ESR Test: Erythrocyte Sedimentation Rate and Inflammation
The erythrocyte sedimentation rate (ESR) is one of the oldest and simplest blood tests in medicine, measuring how quickly red blood cells settle to the bottom of a test tube in one hour. It is a nonspecific marker of systemic inflammation — reliable, inexpensive, and well-validated for conditions like polymyalgia rheumatica and temporal arteritis, where it plays a central diagnostic and monitoring role.
Table of Contents
- Overview
- When Ordered
- Westergren Method
- Normal Values by Age and Sex
- Acute-Phase Proteins and Fibrinogen
- ESR vs CRP Comparison
- Polymyalgia Rheumatica and GCA
- Limitations and Confounders
- References
- Featured Videos
Overview
The erythrocyte sedimentation rate (ESR) is one of the oldest and simplest blood tests in medicine, measuring how quickly red blood cells settle to the bottom of a test tube in one hour. It is a nonspecific marker of systemic inflammation — when inflammation is present, proteins called acute-phase reactants (especially fibrinogen) cause red blood cells to clump together (rouleaux formation) and sink faster.
The ESR does not identify where inflammation is occurring or its cause, but it reliably signals that significant inflammation is present somewhere in the body. It has been used clinically since the early 20th century and remains valuable today because it is inexpensive, reproducible, and well-validated for specific conditions like polymyalgia rheumatica and temporal arteritis.
The test's greatest strengths are its simplicity and its track record in rheumatology. Decades of clinical experience with ESR in specific disease states give it a practical utility that newer, more specific markers have not entirely replaced. Understanding what it measures — and what it cannot tell you — allows it to be interpreted accurately alongside clinical findings and complementary tests like CRP.
When Ordered
Clinicians order an ESR test in the following circumstances:
- Suspected polymyalgia rheumatica (PMR) — bilateral aching of shoulders, hip girdle, or neck in patients over 50 years of age
- Suspected giant cell arteritis (GCA) or temporal arteritis — headache, jaw claudication, visual symptoms, or temporal artery tenderness
- Monitoring of rheumatoid arthritis or systemic lupus erythematosus (SLE) disease activity over time
- Evaluation of unexplained fever, weight loss, or constitutional symptoms where chronic inflammation or malignancy is suspected
- Suspected chronic infection, including tuberculosis, osteomyelitis, or infective endocarditis
- Multiple myeloma screening, where a markedly elevated ESR (>100 mm/hr) is a classic finding
- Evaluation of inflammatory bowel disease (Crohn's disease, ulcerative colitis) activity
- Monitoring temporal arteritis treatment response — ESR should normalize with adequate corticosteroid therapy
- Evaluation of unexplained fatigue and joint pain where occult inflammation needs to be confirmed or excluded
- Confirmation that inflammation is present before initiating disease-modifying therapies such as methotrexate or biologics
