Gerson Therapy — Coffee Enema Component
The coffee enema is the most controversial and frequently misunderstood element of the Gerson Therapy. The Gerson protocol prescribes up to five coffee enemas per day — each composed of approximately 1 liter of filtered water plus 3 tablespoons of organically grown, lightly roasted, drip-grind coffee, simmered for 12 minutes and cooled to body temperature. The claimed mechanism is hepatic Phase II enzyme induction, primarily via caffeine and the kahweol/cafestol palmitates upregulating glutathione-S-transferase activity in the liver, with simultaneous bile flow stimulation. The mainstream medical position is uniformly negative: the American Cancer Society, National Cancer Institute, and most gastroenterology societies explicitly recommend against the practice. This page presents the mechanistic case, the published primary literature, the documented harms, and the historical Kellogg-era origins — allowing readers to weigh the evidence themselves.
Table of Contents
- Historical Origins — Kellogg, Gerson, and the Merck Manual
- The Mechanistic Claim — Wattenberg and Phase II Induction
- Bile Flow, Cholecystokinin, and the Hepatic-Portal Route
- Protocol Specifics — Frequency, Preparation, Technique
- Documented Harms — Deaths, Burns, and Electrolyte Disturbance
- Mainstream Position — ACS, NCI, and Gastroenterology Society Statements
- The Integrative Practitioner View
- Patient Considerations — If You Are Going to Do This
- Key Research Papers
- Connections
- Featured Videos
Historical Origins — Kellogg, Gerson, and the Merck Manual
The coffee enema predates Max Gerson by several decades. Therapeutic enemas of various kinds — saline, soap-suds, herbal — were standard medical practice in the late 19th and early 20th centuries, with coffee enemas appearing in mainstream medical reference works including early editions of the Merck Manual (continuing into the 12th edition, 1972). Dr. John Harvey Kellogg at the Battle Creek Sanitarium used coffee enemas extensively in the 1890s and early 1900s as part of his hydrotherapy and bowel-management protocols.
Max Gerson's own use of coffee enemas began during World War I battlefield medicine. As an army doctor on the German side, Gerson observed that soldiers undergoing surgical procedures with limited morphine were calmed and reported pain relief when given retained coffee enemas. The mechanism Gerson hypothesized at the time was vasodilation of the hepatic portal system, increased bile excretion, and reduced systemic toxic load from surgical tissue trauma. He carried this technique into his interwar practice in Germany, then to the United States after fleeing the Nazi regime in 1936.
By the time Gerson published A Cancer Therapy: Results of Fifty Cases in 1958, coffee enemas had become the central detoxification component of his protocol. His argument was that the high-juice diet liberated stored toxins from fat and lymphatic tissue at a rate the unaided liver could not process, and that coffee enemas accelerated hepatic Phase II conjugation enough to keep up with the liberated load.
Coffee enemas remained in the Merck Manual's standard nursing and medical reference sections through the 12th edition (1972) but were removed thereafter as part of a broader removal of pre-pharmacological-era practices from mainstream reference works. Gerson's clinics, the integrative oncology community, and certain naturopathic traditions retained the practice.
