Hyperphosphatemia (High Phosphate): Vascular Calcification
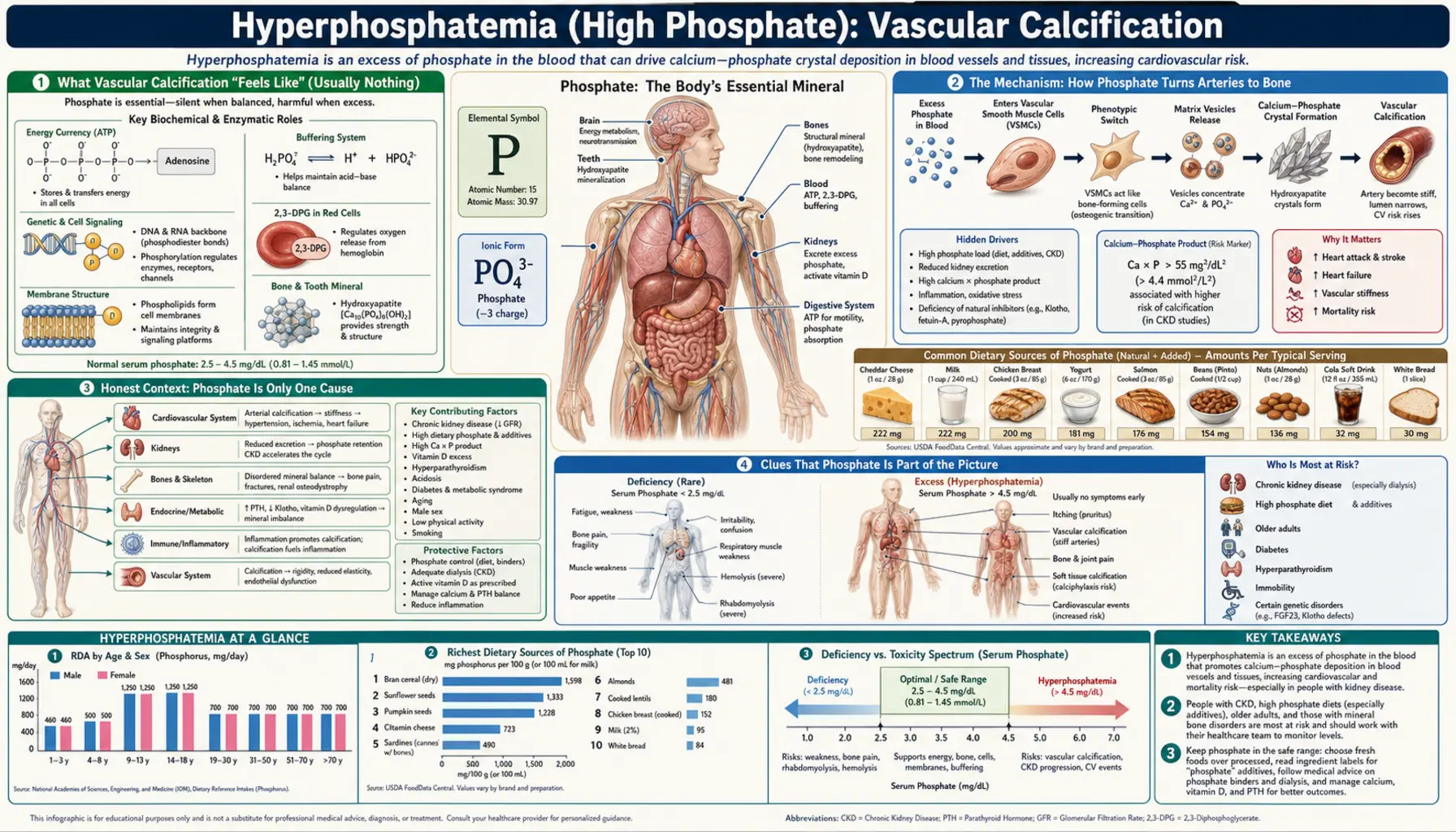
When phosphate runs high in the blood for months or years — a condition called hyperphosphatemia — calcium and phosphate can slowly crystallize inside the walls of the arteries, turning soft, elastic vessels stiff and chalky. This is vascular calcification, and it is the single most important reason high phosphate matters: it is strongly linked to heart attacks, strokes, and early death, especially in people with kidney disease. The hardest part to accept is that it is almost completely silent — you cannot feel your arteries calcifying, there is no ache or warning sign, and by the time it shows up it is usually well advanced. This page explains what vascular calcification is, the surprising biology behind it (the artery wall is not a passive pipe — it actively builds bone-like mineral), why phosphate is only one of several causes, who is truly at risk, how it is detected, and what can be done about it.
