Zinc Deficiency: Skin Rashes and Acne
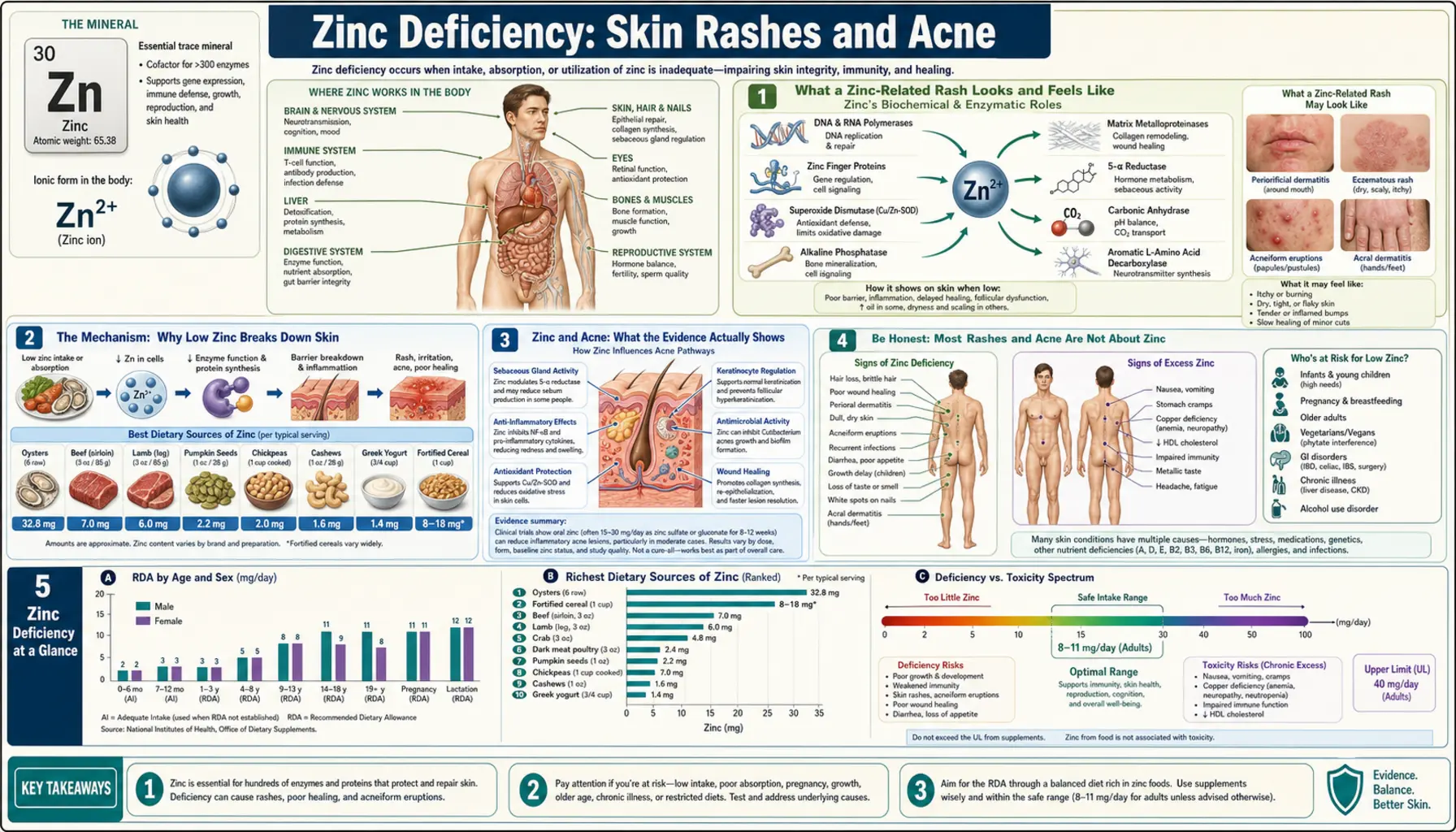
The skin is one of the first places low zinc shows up, because skin is a fast-renewing tissue that depends heavily on this mineral to build new cells and to calm inflammation. When zinc is genuinely deficient, the rash has a recognizable signature: scaly, red, sometimes crusted or weepy patches that cluster around the mouth and nose, around the eyes, around the genitals, and on the hands and feet — the body's openings and its extremities. Some people also notice that their acne is unusually inflamed or stubborn. This page explains what a zinc-related rash actually looks and feels like, the biology of why low zinc breaks down the skin, and — just as importantly — the honest truth that most rashes and most acne are not caused by zinc deficiency, so you can tell when zinc is genuinely worth investigating and when it is a red herring.
