ANA Test: Antinuclear Antibody for Autoimmune Disease
The antinuclear antibody (ANA) test is the primary screening tool for systemic autoimmune diseases. It detects autoantibodies directed against components of the cell nucleus and is positive in more than 95% of patients with systemic lupus erythematosus (SLE). Understanding the ANA result requires interpreting titer, fluorescence pattern, and clinical context together — a positive result alone does not diagnose any disease.
Table of Contents
- Overview
- When Ordered
- HEp-2 Cell Patterns
- Titer Interpretation
- Positive ANA in Healthy Adults
- Associated Autoimmune Diseases
- Reflex Testing
- Clinical Context and Limitations
- References
- Featured Videos
Overview
The ANA (antinuclear antibody) test detects autoantibodies that target components of the cell nucleus — including DNA, histones, RNA-binding proteins, and nuclear enzymes. These autoantibodies are a hallmark of systemic autoimmune connective tissue diseases, where the immune system mistakenly attacks the body's own nuclear material.
ANA is the primary screening test for systemic autoimmune diseases, particularly:
- Systemic lupus erythematosus (SLE) — ANA positive in >95% of cases
- Sjögren's syndrome — positive in approximately 70% of patients
- Systemic sclerosis (scleroderma) — positive in up to 95% of cases
- Polymyositis and dermatomyositis — positive in 20–30%, with specific myositis-associated antibodies
- Mixed connective tissue disease (MCTD) — positive in virtually 100%, with high-titer anti-U1-RNP
The test is performed by indirect immunofluorescence (IIF) on HEp-2 cells, which are a human epithelial cell line whose large nuclei make nuclear fluorescence patterns easy to visualize. Many laboratories also use ELISA or multiplex bead-based assays for initial screening, though IIF remains the gold standard. ANA has high sensitivity (95% for SLE) but low specificity — meaning a positive result requires careful interpretation in clinical context.
When Ordered
A clinician orders an ANA panel when the patient presents with symptoms that could indicate a systemic autoimmune connective tissue disease. Appropriate indications include:
- Persistent fatigue with joint pain — especially polyarthralgia or inflammatory arthritis in multiple joints
- Butterfly (malar) rash — fixed erythema across the cheeks and nasal bridge, sparing the nasolabial folds; hallmark of SLE
- Raynaud's phenomenon — episodic vasospasm of fingers/toes triggered by cold or stress; associated with multiple connective tissue diseases
- Unexplained serositis — pleuritis (pleurisy), pericarditis, or peritonitis without infectious cause
- Dry eyes and dry mouth (sicca symptoms) — cardinal features of Sjögren's syndrome
- Unexplained cytopenias — immune-mediated low platelet count (thrombocytopenia) or low white blood cell count (leukopenia)
- Photosensitivity — unusual skin reactions to sun exposure
- Recurrent pregnancy loss — antiphospholipid syndrome and lupus are leading causes of recurrent miscarriage
- Skin thickening — especially progressive hardening of the fingers, hands, or face, suggesting systemic sclerosis
- Unexplained renal disease — lupus nephritis can present with hematuria, proteinuria, or declining kidney function
- Monitoring known autoimmune disease — periodic retesting may be appropriate when disease activity changes
ANA should not be ordered as a general wellness screening test in patients without symptoms, as the high background rate of low-titer positives in the healthy population leads to unnecessary anxiety and further testing.
HEp-2 Cell Patterns
When ANA is performed by indirect immunofluorescence (IIF) on HEp-2 cells, the pattern of nuclear fluorescence provides important diagnostic guidance. Different patterns reflect which nuclear antigens the autoantibodies are targeting, and each pattern directs which specific antibody tests to order next.