Table of Contents
- What Vascular Calcification "Feels Like" (Usually Nothing)
- The Mechanism: How Phosphate Turns Arteries to Bone
- Honest Context: Phosphate Is Only One Cause
- Clues That Phosphate Is Part of the Picture
- Common Causes of High Phosphate
- Getting Checked
- How High Phosphate Is Lowered
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Vascular Calcification "Feels Like" (Usually Nothing)
The most important thing to understand about vascular calcification is that, for most of its course, it produces no symptoms at all. Unlike a high potassium that can weaken a muscle within hours, or low calcium that can cause cramps you actually feel, the slow mineralization of an artery wall is silent. You cannot sense your arteries stiffening; there is no pain, no fluttering, no specific warning. It is a process measured in months and years, and it is usually discovered by accident — on a chest X-ray, a CT scan ordered for something else, or a blood test that shows a stubbornly high phosphate.
When effects finally do appear, they are downstream consequences of the damage, not the calcification itself:
- Stiff, high-pressure arteries. Healthy arteries are elastic; they expand with each heartbeat and recoil to keep blood flowing smoothly. Calcified arteries are rigid pipes. The result is a higher systolic blood pressure and a wider pulse pressure (a big gap between the top and bottom numbers) that the heart has to push against with every beat.
- A strained heart. Pushing blood into stiff vessels makes the heart's main pumping chamber thicken and work harder over time, which can eventually contribute to heart failure.
- Reduced blood flow. When calcium settles in the inner lining alongside cholesterol plaque, it narrows the channel — the same disease as ordinary atherosclerosis — and can show up as chest pain (coronary artery disease) or leg pain on walking (peripheral artery disease).
- Hard, stiff heart valves. The same mineral can deposit on heart valves, stiffening them and contributing to valvular heart disease, especially of the aortic valve.
So the honest framing for this page is unusual: the “symptom” is the absence of one. Vascular calcification matters not because of how it feels, but because of what it predicts — a markedly higher risk of cardiovascular events and death. That is exactly why a doctor may take a high phosphate seriously even when you feel perfectly well, and why this problem is managed by watching the numbers rather than waiting for the body to complain.
This page is about the artery wall specifically. High phosphate also drives changes in the calcium and bone system that it is tangled up with, and it can cause maddening itching — those are covered on their own pages so this one can stay focused.
The Mechanism: How Phosphate Turns Arteries to Bone
For most of the twentieth century, doctors assumed calcified arteries were just a passive chemistry problem: too much calcium and phosphate floating in the blood, eventually precipitating like limescale in an old kettle. That picture turns out to be only half right — and the half it gets wrong is the important half. The modern understanding, built on a series of landmark experiments around the year 2000, is that vascular calcification is an active, regulated process. The artery is not a dumb pipe that scales up; under the wrong conditions it is coaxed into building bone.