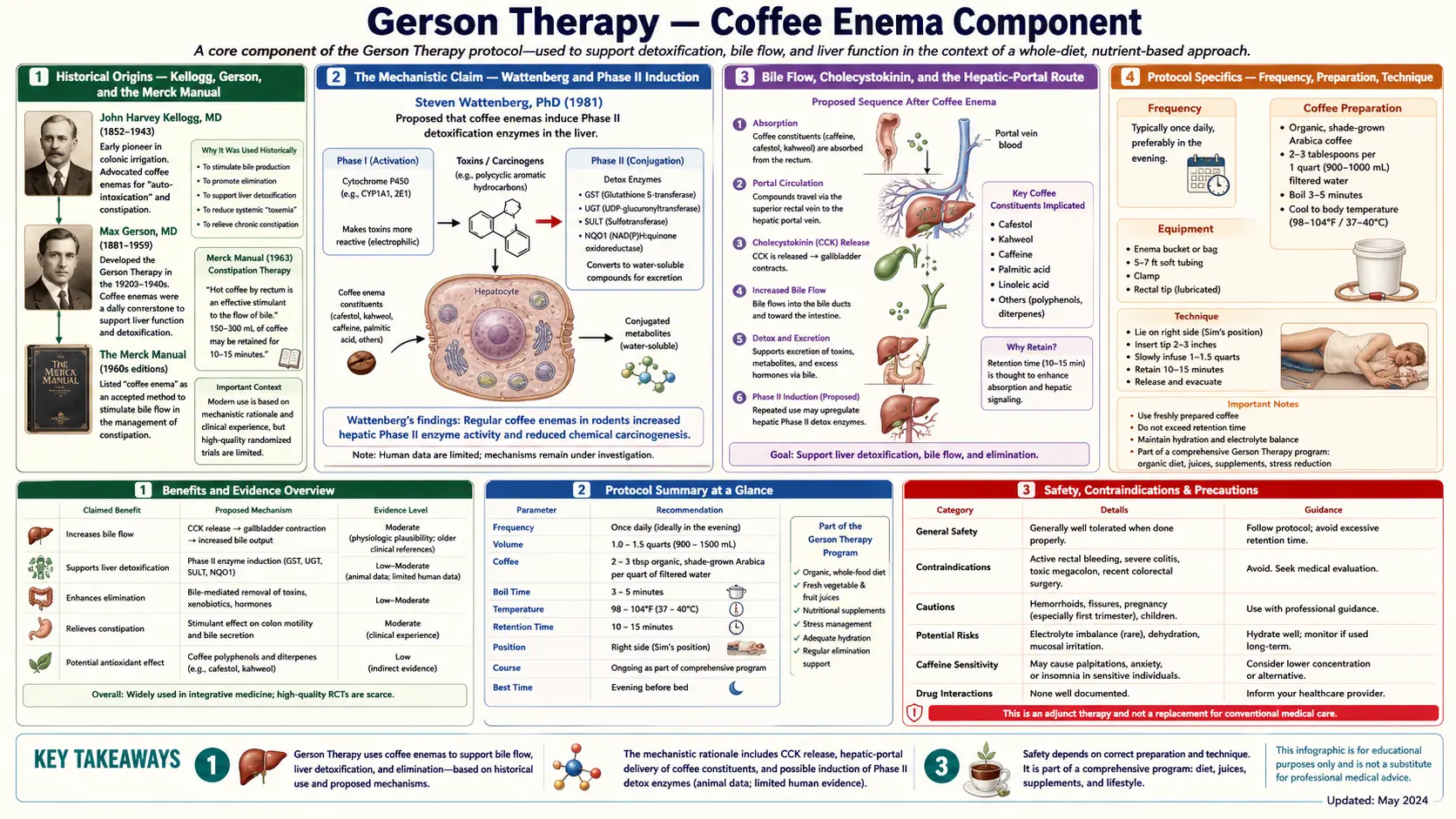
The Mechanistic Claim — Wattenberg and Phase II Induction
The mechanistic case Gerson proponents advance rests largely on the laboratory work of Lee Wattenberg at the University of Minnesota in the 1970s and 1980s. Wattenberg studied dietary modulators of hepatic xenobiotic metabolism and identified several coffee constituents — including the diterpene palmitates cafestol and kahweol — as inducers of glutathione-S-transferase (GST), the Phase II conjugation enzyme that conjugates glutathione to electrophilic xenobiotics and reactive metabolites of Phase I oxidation.
The proponent argument extrapolates from Wattenberg's data as follows:
- GST is the rate-limiting enzyme for conjugation of many environmental toxins and the reactive intermediates of Phase I CYP450 metabolism.
- Cafestol and kahweol are documented GST inducers in rodent liver studies.