Table of Contents
- What a Zinc-Related Rash Looks and Feels Like
- The Mechanism: Why Low Zinc Breaks Down Skin
- Zinc and Acne: What the Evidence Actually Shows
- Be Honest: Most Rashes and Acne Are Not About Zinc
- Clues That Point Toward Zinc
- What Drives Zinc Low Enough to Affect Skin
- Getting Tested
- Correcting Low Zinc Safely
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What a Zinc-Related Rash Looks and Feels Like
The classic zinc-deficiency rash has a name — acrodermatitis, which literally means “skin inflammation of the extremities.” Its distribution is the single most useful clue, because it is so distinctive. The rash favors three zones:
- Around the body's openings (periorificial) — the skin around the mouth and nose, around the eyes, and around the genitals and anus. A red, scaly, sometimes cracked rim around the mouth that won't clear with ordinary moisturizer is a hallmark.
- The hands and feet (acral) — the backs of the hands, the fingers, the feet, and especially the skin around the nails. The skin can become red, thickened, scaly, or fissured.
- Friction and pressure areas — elbows, knees, and the diaper area in infants, where the skin is rubbed or moist.
Up close, the patches are typically well-defined, red to red-brown, dry and scaly, and may develop a glazed, crusted, or weepy (oozing) surface. In more severe cases small blisters or pustules form, and the patches can look almost “burned” or eroded. The rash is often described as resembling stubborn eczema or psoriasis — which is exactly why it is so frequently misdiagnosed at first.
Beyond the rash itself, a person with genuine zinc deficiency severe enough to inflame the skin usually has company symptoms, and those companions matter for distinguishing it from ordinary dermatitis. Commonly reported alongside the rash are hair thinning and wounds that are slow to heal, a blunted sense of taste or smell, mouth sores or inflamed corners of the mouth (angular cheilitis), brittle nails with white bands, diarrhea, irritability, and — in children — poor growth. The combination of a periorificial-and-extremity rash plus several of these systemic clues is far more suggestive of zinc than a rash alone.
The Mechanism: Why Low Zinc Breaks Down Skin
To understand why the skin is hit early and hard, it helps to know what zinc actually does in the body. Zinc is a structural and catalytic component of more than 300 enzymes and of a large family of “zinc-finger” proteins that switch genes on and off. In other words, zinc is not a fuel that gets burned — it is a tiny tool that countless biological machines need in order to work at all. The skin makes especially heavy use of those machines for two jobs: building new cells and controlling inflammation.
Building new cells. The outer layer of skin (the epidermis) is one of the most rapidly dividing tissues in the body — it completely replaces itself roughly every month. Cell division requires copying DNA, and the enzymes that copy and repair DNA (DNA and RNA polymerases) depend on zinc to hold their shape. When zinc runs short, the tissues that turn over fastest feel it first, because they have the least slack: skin, the lining of the gut, hair follicles, and immune cells. The skin cells that should be maturing in an orderly stack instead pile up abnormally and die early, which is why zinc-deficient skin becomes scaly, thickened in the wrong way, and prone to breaking down.
An analogy. Picture the epidermis as a bricklaying crew that must rebuild a wall every single month. Zinc is not the bricks and not the mortar — it is the trowels in the workers' hands. Take away enough trowels and the crew can still show up and still have materials, but the wall they lay is uneven, full of gaps, and crumbles at the edges. That crumbling, gap-ridden wall is exactly what a zinc-deficiency rash is: a skin barrier built by a crew that has lost its essential tools. Hand the trowels back — restore zinc — and the wall is rebuilt properly, often within a week or two.