No fasting is required before an ESR blood draw. Results are not affected by recent meals, making it convenient for routine clinical use at any time of day.
Westergren Method
The Westergren method is the internationally standardized protocol for measuring ESR and is the reference technique endorsed by the International Council for Standardization in Haematology (ICSH):
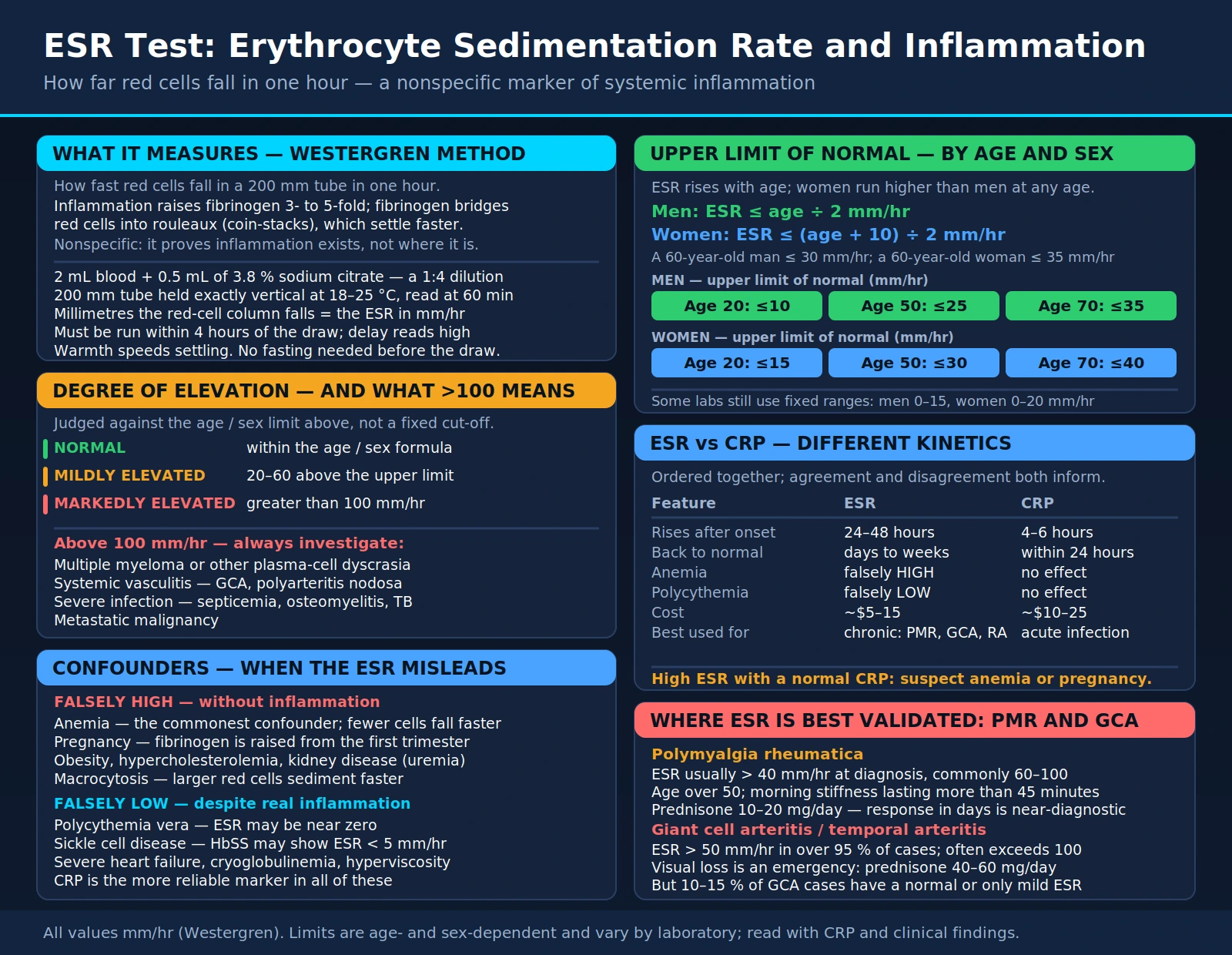
- Sample preparation: 2 mL of blood is mixed with 0.5 mL of 3.8% sodium citrate anticoagulant solution, producing a 1:4 dilution (blood:anticoagulant ratio of 4:1).
- Tube setup: The diluted blood is placed in a 200 mm Westergren glass (or plastic) tube held precisely vertical at room temperature (18–25°C).
- Reading: The distance in millimeters that the red cell column has fallen from its starting position is measured at exactly 60 minutes. This distance equals the ESR in mm/hr.
- Timing constraint: The test must be performed within 4 hours of collection. Delay causes falsely elevated results as RBCs begin to change shape and settle faster.
- Temperature sensitivity: Warmer temperatures accelerate sedimentation and produce falsely high results; the assay must be performed at controlled room temperature.
- Wintrobe method: An older alternative using undiluted blood in a shorter tube; less standardized, less commonly used, and not recommended for international comparison.
- Modern automated analyzers: Most clinical laboratories now use automated photometric or capillary analyzers that simulate the Westergren method with equivalent accuracy, faster turnaround, and reduced technician variability.
Because the method is simple and inexpensive, ESR can be performed in virtually any clinical laboratory worldwide, making it one of the most universally available inflammatory markers.
Normal Values by Age and Sex
ESR rises naturally with age, and women have inherently higher values than men at any given age. The most widely used formula for calculating the upper limit of normal was developed by Miller and colleagues:
- Men: ESR ≤ age ÷ 2 mm/hr (e.g., a 60-year-old man: upper limit ≤ 30 mm/hr)
- Women: ESR ≤ (age + 10) ÷ 2 mm/hr (e.g., a 60-year-old woman: upper limit ≤ 35 mm/hr)
ESR — Men (mm/hr) Upper limits of normal by age
ESR — Women (mm/hr) Upper limits of normal by age
ESR — Degree of Elevation (mm/hr, general interpretation)
Extreme elevation (>100 mm/hr) is clinically significant and strongly suggests one of the following: multiple myeloma or other plasma cell dyscrasia, systemic vasculitis (GCA, polyarteritis nodosa), severe systemic infection (septicemia, osteomyelitis, TB), or metastatic malignancy. A markedly elevated ESR should always prompt targeted investigation.
Some laboratories still use older fixed reference ranges (men: 0–15, women: 0–20 mm/hr) without age correction. Age-corrected interpretation using the Miller formula is clinically superior, especially in older patients where some elevation is physiologically normal.
Acute-Phase Proteins and Fibrinogen
The ESR is not a direct measure of inflammation itself — it is a physical consequence of changes in plasma protein composition that occur during inflammation. Understanding which proteins drive the ESR explains both its utility and its limitations.