The key cell is the vascular smooth muscle cell, the cell that gives the artery wall its tone and elasticity. In a now-classic 2000 experiment, researchers showed that simply raising the phosphate concentration in the fluid bathing these cells caused them to lay down calcium-phosphate mineral — and, remarkably, to switch on the genetic program of a bone-building cell. Phosphate gets into the smooth muscle cell through a dedicated doorway, a sodium-dependent phosphate cotransporter (called PiT-1). Once inside in excess, the phosphate acts as a signal, not just a raw material: the smooth muscle cell begins to behave like an osteoblast, the cell that normally builds your skeleton. It starts expressing bone proteins, organizing mineral, and effectively turning a stretch of artery into something closer to bone.
An analogy. Think of the artery wall as a garden hose, and think of your body as having a full-time crew of gardeners whose job is to stop mineral from forming on the hose. Normally that crew wins easily, and the hose stays soft and flexible. Persistently high phosphate does two things at once: it floods the area with the raw cement for mineral, and it bribes some of the gardeners into switching sides — they stop preventing mineral and start actively troweling it onto the hose. Over years, patches of the hose harden into something like concrete pipe. This is why the process is so hard to reverse and why prevention beats cure: once an artery has been instructed to build bone, telling it to stop is much harder than never giving the order.
The body does have powerful natural defenses against this, which is why most people with a brief or modest phosphate bump never calcify. Inhibitors such as pyrophosphate, fetuin-A, and matrix Gla protein normally patrol the bloodstream and vessel wall, dissolving tiny mineral seeds before they can grow. Vascular calcification takes hold when the balance tips — when high phosphate (and often high calcium) overwhelms these guards, or when disease lowers the guards themselves. That tug-of-war between mineral-formers and mineral-inhibitors is the heart of the modern theory, and it explains why phosphate is dangerous chiefly when it is high for a long time and alongside other failures, not after a single big meal.
One more piece completes the picture. As the kidneys begin to fail, the body fights rising phosphate by ramping up two hormones — fibroblast growth factor 23 (FGF23) and parathyroid hormone (PTH) — that push the kidney to dump more phosphate. For a while this keeps the blood level normal, which is why phosphate often looks fine until kidney disease is advanced. But these same hormonal changes, sustained over years, disturb the whole calcium-phosphate-vitamin D system and themselves contribute to vessel and bone damage. By the time the blood phosphate is frankly high, the underlying mineral disorder has usually been brewing for a long time.
Honest Context: Phosphate Is Only One Cause
It would be misleading to leave you thinking that high phosphate is the cause of hardened arteries, or that a calcified artery proves your phosphate is too high. Neither is true, and the honest picture matters.
Vascular calcification is common, and most of it has nothing to do with phosphate. The two big patterns are:
- Intimal calcification — calcium deposited within cholesterol plaque in the inner lining of the artery. This is part of ordinary atherosclerosis, the disease driven over decades by aging, high LDL cholesterol, high blood pressure, smoking, and diabetes. The great majority of coronary calcium found on scans in the general population is this type, and it reflects plaque burden far more than it reflects phosphate.
- Medial calcification — calcium deposited in the muscular middle layer of the artery wall, stiffening it without necessarily narrowing it. This is the pattern most tightly linked to high phosphate, chronic kidney disease, and diabetes, and it is the one driven by the bone-building mechanism described above.
In real patients the two overlap. So the truthful statement is this: high phosphate is one important, modifiable driver of vascular calcification — especially the medial type in people with kidney disease — but it sits among many other causes, several of which (cholesterol, blood pressure, smoking, diabetes, and aging itself) usually matter more in the general population. Finding calcium in your arteries should prompt attention to all of these, not phosphate alone. And a normal phosphate level does not mean your arteries are protected, because the dominant driver may be something else entirely.
This is also why you should be wary of anyone selling a single “artery-clearing” supplement or claiming that cutting one nutrient will reverse calcification. The biology is multifactorial, the deposits are slow to form and slow to shift, and the evidence base for dramatic reversal is thin. The realistic goal is to slow progression by correcting the drivers that can be corrected.