Controlling inflammation and infection. Zinc also keeps the skin's immune response measured. It is required for the normal function of the immune cells that patrol the skin, and it helps restrain the release of inflammatory signaling molecules. When zinc is low, two things happen at once: the skin barrier leaks, letting in microbes and irritants, and the immune response to those intruders is poorly regulated — sometimes sluggish, sometimes over-reactive. The result is inflamed, easily infected, slow-to-settle skin. This same barrier-plus-immune role is why zinc deficiency also produces weakened immunity elsewhere in the body; the skin is simply the most visible front line.
One more biological detail explains why the rash sits where it does. The periorificial and acral zones — around the mouth, the hands, the feet — are areas of constant mechanical stress, moisture, and exposure, so they demand the highest rate of repair. Tissues with the highest turnover and the most wear are the first to fail when the repair toolkit is depleted, which is why a zinc rash announces itself at the mouth and fingertips rather than on the back or thigh.
Zinc and Acne: What the Evidence Actually Shows
Acne is a different story from the acrodermatitis rash, and it deserves an honest, carefully bounded explanation. Acne is driven by four overlapping problems in the oil glands and pores: excess oil (sebum), sticky shedding skin cells that plug the pore, overgrowth of the skin bacterium Cutibacterium acnes (formerly Propionibacterium acnes), and inflammation around all of it. Zinc plausibly touches three of those levers — it has mild anti-inflammatory and antibacterial activity and modestly influences oil production — which is the biological rationale for studying it in acne.
So what does the research show? Several lines of evidence are worth knowing, stated plainly:
- People with acne tend to have somewhat lower blood zinc. A systematic review and meta-analysis found that, on average, serum zinc levels were lower in people with acne than in those without, and that supplementing zinc could modestly improve acne. This is a real, repeatable association — but a modest average difference across groups is not the same as proof that low zinc caused any one person's acne.
- Oral zinc can reduce inflammatory acne, but it is weaker than antibiotics. In a multicenter randomized double-blind trial, zinc gluconate improved inflammatory acne — though the antibiotic minocycline worked better. That captures zinc's realistic role: a mild helper, not a front-line cure.
- Zinc is most useful for the red, inflamed (papular/pustular) type of acne, and less useful for blackheads and whiteheads (comedonal acne), which are more about pore plugging than inflammation.
The honest bottom line on acne: ordinary acne in a well-nourished person is not a zinc-deficiency disease. Most people with acne are not zinc deficient, and zinc is, at best, a modest adjunct to proven treatments — not a replacement for them. Zinc is most worth considering when acne is inflammatory and other measures have fallen short, or when acne appears alongside the systemic clues of true deficiency described above. We cover acne itself in depth on the Acne page, including the treatments with the strongest evidence.
Be Honest: Most Rashes and Acne Are Not About Zinc
This is the most important section on the page, because rashes are common and zinc deficiency severe enough to cause one is — in well-fed populations — relatively uncommon. A red, scaly, itchy patch is one of the least specific findings in all of medicine. Before reaching for zinc, it is worth remembering how many far more common conditions look similar:
- Eczema (atopic dermatitis) — itchy, dry, inflamed skin, often in the elbow and knee creases. By far the most common chronic rash, and frequently mistaken for a zinc rash early on.
- Contact and irritant dermatitis — a reaction to something the skin touched: nickel, fragrance, soaps, preservatives, plants. The rash maps to where the trigger landed.
- Seborrheic dermatitis — greasy, scaly redness around the nose, eyebrows, and scalp (dandruff is the mild form). Its location around the face can mimic the periorificial zinc pattern.
- Psoriasis — thick, silvery, well-demarcated plaques, classically on elbows, knees, and scalp.
- Rosacea and perioral dermatitis — facial redness and small bumps that are sometimes confused with both acne and a zinc rash.
- Fungal infections, scabies, drug reactions, and ordinary acne — all extremely common, none of them about zinc.