Fibrinogen: the dominant driver. Fibrinogen is the plasma protein most responsible for rouleaux formation — the stacking of red blood cells like coins that causes them to settle rapidly. During acute and chronic inflammation, fibrinogen rises 3- to 5-fold above baseline. Fibrinogen acts as a bridging molecule between adjacent RBCs, overcoming the natural negative electrostatic charge that keeps them apart. More rouleaux = faster sedimentation = higher ESR.
Other positive acute-phase reactants that contribute to elevated ESR include:
- C-reactive protein (CRP): Synthesized by the liver in response to IL-6; rises within 4–6 hours of inflammation onset
- Serum amyloid A (SAA): An apolipoprotein that rises dramatically in acute inflammation; may reach 1,000-fold above baseline
- Alpha-1 antitrypsin: A protease inhibitor that rises 2–4-fold; protects tissues from neutrophil elastase during inflammation
- Complement proteins C3 and C4: Rise moderately during inflammation; part of innate immune activation
- Haptoglobin and ceruloplasmin: Bind free hemoglobin and copper respectively; rise 2–4-fold
Negative acute-phase reactants fall during inflammation — albumin, transferrin, and prealbumin decrease as the liver prioritizes synthesis of inflammatory proteins. Low albumin accompanying a high ESR reinforces the likelihood of significant systemic disease.
ESR lag: Because fibrinogen has a plasma half-life of approximately 4 days, the ESR rises slowly — it may not become clearly elevated until 24–48 hours after inflammation begins. Similarly, it falls slowly after inflammation resolves, sometimes taking weeks to normalize after an acute event. This makes ESR better for monitoring chronic, sustained inflammation (like PMR under steroid treatment) than for detecting acute events.
ESR vs CRP Comparison
ESR and CRP are both nonspecific markers of inflammation, but they respond to inflammation through different kinetics and are affected by different confounders. They are often ordered together, and their concordance or discordance is clinically informative.
| Feature | ESR | CRP |
|---|---|---|
| Rise after inflammation onset | 24–48 hours | 4–6 hours |
| Return to normal after resolution | Days to weeks | Within 24 hours |
| Specificity for inflammation | Lower (more confounders) | Higher (fewer confounders) |
| Affected by anemia | Yes — falsely elevated | No |
| Affected by polycythemia | Yes — falsely low | No |
| Affected by RBC shape abnormalities | Yes (sickle cell lowers ESR) | No |
| Best clinical use | Chronic monitoring (PMR, GCA, RA) | Acute infection, post-op monitoring |
| PMR/GCA primary monitoring tool | Yes | Complementary |
| Cost | Very low (~$5–15) | Low (~$10–25) |
| Availability | Universal | Universal |
When ESR and CRP are discordant, consider the following:
- High ESR, normal CRP: Suspect anemia (most common explanation), pregnancy, hypergammaglobulinemia, or early phase inflammation not yet reflected in CRP
- Normal ESR, high CRP: Suspect polycythemia, sickle cell disease, or other conditions that suppress ESR despite real inflammation; CRP is more reliable here
- Both elevated: Strong evidence of true systemic inflammation; warrants investigation
The combination of both tests provides more information than either alone. In PMR and GCA, both ESR and CRP are typically elevated at diagnosis, and both should normalize with adequate corticosteroid treatment — persistent elevation of either marker warrants evaluation for incomplete treatment response or relapse.
Polymyalgia Rheumatica and GCA
ESR is clinically central to the diagnosis and monitoring of two related inflammatory conditions: polymyalgia rheumatica (PMR) and giant cell arteritis (GCA, also called temporal arteritis). These are the conditions for which ESR has its best-validated diagnostic utility.
Polymyalgia Rheumatica (PMR)
- ESR is typically >40 mm/hr at diagnosis, and commonly >60–100 mm/hr
- Classic presentation: bilateral aching and stiffness of the shoulder girdle, hip girdle, and neck in patients over 50 years of age; morning stiffness lasting >45 minutes
- A dramatic symptomatic response to low-dose prednisone (10–20 mg/day) within days is nearly diagnostic — if there is no response, reconsider the diagnosis
- ESR is used to monitor disease activity during corticosteroid tapering; rising ESR during taper signals disease relapse
- CRP is typically elevated as well and is also used for monitoring
- PMR may occur concurrently with GCA in 40–50% of GCA patients
Giant Cell Arteritis (GCA) / Temporal Arteritis
- ESR >50 mm/hr is present in >95% of GCA cases at diagnosis; often exceeds 100 mm/hr
- Symptoms: new-onset headache (often temporal), temporal artery tenderness, jaw claudication (pain with chewing), scalp tenderness, diplopia, or sudden visual loss
- Visual loss from GCA is an emergency — irreversible ischemic optic neuropathy can occur; high-dose prednisone (40–60 mg/day or IV methylprednisolone for visual symptoms) must be started urgently, before biopsy results return
- Temporal artery biopsy remains the gold standard for diagnosis confirmation, but treatment should not be delayed pending biopsy
- ESR is the primary monitoring tool during treatment: normalization of ESR indicates adequate disease suppression; a rising ESR during steroid taper is the most sensitive predictor of relapse
- Important caveat: 10–15% of GCA patients have a normal or only mildly elevated ESR at presentation. A normal ESR does not exclude GCA if clinical suspicion is high — clinical assessment plus CRP and imaging (PET/CT, temporal artery ultrasound) should guide the decision.