Clues That Phosphate Is Part of the Picture
Because calcification itself is silent and has many causes, the question that actually matters is: when should phosphate be suspected as a contributor? The clues are about context, not symptoms.
- Chronic kidney disease, above all. This is the dominant setting. As kidney function declines, the ability to excrete phosphate falls, the protective hormone system goes awry, and the medial, phosphate-driven type of calcification accelerates. People on dialysis have the highest risk, and calcification can appear strikingly early — even young adults on dialysis can have coronary calcium scores like those of much older people. If you have known kidney disease and calcified arteries, phosphate is very likely part of the story.
- A persistently high phosphate on blood tests — not a single high reading, but a level that stays above the normal range over time, particularly together with a high calcium × phosphate product (the two multiplied), which historically tracked with worse outcomes.
- Calcification that is out of proportion to the usual risk factors — for instance, heavy, diffuse medial-pattern calcification in someone who does not smoke and has normal cholesterol, especially with kidney disease, points toward the mineral pathway rather than ordinary plaque.
- Companion features of disordered mineral balance — the same high phosphate that calcifies arteries often shows up alongside the calcium and bone problems of kidney disease and, when very high, relentless itching. When those travel together, the whole mineral system — not just one number — needs attention.
Conversely, in an otherwise healthy person with normal kidneys and a normal phosphate, calcified arteries almost always reflect age and conventional cardiovascular risk factors, and the focus belongs on cholesterol, blood pressure, and lifestyle rather than phosphate.
Common Causes of High Phosphate
Healthy kidneys are extraordinarily good at clearing phosphate, so a sustained high level almost always means the kidneys cannot keep up, or that phosphate is being released or absorbed faster than they can excrete it. The common setups are:
- Chronic kidney disease. This is by far the leading cause. As filtering capacity declines, phosphate that would normally be excreted in urine accumulates in the blood. The level often stays normal until kidney function is well below half, then climbs — which is why advanced kidney disease and dialysis are where dangerous hyperphosphatemia and its calcification live. See chronic kidney disease and acute kidney injury.
- Too much phosphate coming in, in the wrong setting. In someone with reduced kidney function, a high phosphate diet can tip the balance — and a major hidden source is phosphate additives in processed foods, fast food, colas, and many packaged products. These inorganic additives are absorbed far more completely than the phosphorus naturally bound in whole foods, so they punch above their weight. Phosphate-containing laxatives or enemas can also cause sharp, sometimes dangerous spikes, particularly in older adults or anyone with kidney impairment.
- Tissue breakdown that dumps phosphate from inside cells. Phosphate is highly concentrated inside cells, so anything that destroys cells in bulk floods the blood: muscle breakdown (rhabdomyolysis), the rapid die-off of cancer cells during chemotherapy (tumor lysis syndrome), and severe tissue injury. These can raise phosphate quickly.
- Hormonal causes. Conditions that lower parathyroid hormone — which normally tells the kidney to excrete phosphate — raise it instead (hypoparathyroidism). Note the contrast with hyperparathyroidism, where excess PTH typically lowers phosphate; the parathyroid–phosphate relationship is a key part of the whole mineral picture. Severe vitamin D excess can also raise phosphate by driving up gut absorption (see vitamin D).
Pinning down the cause matters because the fix differs sharply: managing kidney disease, cutting phosphate additives, stopping a phosphate enema, treating the underlying breakdown, or correcting a hormone problem are very different interventions. In practice the first steps are reviewing kidney function and taking an honest look at the diet, especially processed and fast foods.
Getting Checked
Two separate questions get answered with two separate tools: is the phosphate high? (a blood test), and are the arteries calcifying? (imaging).
The first is a simple blood test. A Comprehensive Metabolic Panel reports kidney function (creatinine), calcium, and glucose, but note that the basic panel does not always include phosphate — the serum phosphate is often a separate add-on test, so it may need to be requested specifically. When the mineral system is being evaluated properly, a clinician typically checks phosphate together with calcium, parathyroid hormone (PTH), and vitamin D, because these move together and the pattern across all four — not phosphate alone — tells the real story. The normal adult serum phosphate is roughly 2.5–4.5 mg/dL, though laboratories vary and children normally run higher.