And acne, specifically, is so widespread that it affects most adolescents and a large share of adults — the overwhelming majority of whom have entirely normal zinc levels. Having a rash, or having acne, is not evidence of zinc deficiency. A zinc rash is suggested not by the rash in isolation but by its tell-tale distribution (around the mouth, eyes, genitals, hands, and feet), its resistance to standard skin treatments, and the company it keeps (hair loss, taste change, diarrhea, poor healing, poor growth in a child). Without those features, the smart money is on one of the common conditions above — and a dermatologist, not a zinc bottle, is the right next step. Self-diagnosing a rash as “low zinc” and self-treating with high-dose supplements risks both missing the real diagnosis and causing harm (see Correcting Low Zinc Safely).
Clues That Point Toward Zinc
Given how non-specific rashes are, it helps to have a short checklist of features that genuinely raise the suspicion of zinc. The more of these that are present together, the more zinc is worth investigating:
- The signature distribution — rash clustered around the mouth/nose, eyes, and genitals and on the hands and feet, rather than scattered randomly.
- It resists ordinary treatment — the rash shrugs off moisturizers, mild steroid creams, and antifungals that would normally help eczema or a fungal rash.
- Telltale company — hair loss and slow wound healing, a blunted sense of taste or smell, diarrhea, mouth-corner cracking, or frequent infections from weakened immunity appearing in the same person.
- A reason to be deficient — one of the situations in the next section (gut disease, bariatric surgery, alcohol use, a very restricted diet, exclusive breastfeeding of a premature infant, or long-term intravenous nutrition).
- An infant with a rash that began around weaning — a special pattern (discussed below) that should always prompt a zinc workup.
A useful real-world tell that ties several of these together is the rare inherited disease acrodermatitis enteropathica, in which a faulty intestinal zinc transporter prevents zinc absorption. Classic cases appear in infancy with the full triad of rash around the mouth and extremities, diarrhea, and hair loss — and the rash dramatically clears with zinc. That triad is the clinical fingerprint of zinc-deficient skin, and even in acquired (non-genetic) zinc deficiency, the more the picture resembles that triad, the more confident the suspicion.
What Drives Zinc Low Enough to Affect Skin
Zinc deficiency severe enough to inflame the skin rarely happens to a healthy person eating a varied diet. There is almost always a reason — either zinc isn't getting in, isn't being absorbed, or is being lost. The common drivers:
- Malabsorption from gut disease — Crohn's disease, celiac disease, and other conditions that inflame or shorten the bowel impair zinc absorption. Chronic diarrhea is a double hit: it both reduces absorption and directly flushes zinc out.
- Bariatric (weight-loss) surgery — procedures that bypass part of the small intestine reduce zinc absorption, and zinc deficiency is a recognized long-term complication that surgical teams monitor for.
- Heavy alcohol use — alcohol reduces zinc absorption and increases its loss in urine, and people with alcohol use disorder often eat poorly as well, compounding the problem.
- Diets very low in available zinc — zinc is most bioavailable from animal foods. Diets built heavily on unleavened whole grains and legumes are high in phytate, a compound that binds zinc in the gut and blocks its absorption, so a person can eat “enough” zinc on paper yet absorb too little. Strict, poorly planned plant-based diets are a recognized risk, as is severe general malnutrition (such as anorexia nervosa).
- Infancy and breastfeeding edge-cases — the dramatic acquired form occurs in some breastfed (especially premature) infants whose mother's milk is unusually low in zinc, or who have the inherited acrodermatitis enteropathica. The rash classically appears around the time of weaning, when the infant's zinc demand rises and milk zinc falls.
- Increased losses or demand — severe burns, major surgery, sickle cell disease, and long-term intravenous (parenteral) nutrition without adequate zinc can all deplete stores.
It is worth noting one nutrient interaction in the other direction, because it bears on safe treatment: too much zinc blocks copper. Long-term high-dose zinc supplementation can drive down copper levels and cause a copper-deficiency anemia and neurological problems — which is exactly why chasing a rash with megadoses of zinc can backfire. We return to this in the treatment section.
Getting Tested
Confirming zinc as the cause of a rash is partly a lab question and partly a clinical one, because zinc is a genuinely difficult mineral to measure well. The usual first test is a serum (plasma) zinc level, often ordered alongside a Comprehensive Metabolic Panel to check kidney and liver function and look for clues to malabsorption. But the serum zinc number must be read with care, for several reasons:
- Only about 0.1% of the body's zinc is in the blood, so a serum level is a crude snapshot of total body stores and can be normal even when tissue zinc is low.