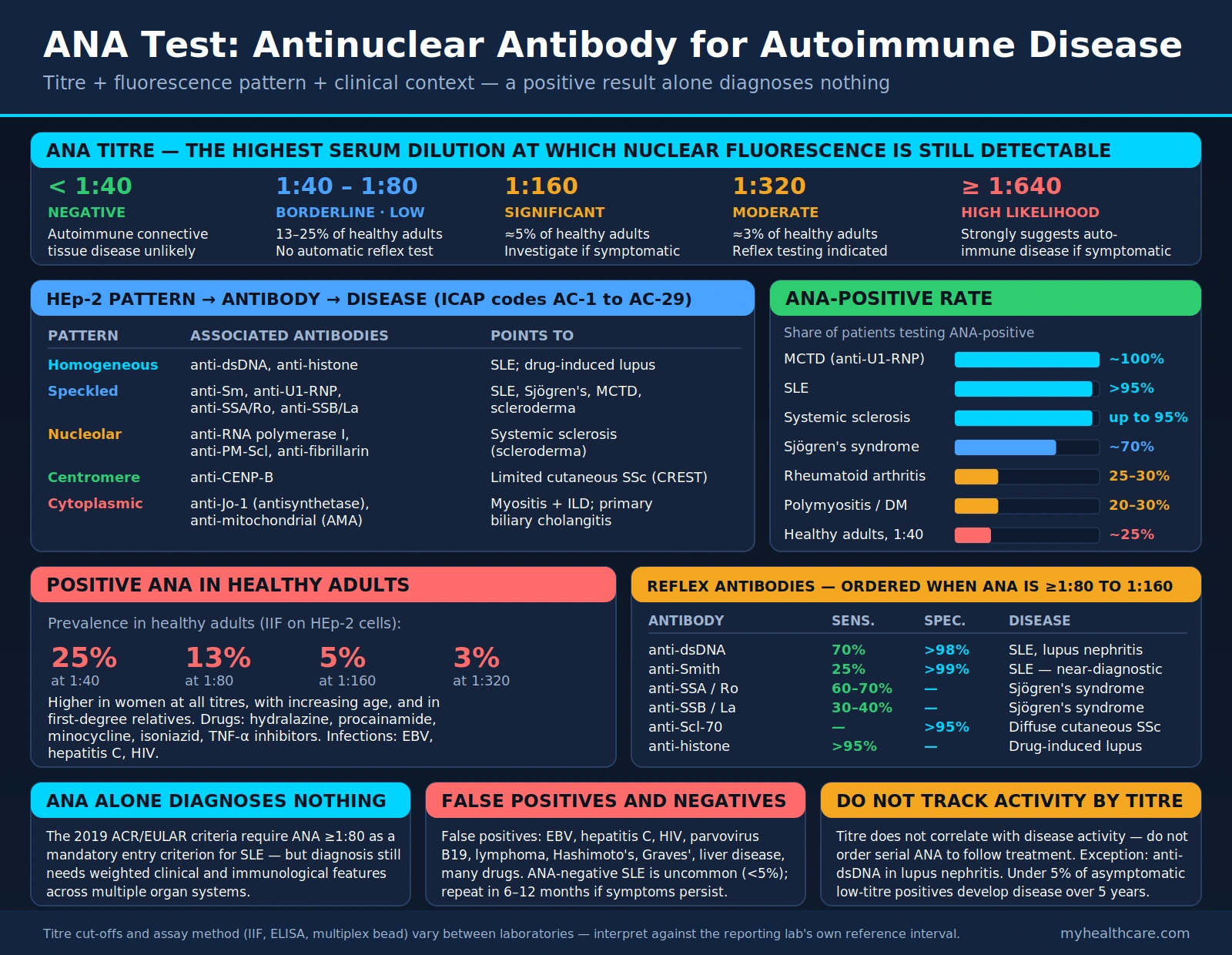
- Homogeneous (diffuse) pattern: The most common pattern. The entire nucleus stains uniformly, including the chromosomes in dividing cells. Associated with anti-double-stranded DNA (anti-dsDNA) and anti-histone antibodies. Seen in SLE and drug-induced lupus. A high-titer homogeneous pattern with symptoms of SLE strongly warrants anti-dsDNA and anti-Smith reflex testing.
- Speckled pattern: Fine or coarse discrete dots scattered throughout the nucleus, sparing the nucleolus. One of the most common patterns. Associated with anti-Sm, anti-U1-RNP, anti-SSA/Ro, and anti-SSB/La antibodies. Seen in SLE, Sjögren's syndrome, mixed connective tissue disease, and scleroderma. Fine speckled often suggests anti-SSA/SSB; coarse speckled often suggests anti-Sm or anti-RNP.
- Nucleolar pattern: Staining concentrated in the nucleolus (the RNA-synthesis center of the nucleus). Strongly associated with systemic sclerosis (scleroderma). Specific antibodies include anti-RNA polymerase I, anti-PM-Scl (overlap myositis/scleroderma), and anti-fibrillarin (anti-U3-RNP). A nucleolar pattern warrants reflex testing for scleroderma-specific antibodies.