The second question — the state of the arteries — is answered by imaging. A coronary artery calcium (CAC) score is a low-dose CT scan that measures how much calcium is in the coronary arteries and reports a number; a higher score means more calcified plaque and, in the general population, a higher cardiovascular risk. Calcification is also frequently spotted incidentally on chest X-rays, mammograms, and CT scans done for other reasons. It is worth understanding what these tests do and do not say: a calcium score reflects total calcified burden, much of which is ordinary atherosclerotic plaque, so it is a powerful marker of cardiovascular risk but does not by itself tell you that phosphate is to blame. Interpreting it means putting it together with the blood work and the clinical context, above all whether kidney disease is present.
How High Phosphate Is Lowered
The realistic aim of treatment is to bring phosphate back toward the normal range and keep it there, in the hope of slowing further calcification — not to dissolve mineral that has already formed, which the body does only very slowly if at all. For people with chronic kidney disease, this is a long-term, three-part effort done with a nephrology team:
- Cut phosphate intake, smartly. The biggest, most underused lever is eliminating inorganic phosphate additives in processed foods, fast food, and colas, because they are absorbed almost completely. This often lowers phosphate more, and more painlessly, than restricting healthy whole foods. A renal dietitian helps strike the balance — cutting additives and the worst offenders while preserving enough protein, which matters because protein-rich foods carry phosphorus but are still essential.
- Block absorption with phosphate binders. When diet alone is not enough — which is usual in advanced kidney disease — phosphate binders taken with meals grab dietary phosphate in the gut so it passes out in the stool instead of being absorbed. Several types exist; non-calcium binders are often preferred specifically to avoid adding to the body's calcium load and feeding the calcification process.
- Remove phosphate and manage the whole mineral system. In people on dialysis, the dialysis treatment itself removes some phosphate, though usually not enough on its own. Alongside this, clinicians manage the linked hormones — controlling parathyroid hormone and using vitamin D carefully — because the goal set out in the major kidney guidelines is to normalize the pattern of phosphate, calcium, and PTH together, not to chase a single number.
For everyone, including those without kidney disease, the deepest point bears repeating: because calcification is multifactorial and hard to reverse, the most effective “treatment” for the arteries is to address the bigger drivers in parallel — cholesterol, blood pressure, blood sugar, and not smoking — and, in kidney disease, to catch and control phosphate early, before the artery wall has been given years of instructions to build bone.
When to Seek Care / Red Flags
Vascular calcification itself is silent, so the red flags are not about the calcification — they are about its consequences and about catching high phosphate before it does harm. Treat the following as reasons to seek medical attention, and the emergencies as reasons to call emergency services right away:
- Chest pain or pressure, breathlessness, or pain spreading to the arm or jaw — possible heart attack. Call emergency services immediately; do not wait.
- Sudden weakness, facial droop, slurred speech, or loss of vision — possible stroke. Call emergency services immediately.
- New or worsening leg pain when walking that eases with rest — a sign of reduced circulation from peripheral artery disease that warrants prompt evaluation.
- Known kidney disease with a phosphate that will not come down, or a phosphate you cannot keep in range despite diet and binders — this needs review with your kidney team, because persistently high phosphate is the setup for accelerating calcification.
- Extremely painful skin ulcers or hard, tender skin lumps in someone with advanced kidney disease — this can signal calciphylaxis, a rare but life-threatening condition in which calcium deposits block small skin blood vessels. It is a medical emergency and needs urgent specialist care.
The constructive takeaway is the opposite of alarm: because the process is silent and slow, the real opportunity is to act before any of these red flags appear — by having phosphate and kidney function checked if you are at risk, by controlling conventional heart risk factors, and by treating a high phosphate as a number worth correcting even when, as is almost always the case, you feel completely well.