- Inflammation and infection temporarily lower serum zinc regardless of true status, because the body shifts zinc out of the blood during an immune response. A low reading during an acute illness can therefore be misleading.
- Low albumin (the blood protein zinc rides on), recent meals, and even the time of day shift the result, so a fasting morning sample is preferred.
Because of these limits, doctors often lean on the clinical picture and a treatment trial as much as the number. When the rash has the signature distribution, resists standard treatment, and is accompanied by the telltale company symptoms, a brief course of zinc that produces rapid, dramatic clearing of the rash is itself strong confirmation — this response to treatment is a recognized way of clinching the diagnosis, especially in the acrodermatitis pattern. A clinician may also check a copper level (to set a safe baseline before treatment), and in an infant or a person with gut disease, additional nutritional and absorption testing. The practical message: a single zinc level neither rules zinc in nor out by itself; it is interpreted in context.
Correcting Low Zinc Safely
When zinc deficiency is genuinely the cause, the good news is that the skin usually responds quickly — often visibly improving within days to a couple of weeks of adequate repletion. The approach follows a sensible order, food first for mild shortfalls and supervised supplements for true deficiency:
- Food first, for mild shortfalls. The most bioavailable zinc comes from animal foods — beef and other red meat, shellfish, poultry, eggs and dairy — while pumpkin seeds, lentils, beans, nuts, and whole grains contribute meaningful amounts. Soaking, sprouting, and leavening (fermenting) grains and legumes lowers their phytate and frees up more of their zinc. The full food list lives on the zinc food sources page.
- Oral zinc supplements, for true deficiency. When a rash is driven by genuine deficiency, oral zinc (commonly zinc sulfate, gluconate, or acetate) is the treatment, dosed and timed by a clinician. For the inherited acrodermatitis enteropathica, lifelong zinc supplementation is required and is dramatically effective. Taking zinc with food reduces the nausea it can cause, though food (especially phytate-rich food) can also blunt absorption — timing is something the prescriber will guide.
- Mind the copper. This is the key safety point. Sustained high-dose zinc (typically well above the tolerable upper limit, taken for months) suppresses copper absorption and can cause copper-deficiency anemia and nerve damage. Anyone on long-term zinc — and certainly anyone self-treating — should not take open-ended megadoses; clinicians monitor copper and keep zinc at the lowest effective dose.
- Topical zinc has a narrower role. For acne specifically, some topical preparations combine zinc with an antibiotic, and zinc-oxide barrier creams help diaper-area and irritant rashes. But topical zinc does not correct a true dietary deficiency — that requires getting zinc into the body.
- Fix the cause. Replacing zinc without addressing why it dropped — treating the gut disease, adjusting after bariatric surgery, reducing alcohol, replanning a restrictive diet — only buys time before it falls again.
For ordinary acne in someone who is not deficient, zinc is at most a modest add-on, not a cure, and the proven acne treatments (topical retinoids, benzoyl peroxide, and others discussed on the Acne page) do the heavy lifting. Reaching for high-dose zinc to treat acne in a well-nourished person risks the copper problem above for little benefit.
When to Seek Care / Red Flags
Most rashes are not emergencies, and most can wait for a routine appointment. But certain features mean see a clinician promptly rather than continuing to self-treat — either because the rash may signal genuine deficiency that needs correcting, or because it may be something more serious than a nutrient problem:
- A rash with the signature zinc pattern — clustered around the mouth, eyes, and genitals and on the hands/feet — especially if it resists ordinary skin treatments or comes with hair loss, diarrhea, or a change in taste. This warrants a workup rather than another tube of cream.
- An infant or young child with a spreading rash around the mouth and bottom plus diarrhea or poor growth — this can be acrodermatitis enteropathica and should be evaluated without delay, as it is fully treatable once recognized.
- A rash that is rapidly spreading, blistering, peeling, or accompanied by fever, or any rash with skin peeling off in sheets or sores in the mouth or eyes — these can signal a severe drug reaction or serious infection and are medical emergencies.