- Coffee delivered rectally enters portal circulation directly via the hemorrhoidal-vein anastomosis, bypassing first-pass dilution in the systemic circulation, and reaches the liver at higher local concentration than oral coffee would.
- Therefore rectal coffee should induce hepatic GST more efficiently than oral coffee, accelerating clearance of stored and circulating toxins.
This chain has several legitimate weak links that the mainstream critique highlights:
- Wattenberg studied dietary (oral) coffee and isolated cafestol/kahweol. He did not study rectal administration, and no rigorous head-to-head comparison of oral vs rectal coffee for hepatic enzyme induction has been published.
- The hemorrhoidal-portal anastomosis is real but inconsistently developed; in most patients the dominant venous drainage of the lower rectum is systemic (via inferior hemorrhoidal veins to the inferior vena cava), not portal.
- Caffeine itself is a poor GST inducer; the active compounds appear to be the lipid-soluble diterpene palmitates, whose absorption from a coffee enema with very limited retention time has not been quantified.
- Even if hepatic GST induction does occur, the clinical relevance — whether faster Phase II conjugation translates into meaningful detoxification of any specific named toxin in any specific named disease — has not been established by any controlled trial.
The honest summary is that the mechanism is plausible at the molecular level, has not been demonstrated in vivo for the rectal route, and even if demonstrated would not by itself establish clinical benefit.
Bile Flow, Cholecystokinin, and the Hepatic-Portal Route
A separate proponent argument is that coffee enemas stimulate bile flow through cholecystokinin (CCK) release and direct dilation of the bile ducts, allowing more rapid hepatobiliary excretion of conjugated metabolites. The CCK release argument has some mainstream support — oral coffee is a documented CCK secretagogue, and CCK does trigger gallbladder contraction and bile expulsion.
The extrapolation to rectal coffee is again less well-established. Theophylline and theobromine (caffeine's metabolic relatives) do relax sphincter muscles including the sphincter of Oddi, which controls bile and pancreatic-juice flow into the duodenum. Whether this effect occurs at clinically meaningful magnitude from rectally administered coffee is unclear.
The subjective reports from Gerson Therapy patients are consistent and worth noting even if not mechanistically conclusive. Patients describe a sense of decreased nausea, decreased pain (particularly in cancer patients), and a "lightened" feeling after coffee enemas. These reports could reflect: (a) genuine hepatic detoxification benefit, (b) the caffeine's direct analgesic effect (caffeine is a well-known opioid analgesic adjunct), (c) cholinergic vagal stimulation from rectal volume distension, (d) classical pharmacological placebo, or some combination of all four. Distinguishing these in a controlled trial would be straightforward in principle and has not been done.
Protocol Specifics — Frequency, Preparation, Technique
The standard Gerson coffee enema preparation, as published by the Gerson Institute:
- Coffee: 3 tablespoons organically grown, lightly roasted, drip-grind (not espresso, not instant). The light roast is specified because cafestol and kahweol degrade with heavier roasting.
- Water: 1 liter (32 ounces) of filtered or distilled water.
- Preparation: Bring water to boil, add coffee, boil 3 minutes, simmer 12 minutes, strain through cheesecloth or fine mesh, cool to body temperature (~37 °C). Discard if the liquid is too hot or too cold.
- Administration: Lying on the right side, knees drawn up. Insert lubricated catheter 4–6 inches into rectum. Open clamp on enema bag (suspended ~18 inches above body to provide gentle gravity pressure). Allow full liter to enter slowly (4–5 minutes).
- Retention: Target 12–15 minutes of retention before evacuation. Stay on right side initially to encourage left-to-right colonic distribution.
- Frequency: Up to 5 per day during active treatment of advanced disease; 1–2 per day during maintenance.
The right-side positioning is specifically argued to encourage absorption through the hepatic flexure of the colon and into the portal circulation. The 12-15 minute retention target is chosen as the empirical compromise between insufficient absorption (less than 10 minutes) and rectal mucosal irritation (more than 20 minutes).