- Centromere pattern: Multiple discrete, evenly spaced dots corresponding to the centromere regions of chromosomes. Seen clearly in dividing cells. Pathognomonic for anti-centromere protein B (anti-CENP-B) antibodies. Strongly associated with limited cutaneous systemic sclerosis (lcSSc), formerly called CREST syndrome (Calcinosis, Raynaud's, Esophageal dysmotility, Sclerodactyly, Telangiectasia). The centromere pattern is relatively specific — a positive result in a patient with Raynaud's phenomenon is highly suggestive of early limited scleroderma.
- Cytoplasmic pattern: Staining in the cytoplasm rather than the nucleus. Technically not an antinuclear antibody, but detected on HEp-2 cells and reported as ANA-positive by many labs. Associated with anti-Jo-1 (anti-histidyl-tRNA synthetase) and related antisynthetase antibodies that cause the antisynthetase syndrome (inflammatory myositis + interstitial lung disease + mechanic's hands + Raynaud's). Anti-mitochondrial antibodies (primary biliary cholangitis) also produce a cytoplasmic pattern.
Standardized pattern nomenclature is provided by the International Consensus on ANA Patterns (ICAP), which classifies patterns hierarchically and assigns them alphanumeric codes (AC-1 through AC-29) to improve reporting consistency across laboratories.
Titer Interpretation
The ANA titer is reported as a dilution ratio, representing the highest dilution of the patient's serum at which antinuclear fluorescence is still detectable. Higher titers indicate greater quantities of autoantibody.
ANA Titer — Clinical Significance
ANA Titer — Disease Likelihood
- <1:40 (Negative): Not clinically significant. Autoimmune connective tissue disease is unlikely, though rare ANA-negative SLE cases occur (usually anti-SSA-positive Sjögren's overlap).
- 1:40–1:80 (Borderline): Present in a substantial proportion of healthy adults (13–25%). Low clinical significance without accompanying symptoms. Does not warrant automatic reflex testing.
- 1:160 (Clinically significant threshold): Warrants further investigation in a symptomatic patient. Present in approximately 5% of the healthy population, so still requires clinical correlation.
- 1:320 or higher: Increasingly associated with true autoimmune disease. In a patient with compatible symptoms, reflex antibody testing is clearly indicated.
- 1:640 or higher: Strongly suggestive of an underlying autoimmune connective tissue disease in a symptomatic patient.
Important caveat: ANA titer generally does not correlate with disease activity and should not be used to monitor disease flares. The notable exception is anti-dsDNA in SLE, where rising titers often precede or accompany lupus nephritis flares and are used to guide treatment decisions.
Positive ANA in Healthy Adults
One of the most clinically important facts about the ANA test is its high background positivity in the general healthy population. This makes indiscriminate ordering of ANA a significant source of false alarms, unnecessary specialist referrals, and patient anxiety.
Population prevalence of ANA positivity in healthy adults (IIF on HEp-2 cells):
- At 1:40 dilution: approximately 25% of the healthy population
- At 1:80 dilution: approximately 13% of the healthy population
- At 1:160 dilution: approximately 5% of the healthy population
- At 1:320 dilution: approximately 3% of the healthy population
Several factors increase the background rate of ANA positivity in otherwise healthy individuals:
- Sex: Women test ANA-positive more frequently than men at all titers, even without autoimmune disease
- Age: ANA prevalence increases with age in the general population
- First-degree relatives of autoimmune patients: Genetic predisposition increases ANA positivity even in asymptomatic family members
- Medications: Numerous drugs (hydralazine, procainamide, minocycline, isoniazid, TNF-alpha inhibitors) can induce transient ANA positivity
- Infections: Viral infections including EBV, hepatitis C, and HIV transiently trigger ANA production
Low-titer positive ANA results (1:40–1:80) in asymptomatic individuals rarely progress to autoimmune disease. Long-term follow-up studies show that fewer than 5% of asymptomatic low-titer ANA-positive individuals develop a defined autoimmune disease over 5 years. This is why clinical context is essential — ANA should be ordered only when there is genuine suspicion based on symptoms, physical examination, or laboratory findings.
Associated Autoimmune Diseases
Different autoimmune diseases have characteristic ANA positivity rates and associated specific antibody profiles. Understanding these associations helps determine which reflex tests to order when ANA is positive.
- Systemic lupus erythematosus (SLE): ANA positive in >95% of patients. The most ANA-sensitive autoimmune disease. Specific antibodies include anti-dsDNA (70% sensitive, >98% specific for SLE) and anti-Smith (anti-Sm: only 25% sensitive but >99% specific). Both are included in ACR/EULAR 2019 SLE classification criteria.