- Signs of skin infection — increasing redness, warmth, swelling, pus, or spreading red streaks — particularly in someone whose immunity may be compromised.
- Severe, scarring, or psychologically distressing acne — worth seeing a dermatologist for proven treatment rather than experimenting with supplements.
- New neurological symptoms (numbness, weakness, balance trouble) or unexplained anemia in someone taking long-term high-dose zinc — possible copper deficiency from the zinc itself; stop self-dosing and seek evaluation.
The single most useful instinct is this: a rash that fits the zinc pattern and keeps its company deserves a proper evaluation, and a rash that is spreading fast, blistering, or making you systemically ill deserves urgent care. When unsure, a clinician can sort a benign rash from a serious one quickly.
Key Research Papers
- Prasad AS (2001). Discovery of human zinc deficiency: impact on human health. Nutrition;17(7-8):685-687. — DOI: 10.1016/s0899-9007(01)00598-6
- Prasad AS (2013). Discovery of Human Zinc Deficiency: Its Impact on Human Health and Disease. Advances in Nutrition;4(2):176-190. — DOI: 10.3945/an.112.003210
- Prasad AS (1985). Clinical Manifestations of Zinc Deficiency. Annual Review of Nutrition;5:341-363. — DOI: 10.1146/annurev.nu.05.070185.002013
- Gupta M, Mahajan VK, Mehta KS, Chauhan PS (2014). Zinc Therapy in Dermatology: A Review. Dermatology Research and Practice;2014:709152. — DOI: 10.1155/2014/709152
- Coromilas A, Brandling-Bennett HA, Morel KD, Garzon MC (2011). Novel SLC39A4 Mutation in Acrodermatitis Enteropathica. Pediatric Dermatology;28(6):697-700. — DOI: 10.1111/j.1525-1470.2011.01637.x
- Yee BE, Richards P, Sui JY, Marsch AF (2020). Serum zinc levels and efficacy of zinc treatment in acne vulgaris: A systematic review and meta-analysis. Dermatologic Therapy;33(6):e14252. — DOI: 10.1111/dth.14252
- Dréno B, Moyse D, Alirezai M, Amblard P, et al. (2001). Multicenter Randomized Comparative Double-Blind Controlled Clinical Trial of the Safety and Efficacy of Zinc Gluconate versus Minocycline Hydrochloride in the Treatment of Inflammatory Acne Vulgaris. Dermatology;203(2):135-140. — DOI: 10.1159/000051728
- Dessinioti C, Katsambas AD (2010). The role of Propionibacterium acnes in acne pathogenesis: facts and controversies. Clinics in Dermatology;28(1):2-7. — DOI: 10.1016/j.clindermatol.2009.03.012
- Wessels I, Maywald M, Rink L (2017). Zinc as a Gatekeeper of Immune Function. Nutrients;9(12):1286. — DOI: 10.3390/nu9121286
- Prasad AS (2008). Zinc in Human Health: Effect of Zinc on Immune Cells. Molecular Medicine;14(5-6):353-357. — DOI: 10.2119/2008-00033.prasad
- Wessels I, Fischer HJ, Rink L (2021). Dietary and Physiological Effects of Zinc on the Immune System. Annual Review of Nutrition;41:133-175. — DOI: 10.1146/annurev-nutr-122019-120635
PubMed Topic Searches
- PubMed — Zinc deficiency and acrodermatitis skin rash
- PubMed — Acrodermatitis enteropathica and the SLC39A4 zinc transporter
- PubMed — Zinc supplementation in acne vulgaris (trials)
- PubMed — Zinc, the skin barrier, and epidermal repair
- PubMed — Zinc supplementation and copper deficiency
Connections
- Zinc Deficiency Symptom Hub
- Zinc Deficiency and Weakened Immunity
- Zinc Deficiency and Loss of Taste & Smell
- Zinc Deficiency, Hair Loss & Slow Healing
- Zinc Overview
- Zinc and Skin Health
- Zinc and Wound Healing
- Zinc Food Sources
- Copper
- Acne
- Eczema
- Psoriasis
- Rosacea
- Crohn's Disease
- Celiac Disease
- Comprehensive Metabolic Panel
- Beef
- Pumpkin Seeds