Limitations and Confounders
Because ESR measures a physical property of blood (sedimentation rate) rather than a specific inflammatory molecule, it is susceptible to a variety of conditions that alter blood viscosity or red cell behavior independently of inflammation. Knowing these confounders prevents misinterpretation.
Causes of Falsely Elevated ESR (not from inflammation)
- Anemia: The most common confounder. Fewer red blood cells means less mutual hindrance to sedimentation — the remaining cells fall faster even without rouleaux formation. Any cause of anemia (iron deficiency, B12/folate deficiency, hemolysis) can elevate ESR independently of inflammation.
- Pregnancy: Physiologically elevated fibrinogen starting in the first trimester produces an elevated ESR throughout pregnancy and for several weeks postpartum.
- Female sex and older age: Both independently elevate ESR; the age/sex formulas correct for this physiological baseline elevation.
- Obesity: Adipose tissue produces inflammatory cytokines and increases fibrinogen, mildly elevating ESR even without active disease.
- Hypercholesterolemia: Elevated LDL and VLDL promote rouleaux formation, producing a mildly elevated ESR.
- Kidney disease: Uremia increases fibrinogen and other plasma proteins, elevating ESR.
- Macrocytosis: Larger RBCs sediment faster; macrocytic anemia (B12 or folate deficiency) can elevate ESR by two mechanisms simultaneously.
Causes of Falsely Low ESR Despite Inflammation
- Polycythemia vera: Markedly increased red cell mass creates mutual interference between cells, preventing rouleaux formation. ESR may be near zero even in the presence of significant inflammation or other disease. CRP is more reliable in polycythemia.
- Sickle cell disease and other RBC shape abnormalities: Irregular-shaped cells cannot stack into rouleaux, producing a falsely low ESR. Hemoglobin SS disease may show ESR <5 mm/hr regardless of inflammatory status.
- Severe congestive heart failure: Thought to relate to increased plasma viscosity limiting sedimentation; the mechanism is incompletely understood.
- Cryoglobulinemia: Abnormal proteins that precipitate at cold temperatures can interfere with the assay if the sample is processed at lower-than-standard room temperature.
- Hyperviscosity states: Including Waldenström's macroglobulinemia with very high IgM levels — paradoxically, extreme hyperviscosity can impede sedimentation.
What ESR Cannot Do
- Monitor acute infections: ESR rises too slowly (24–48 hour lag) to be useful for tracking rapid changes in acute infection. CRP or procalcitonin are superior for this purpose.
- Diagnose fibromyalgia: A normal ESR is actually part of the diagnostic criteria for fibromyalgia — inflammation is absent by definition. An elevated ESR in a patient suspected of having fibromyalgia should prompt reconsideration of the diagnosis.
- Distinguish between specific rheumatic diseases: ESR is elevated in RA, SLE, vasculitis, myositis, and many other conditions. It cannot discriminate between them; disease-specific antibodies and clinical context are required.
References
The following PubMed searches retrieve current research on ESR and inflammation:
- Erythrocyte sedimentation rate ESR clinical use — PubMed
- Westergren method ESR standardization — PubMed
- ESR CRP comparison inflammation markers — PubMed
- Fibrinogen acute phase reactant inflammation — PubMed
- Polymyalgia rheumatica ESR diagnosis — PubMed
- Giant cell arteritis ESR temporal artery — PubMed
- ESR normal values age sex formula — PubMed
- ESR anemia polycythemia confounders — PubMed
- Multiple myeloma elevated ESR — PubMed
- ESR rheumatoid arthritis monitoring — PubMed
- ESR tuberculosis osteomyelitis infection — PubMed
- Inflammatory bowel disease ESR CRP — PubMed
Connections
- All Lab Tests
- Inflammatory Markers
- ANA Test
- hs-CRP (High-Sensitivity CRP)
- Polymyalgia Rheumatica
- Temporal Arteritis / GCA
- Rheumatoid Arthritis
- Multiple Myeloma
- Lupus (SLE)
- Complete Blood Count (CBC)
- Ferritin Test
- Iron Panel
- Comprehensive Metabolic Panel
- Homocysteine
- Vitamin B12 Test