The Gerson Institute's patient training program at its Tijuana clinic includes hands-on demonstration and supervised practice of the technique. Self-taught patients without prior clinic training experience higher rates of technical complications (improper temperature, insufficient straining causing colonic irritation from coffee grounds, improper retention causing premature evacuation).
Documented Harms — Deaths, Burns, and Electrolyte Disturbance
The published harms case against coffee enemas is real and should be presented honestly. Documented case-series harms include:
- Electrolyte deaths: Several deaths have been published in case reports attributed to severe hyponatremia following excessive frequency of coffee enemas (more than 5 per day, sometimes more than 10 per day, in patients self-administering outside any clinic protocol). The mechanism is loss of sodium and other electrolytes in evacuated fluid combined with rapid water absorption from each enema.
- Septicemia: Case reports of gram-negative bacteremia from contaminated enema bags, insufficiently sterilized catheters, or contaminated coffee preparation. Patients on protocol-related immunosuppression are at higher risk.
- Proctocolitis: Inflammation of the rectum and distal colon from caffeine-induced mucosal irritation, particularly with very frequent administration. Usually self-limited on discontinuation but occasionally requires medical treatment.
- Rectal burns: From improperly cooled coffee enema fluid. The Gerson Institute's emphasis on testing temperature against the inner wrist before administration directly addresses this.
- Hemorrhoidal exacerbation: The repeated mechanical introduction of fluid worsens existing hemorrhoidal disease.
The American Cancer Society's position statement specifically cites these harms as the basis for its recommendation against the practice. The number of documented serious harms is small (single digits of published deaths, several dozen serious complications across decades of practice and tens of thousands of patient-years of exposure), but the harms are real, and patients deserve to know.
It is also fair to note that most published deaths and serious complications have occurred in patients self-administering at frequencies above the Gerson Institute's recommended maximum (5 per day) and without clinic-supervised technique training. The harms in clinic-supervised settings have been substantially lower. This does not change the fundamental safety equation but does point to where harm-reduction would have the most impact if the practice continues.
Mainstream Position — ACS, NCI, and Gastroenterology Society Statements
The mainstream medical position on coffee enemas is unambiguous:
- American Cancer Society: explicitly recommends against the use of coffee enemas. Cites the documented harms (deaths, infections, electrolyte disturbance) and the absence of evidence for the claimed mechanism in vivo.
- National Cancer Institute (PDQ summary): notes that no controlled clinical trial has demonstrated benefit from coffee enemas in cancer treatment; describes the mechanistic claims as unsubstantiated.
- American Gastroenterological Association: does not include coffee enemas in any treatment guideline. The broader category of "colon cleansing" practices is described as without evidence base.
- Cancer Research UK: states there is no scientific evidence that coffee enemas help treat cancer; lists the published harms.
- Memorial Sloan Kettering Integrative Medicine: lists the practice in its database as without supporting clinical evidence.
The mainstream position is, however, a position about the published clinical-evidence base, not necessarily a position about every mechanistic claim. The Wattenberg laboratory work on Phase II enzyme induction is mainstream science; what is disputed is the leap from that bench-level observation to therapeutic benefit in cancer or chronic disease. This distinction is sometimes lost in shorthand summaries on both sides.
The Integrative Practitioner View
A minority of integrative oncologists and naturopathic physicians continue to recommend coffee enemas, typically with several modifications from the strict Gerson protocol:
- Lower frequency (1–2 per day rather than 5)
- Mandatory electrolyte monitoring (serum sodium, potassium, chloride at baseline and every 2–4 weeks during use)
- Patient training on temperature testing and contamination prevention
- Exclusion of patients with active hemorrhoidal disease, diverticulitis, recent abdominal surgery, or severe immunosuppression
- Use as adjunct to conventional therapy (rather than replacement)
Practitioners taking this position cite the subjective patient-reported benefit (decreased nausea, decreased pain in cancer patients on opioid-sparing protocols), the plausibility of the Phase II induction mechanism even if not formally proven, and the historical safety record when properly supervised. They are also typically careful to distinguish their recommendation (coffee enemas as a supportive adjunct in selected patients) from the unmodified Gerson position (coffee enemas as a curative element of cancer treatment).