Key Research Papers
- Block GA, Hulbert-Shearon TE, Levin NW, Port FK (1998). Association of serum phosphorus and calcium x phosphate product with mortality risk in chronic hemodialysis patients. American Journal of Kidney Diseases;31(4):607-617. — DOI: 10.1053/ajkd.1998.v31.pm9531176
- Goodman WG, Goldin J, Kuizon BD, et al. (2000). Coronary-Artery Calcification in Young Adults with End-Stage Renal Disease Who Are Undergoing Dialysis. New England Journal of Medicine;342(20):1478-1483. — DOI: 10.1056/NEJM200005183422003
- Jono S, McKee MD, Murry CE, et al. (2000). Phosphate Regulation of Vascular Smooth Muscle Cell Calcification. Circulation Research;87(7):e10-e17. — DOI: 10.1161/01.RES.87.7.e10
- Kestenbaum B, Sampson JN, Rudser KD, et al. (2005). Serum Phosphate Levels and Mortality Risk among People with Chronic Kidney Disease. Journal of the American Society of Nephrology;16(2):520-528. — DOI: 10.1681/ASN.2004070602
- Tonelli M, Sacks F, Pfeffer M, et al. (2005). Relation Between Serum Phosphate Level and Cardiovascular Event Rate in People With Coronary Disease. Circulation;112(17):2627-2633. — DOI: 10.1161/CIRCULATIONAHA.105.553198
- Giachelli CM (2005). Regulation of Vascular Calcification: Roles of Phosphate and Osteopontin. Circulation Research;96(7):717-722. — DOI: 10.1161/01.RES.0000161997.24797.c0
- Razzaque MS, Lanske B (2007). The emerging role of the fibroblast growth factor-23–klotho axis in renal regulation of phosphate homeostasis. Journal of Endocrinology;194(1):1-10. — DOI: 10.1677/joe-07-0095
- Mizobuchi M, Towler D, Slatopolsky E (2009). Vascular Calcification: The Killer of Patients with Chronic Kidney Disease. Journal of the American Society of Nephrology;20(7):1453-1464. — DOI: 10.1681/ASN.2008070692
- Shanahan CM, Crouthamel MH, Kapustin A, Giachelli CM (2011). Arterial Calcification in Chronic Kidney Disease: Key Roles for Calcium and Phosphate. Circulation Research;109(6):697-711. — DOI: 10.1161/CIRCRESAHA.110.234914
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Update Work Group (2017). KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease–Mineral and Bone Disorder (CKD-MBD). Kidney International Supplements;7(1):1-59. — DOI: 10.1016/j.kisu.2017.04.001
- Nigwekar SU, Thadhani R, Brandenburg VM (2018). Calciphylaxis. New England Journal of Medicine;378(18):1704-1714. — DOI: 10.1056/NEJMra1505292
PubMed Topic Searches
- PubMed — Hyperphosphatemia and vascular calcification
- PubMed — Phosphate, smooth muscle cells, and osteoblast-like change
- PubMed — Serum phosphate, cardiovascular events, and mortality in CKD
- PubMed — Medial arterial calcification in kidney disease
- PubMed — Phosphate binders and CKD-MBD treatment
Connections
- Hyperphosphatemia Symptom Hub
- Hyperphosphatemia and Calcium & Bone Problems
- Hyperphosphatemia and Itching
- Phosphorus Deficiency Hub
- Phosphorus Overview
- Phosphorus and Bone Mineralization
- Calcium
- Calcium Toxicity (Hypercalcemia)
- Magnesium
- Vitamin D
- Chronic Kidney Disease
- Acute Kidney Injury
- Hyperparathyroidism
- Atherosclerosis
- Coronary Artery Disease
- Peripheral Artery Disease
- Valvular Heart Disease
- Hypertension
- Coronary Calcium Score
- Comprehensive Metabolic Panel