and DPP-4 inhibition in cell and animal studies, with modest supporting human evidence: EGCG from green tea (DPP-4 inhibition), curcumin from turmeric (multi-mechanism), resveratrol from grapes and red wine (SIRT1 activation with downstream GLP-1 effect), anthocyanins from berries, and quercetin from onions and capers. These add small effects and the broad pattern (a colorful, polyphenol-rich whole-food diet) is more important than any single compound.
Fermented foods may contribute via several pathways: live bacterial cultures that modulate the gut microbiome to favor SCFA-producing taxa, intrinsic SCFA content in mature ferments, and bioactive peptides produced during fermentation. Yogurt (especially Greek yogurt for the protein bonus), kefir, sauerkraut, kimchi, miso, tempeh, and natto are all reasonable inclusions in a daily diet. Trial evidence for a direct GLP-1 effect of fermented foods is preliminary but the broader metabolic-health evidence is supportive.
Meal Sequencing and Food Order
Eating vegetables and protein before carbohydrate within a meal produces lower post-prandial glucose, higher post-prandial GLP-1, and modestly increased satiety. Shukla et al. (Diabetes Care 2015) documented that the same total meal eaten in the order (1) vegetables & protein, then (2) carbohydrates 10 minutes later, produced ~30% lower glucose AUC and significantly higher GLP-1 elevation than the reverse order in patients with type 2 diabetes.
Practical application: at restaurants, eat the salad first, the protein second, the bread / rice / potato last. At home, fill half the plate with non-starchy vegetables and eat them first. The intervention requires no change in what is eaten, only the order — one of the lowest-friction metabolic interventions documented.
Other practical eating-pattern tweaks with supporting evidence: a 12–14 hour overnight fast (time-restricted eating with the eating window between roughly 8 AM and 6–8 PM), a longer post-prandial walk (10–15 minutes after each meal blunts the glucose excursion and supports gastric emptying within tolerable limits), and avoiding sugar-sweetened beverages (which deliver carbohydrate without protein, fiber, or fat to slow absorption).
A Sample High-GLP-1 Day of Eating
An illustrative daily pattern that maximizes GLP-1 stimulation across all the mechanisms above:
- Breakfast (8 AM) — Greek yogurt (35 g protein) with mixed berries (anthocyanins, pectin), ground flaxseed (omega-3 ALA, fiber), and 25 g of cooked-and-cooled steel-cut oats (resistant starch + beta-glucan). Coffee (bitter compounds, chlorogenic acid).
- Lunch (12–1 PM) — large mixed-greens salad with bitter greens (arugula, radicchio), 6 oz of canned wild salmon (omega-3 + protein), olive oil and apple-cider-vinegar dressing, a side of cooked-and-cooled lentils (resistant starch + fermentable fiber). Eat the salad and salmon first; eat the lentils last.
- Snack (3 PM) — whey protein shake (25 g whey isolate) blended with 1 tbsp chia seeds and water.
- Dinner (6–7 PM) — broiled cod or sardines, steamed broccoli rabe, roasted Brussels sprouts, a small portion of cooked-and-cooled wild rice. Eat the vegetables and fish first.
- Optional — berberine 500 mg with breakfast and dinner (with calorie-containing meals; on empty stomach causes GI upset).
- Overnight fast — finish dinner by 7–8 PM, begin breakfast at 8 AM for a 12–13 hour fast.
Total: roughly 130–150 g protein, 40–50 g fiber (15–20 g fermentable), 2–3 g EPA+DHA, bitter compounds at multiple meals, polyphenols throughout. This level of food-based optimization is sufficient for substantial metabolic improvement in many patients without diabetes, and is a reasonable foundation for those also using an injectable.
Combining With Pharmacotherapy
For patients on an injectable GLP-1 receptor agonist, the food strategies above are synergistic, not redundant. Three reasons to maintain them even while on injectable therapy:
- Side-effect mitigation. A high-protein, lower-fat eating pattern reduces the nausea and gastric-emptying delay that drive titration intolerance. Smaller, more frequent meals are also better tolerated.
- Lean-mass preservation. The 1.2–1.6 g/kg/day protein target combined with resistance training is the documented strategy to minimize the 25–40% lean-mass loss that otherwise accompanies large total-weight loss.
- Post-discontinuation cushion. Patients who learn the food-based GLP-1 strategy while on the injectable have it available as a partial maintenance approach when the injectable is stopped or interrupted. It will not fully prevent regain, but it can blunt it.
For patients not on an injectable, the food strategy is the primary GLP-1-targeted intervention. Realistic expectations are 2–5% body-weight reduction over 6–12 months with strict adherence, accompanied by meaningful improvements in HbA1c, post-prandial glucose, fasting insulin, blood pressure, and lipid profile.
Key Research Papers
- Tolhurst G et al., SCFAs stimulate GLP-1 via FFAR2 (Diabetes 2012) — Search PubMed
- Cani PD et al., oligofructose and endogenous GLP-1 (Diabetes 2009) — Search PubMed
- Karra E et al., whey protein and post-prandial GLP-1 (Diabetologia 2009) — Search PubMed
- Thomsen C et al., dietary fat type and GLP-1 (Am J Clin Nutr 1999) — Search PubMed
- Iwasaki Y et al., bitter taste receptors and GLP-1 (Cell Metab 2018) — Search PubMed
- Thomas C et al., TGR5 bile acid receptor (Cell Metab 2009) — PubMed: Thomas 2009
- Yu Y et al., berberine and GLP-1 (Phytomedicine 2018) — Search PubMed
- Hirasawa A et al., GPR120 omega-3 receptor (Nat Med 2005) — Search PubMed
- Shukla AP et al., food order and post-prandial glucose (Diabetes Care 2015) — PubMed: Shukla 2015
- Reimer RA et al., dietary fiber and L-cell GLP-1 (Endocrinology 2017) — Search PubMed
- Belza A et al., whey isolate suppresses food intake via GLP-1 (Am J Clin Nutr 2013) — Search PubMed
- Bodnaruc AM et al., nutritional modulation of GLP-1 secretion review (Nutr Metab 2016) — Search PubMed
Connections
- Hunger, Leptin & Why Diets Fight Back — interactive animation
- GLP-1 Benefits Hub
- Mechanism & Insulin Response
- Weight Loss Studies
- Side Effects & Cautions
- GLP-1 Receptor Agonists (Hub)
- Berberine
- Intermittent Fasting
- Salmon
- Sardines
- Eggs
- Lentils
- Yogurt (Greek)
- Bone Broth
- Turmeric (Curcumin)
- Type 2 Diabetes
- Insulin Resistance