This more conservative integrative position is itself contested by mainstream medicine but is operationally distinct from the strict Gerson position. Patients evaluating practitioner recommendations should clarify which version of the practice is being recommended.
Patient Considerations — If You Are Going to Do This
If a patient and their physician have weighed the evidence and decided to include coffee enemas in a treatment plan despite the mainstream recommendation against, several risk-reduction practices substantially lower the harm risk:
- Baseline labs: serum sodium, potassium, chloride, BUN, creatinine, magnesium, and liver function before starting. Repeat every 2–4 weeks during use.
- Frequency limit: do not exceed the Gerson Institute's published maximum of 5 per day, and consider 1–2 per day adequate for most contexts.
- Sterile technique: dedicated enema bag (not shared), thoroughly cleaned after each use, replaced every 1–3 months. Filtered or distilled water only.
- Temperature testing: against the inner wrist; should feel neutral, neither warm nor cool.
- Absolute contraindications: active diverticulitis, recent colorectal surgery, severe hemorrhoidal disease, severe immunosuppression, rectal or anal cancer, inflammatory bowel disease in active flare.
- Stop immediately if: rectal bleeding, fever, severe abdominal pain, lightheadedness on standing (orthostatic indicator of electrolyte depletion), or persistent diarrhea.
- Do not substitute: for any conventional cancer treatment, surgery, or anti-cancer medication recommended by an oncologist.
Editorial position: this page is not a recommendation either for or against coffee enemas. It is an attempt to present the mechanistic case, the published clinical evidence, the documented harms, and the mainstream consensus accurately enough that readers can make their own informed decision in consultation with their own physicians. The page exists because the question is asked repeatedly and patients deserve a more complete answer than either "all natural therapies are safe" or "Gerson is quackery."
Key Research Papers
- Wattenberg LW, dietary coffee and Phase II enzyme induction — PubMed: Wattenberg coffee Phase II
- Cafestol and kahweol diterpene palmitates as GST inducers — PubMed: Cafestol kahweol GST
- Caffeine and cholecystokinin-mediated bile flow stimulation — PubMed: Caffeine bile flow
- Coffee enema-associated electrolyte deaths — case reports — PubMed: Coffee enema fatalities
- Coffee enema-associated proctocolitis and rectal injury — PubMed: Coffee enema proctocolitis
- Enema-related septicemia case series — PubMed: Enema septicemia
- American Cancer Society review of metabolic / detoxification therapies — PubMed: ACS metabolic therapy review
- Acosta & Cash, colonic irrigation safety review — PubMed: Acosta Cash colonic irrigation
- Hepatic Phase II enzyme biology and dietary modulation — PubMed: Hepatic Phase II
- NRF2 pathway and dietary inducers (sulforaphane, polyphenols, coffee compounds) — PubMed: NRF2 dietary inducers
- Caffeine analgesic adjunct effects and opioid-sparing — PubMed: Caffeine analgesic
- Hemorrhoidal-portal venous anastomosis anatomy — PubMed: Hemorrhoidal-portal anatomy
Connections
- Benefits Deep Dive Hub
- Juicing Protocol
- Mineral Density and Sodium-Potassium
- Documentary Evidence and Critique
- Gerson Therapy Main Hub
- Coffee Enemas Overview
- Coffee Enema Protocol
- Coffee
- Liver Cleansing
- Detox Protocols
- Coffee Enemas — the detox-protocol treatment of the same practice, covering the Phase II mechanism and safety framing outside the Gerson context.
- Gastroenterology
- Hepatology
- Magnesium
- Potassium
- Sodium