- Sjögren's syndrome: ANA positive in approximately 70% of patients. Anti-SSA (anti-Ro) is present in 60–70% and anti-SSB (anti-La) in 30–40%. Anti-SSA can be present with a negative ANA (ANA-negative Sjögren's), which is why direct anti-SSA testing may be warranted even when ANA is negative. Anti-SSA also causes neonatal lupus and congenital heart block in babies of positive mothers.
- Systemic sclerosis (scleroderma): ANA positive in up to 95% of patients, making it second only to SLE in ANA sensitivity. Two major disease subsets have distinct antibody profiles: anti-topoisomerase I (anti-Scl-70) in diffuse cutaneous SSc (associated with pulmonary fibrosis), and anti-centromere antibodies (anti-CENP-B) in limited cutaneous SSc/CREST syndrome (associated with pulmonary arterial hypertension).
- Drug-induced lupus (DIL): Anti-histone antibodies are the characteristic finding, present in >95% of drug-induced lupus cases. Implicated drugs include hydralazine (antihypertensive), procainamide (antiarrhythmic), isoniazid (tuberculosis treatment), minocycline (antibiotic), and TNF-alpha inhibitors (biologics). Drug-induced lupus typically resolves when the offending drug is discontinued.
- Mixed connective tissue disease (MCTD): Defined by the presence of high-titer anti-U1-RNP antibodies alongside an overlap of SLE, scleroderma, and polymyositis features. ANA positive in virtually 100% of MCTD patients, typically with a coarse speckled pattern at very high titers.
- Polymyositis and dermatomyositis: ANA positive in 20–30% of patients. The antisynthetase syndrome — characterized by anti-Jo-1 antibodies — includes inflammatory myositis, interstitial lung disease, Raynaud's phenomenon, and mechanic's hands. Anti-Jo-1 is the most common myositis-specific antibody.
- Rheumatoid arthritis (RA): Weakly positive ANA found in 25–30% of RA patients, but this is not diagnostically useful. Anti-cyclic citrullinated peptide (anti-CCP) and rheumatoid factor (RF) are the specific diagnostic antibodies for RA. ANA positivity in RA often reflects an overlap with another connective tissue disease.
- Primary biliary cholangitis (PBC): Anti-mitochondrial antibodies (AMA) are the hallmark finding (>95% sensitivity). ANA with a cytoplasmic or rim pattern may also be seen.
Reflex Testing
When ANA is positive at a clinically significant titer (≥1:80 to 1:160, depending on laboratory and clinical context), the next step is to test for specific antinuclear antibodies to identify which disease is most likely. This is called "reflex testing." The fluorescence pattern on HEp-2 cells guides which specific tests to order.
- Anti-double-stranded DNA (anti-dsDNA): Ordered when SLE is suspected, especially with homogeneous pattern. Anti-dsDNA is highly specific for SLE (>98%) and correlates with lupus nephritis activity. Rising anti-dsDNA titers often precede kidney flares. Used both for diagnosis and ongoing monitoring of SLE disease activity.
- Anti-Smith (anti-Sm): Extremely specific for SLE (>99%) but only 25% sensitive. When positive, it is virtually diagnostic of SLE. Part of the ACR/EULAR 2019 SLE classification criteria. Ordered alongside anti-dsDNA in suspected SLE.
- Anti-SSA (anti-Ro) and anti-SSB (anti-La): Characteristic of Sjögren's syndrome. Anti-SSA also causes neonatal lupus and congenital complete heart block — women of childbearing age who test positive require fetal cardiac monitoring during pregnancy. Both antibodies can be present in SLE as well.
- Anti-topoisomerase I (anti-Scl-70): Specific for diffuse cutaneous systemic sclerosis (>95% specificity). Associated with a higher risk of pulmonary fibrosis and more severe, rapidly progressive skin disease. Nucleolar or fine speckled ANA pattern prompts this test.
- Anti-centromere (anti-CENP-B): Highly specific for limited cutaneous systemic sclerosis/CREST syndrome. Centromere ANA pattern is virtually diagnostic. Associated with pulmonary arterial hypertension (not pulmonary fibrosis), esophageal dysmotility, and calcinosis.
- Anti-Jo-1 (anti-histidyl-tRNA synthetase): The signature antibody of antisynthetase syndrome. When positive in a patient with muscle weakness and elevated creatine kinase (CK), it indicates inflammatory myopathy. Associated with a high risk of interstitial lung disease. Cytoplasmic ANA pattern prompts this test.
- Anti-U1-RNP: High-titer anti-U1-RNP is required for the diagnosis of mixed connective tissue disease. Also present in SLE (as part of anti-Sm complex). Coarse speckled ANA pattern at very high titer warrants this test.
- Anti-histone: Present in >95% of drug-induced lupus cases. Ordered when DIL is suspected — patient on a known DIL-causing drug who develops lupus-like symptoms. Anti-histone can also be positive in SLE without drug exposure, so the diagnosis of DIL requires both the antibody and temporal association with the drug.
Many laboratories offer an "ANA reflex panel" that automatically tests for multiple specific antibodies when ANA is positive, streamlining the diagnostic workup.
Clinical Context and Limitations
The ANA test is a screening tool, not a standalone diagnostic test. Several important clinical principles govern its interpretation:
- ANA alone does not diagnose SLE or any autoimmune disease. The 2019 ACR/EULAR classification criteria for SLE require ANA positivity (≥1:80) as a mandatory entry criterion, but diagnosis also requires accumulating clinical and immunological features across multiple organ systems scored on a weighted scale. A positive ANA is necessary but far from sufficient.
- False positives are common. Infections (EBV, hepatitis C, HIV, parvovirus B19), malignancy (especially lymphomas), thyroid disease (Hashimoto's thyroiditis, Graves' disease), liver disease, and numerous medications cause transient or persistent low-titer ANA positivity without underlying connective tissue disease.
- False negatives are rare but occur. True ANA-negative SLE is uncommon (<5%) and is usually associated with anti-SSA-positive Sjögren's overlap. ANA-negative patients with strong clinical features warrant direct anti-SSA, anti-dsDNA, and anti-Sm testing regardless of ANA result.
- Repeat testing may capture early disease. Some patients have an ANA-negative result early in their illness that converts to positive as the disease evolves. Repeating ANA in 6–12 months is reasonable in patients with persistent symptoms but an initially negative result.
- Titer fluctuation does not reliably reflect disease activity for most autoimmune diseases. Do not order serial ANA titers to monitor treatment response, except in specific contexts such as anti-dsDNA in lupus nephritis.
- Laboratory methodology matters. IIF on HEp-2 cells is the gold-standard method. ELISA and multiplex bead assays are faster and cheaper but may have different sensitivity and specificity characteristics. A result from one method may not be directly comparable to another.
- Refer to a rheumatologist for positive results with symptoms. Interpretation of a positive ANA in the context of systemic symptoms, pattern, titer, and specific reflex antibodies is a specialized clinical skill. Rheumatology referral is appropriate for patients with a clinically significant positive ANA and compatible symptoms.
References
The following are curated PubMed literature searches covering the evidence base for ANA testing, pattern interpretation, and clinical management. Each link opens a live, filtered PubMed query so the results stay current as new studies are indexed.
- Antinuclear antibody ANA test interpretation — PubMed literature search
- ANA HEp-2 immunofluorescence patterns — PubMed literature search
- ANA positive healthy adults prevalence — PubMed literature search
- Anti-dsDNA antibody lupus diagnosis — PubMed literature search
- Anti-Smith antibody SLE specificity — PubMed literature search
- Anti-SSA Sjögren's syndrome diagnosis — PubMed literature search
- Systemic sclerosis antinuclear antibody — PubMed literature search
- Drug-induced lupus anti-histone antibody — PubMed literature search
- ANA reflex testing autoimmune disease — PubMed literature search
- Mixed connective tissue disease anti-RNP — PubMed literature search
- Antinuclear antibody screening guidelines — PubMed literature search
- 2019 ACR/EULAR lupus classification criteria — PubMed literature search
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- American College of Rheumatology — Lupus Patient Resources
Connections
- All Lab Tests
- Lupus (SLE)
- Sjögren's Syndrome
- Rheumatoid Arthritis
- Scleroderma
- Polymyositis
- Dermatomyositis
- Inflammatory Markers
- ESR Test
- Ferritin Test
- Complete Blood Count
- Comprehensive Metabolic Panel
- Vitamin D Test
- Antiphospholipid Syndrome
- Lupus Nephritis
- Pericarditis
- Hashimoto's Thyroiditis
- Primary Biliary Cholangitis
- Vitamin D3