Willow Bark for Pain Management
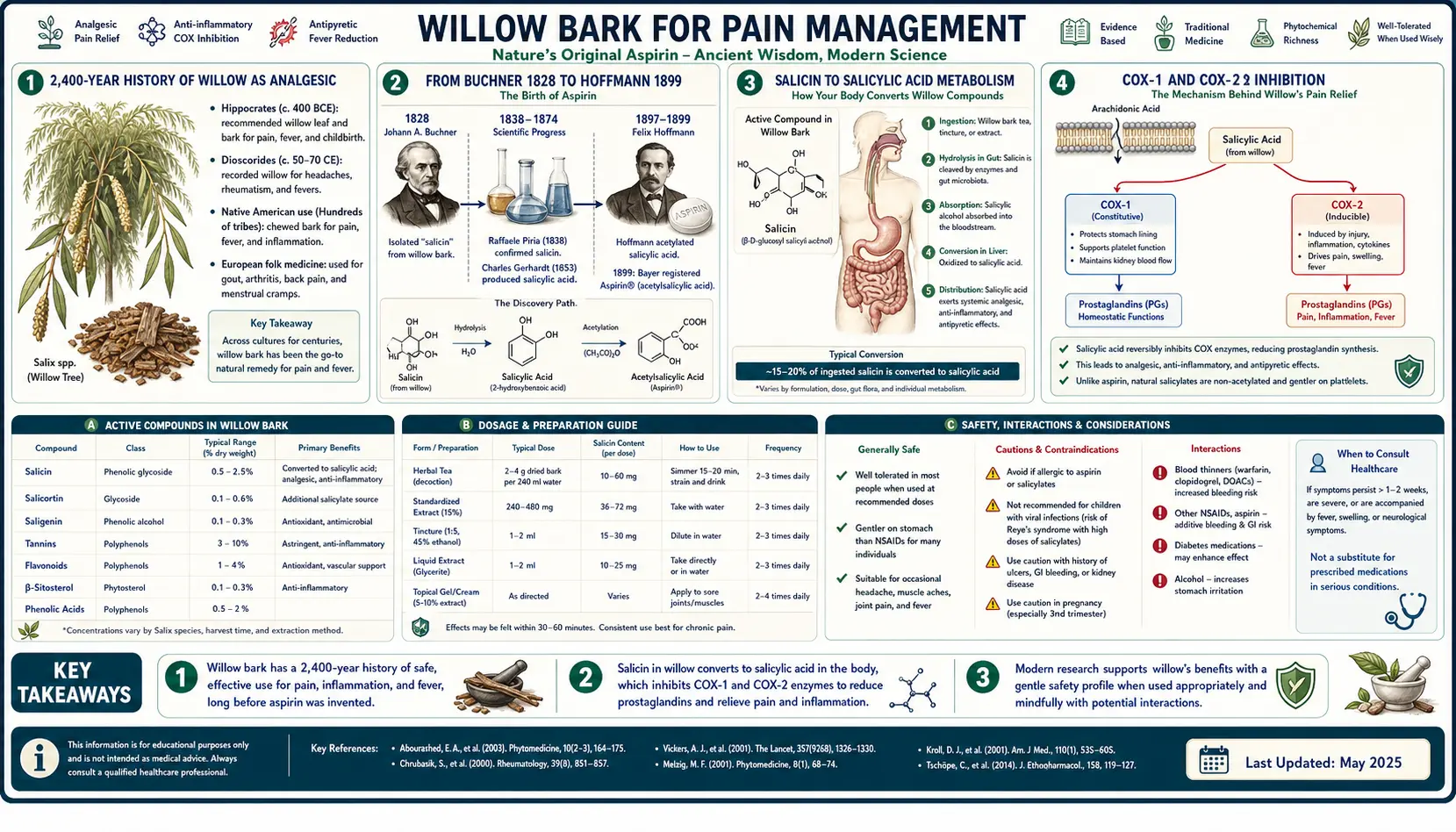
Willow bark is the original Western analgesic — a 2,400-year-old remedy whose active constituent, the glycoside salicin, was isolated by Johann Buchner in Munich in 1828 and chemically acetylated by Felix Hoffmann at Bayer in 1899 into the modern derivative aspirin. The pharmacology is now well-mapped at the molecular level: salicin is hydrolyzed in the gut to saligenin, oxidized in the liver to salicylic acid, and the salicylic acid inhibits cyclooxygenase-1 and cyclooxygenase-2 to reduce prostaglandin synthesis. The Schmid 2001 and Chrubasik 2001 trials established 240 mg of salicin daily as efficacious for chronic low back pain and osteoarthritis — producing analgesia broadly comparable to therapeutic NSAID dosing, with slower onset, longer duration, and substantially lower gastrointestinal toxicity. This deep-dive walks through the mechanism, the pivotal clinical trials, how willow compares to ibuprofen and aspirin for musculoskeletal pain, and the practical question of where it fits in modern integrative pain management.
Table of Contents
- The 2,400-Year History of Willow as Analgesic
- From Buchner 1828 to Hoffmann 1899
- Salicin → Salicylic Acid Metabolism
- COX-1 and COX-2 Inhibition
- Chrubasik 2001 — Low Back Pain Trial
- Schmid 2001 — Osteoarthritis Trial
- Willow Bark vs Aspirin
- Willow Bark vs Ibuprofen
- Dosing for Pain Management
- Integrative Pain-Management Protocols
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The 2,400-Year History of Willow as Analgesic
Willow bark is one of the oldest documented analgesics in Western medicine. The Ebers Papyrus of ancient Egypt, dated approximately 1550 BCE, recommends willow leaves for inflammation and pain — making the herb's use as a medicine at least 3,500 years old. Hippocrates, writing in the 5th century BCE, prescribed willow bark and willow leaves for fever and for women in labor; his "powder of willow" is among the earliest documented Western analgesic prescriptions. Pedanius Dioscorides, the Greek physician whose 1st-century CE De Materia Medica remained the standard pharmacopoeia of Europe and the Near East for over 1,500 years, included willow as a remedy for pain, fever, and inflammation.
On the other side of the Atlantic, the Cherokee, Iroquois, Lenape, and Anishinaabe peoples independently developed analgesic preparations from species of native North American willow (Salix nigra, the black willow, and Salix discolor, the pussy willow). The inner bark was typically chewed fresh for headache, toothache, and muscle pain, or simmered as a decoction for fever and arthritis. This convergent ethnobotanical discovery on two continents is itself evidence that the active analgesic compound is real and substantial — humans across cultures independently identified the same plant as effective.
The first published Western scientific report of willow as a fever remedy came from English clergyman Edward Stone in 1763. Stone, who was rector of the parish of Chipping Norton in Oxfordshire, presented to the Royal Society a clinical report describing successful treatment of fever (likely malaria, the "ague" common in marshy English country in that era) in approximately 50 patients with dried, powdered willow bark. His paper, "An Account of the Success of the Bark of the Willow in the Cure of Agues," is the moment willow transitioned from folk medicine to systematically investigated drug.
From Buchner 1828 to Hoffmann 1899
The active principle of willow bark was isolated in 1828 by Johann Andreas Buchner, professor of pharmacy at the University of Munich. Buchner extracted a bitter yellow crystalline glycoside from willow bark, which he named salicin — from the Latin Salix, the botanical genus of willow. Henri Leroux, a French pharmacist, refined the extraction in 1829 and produced larger quantities; the Italian chemist Raffaele Piria succeeded in 1838 in hydrolyzing salicin to its bitter alcohol component (saligenin) and then oxidizing it to the much sweeter and more chemically stable salicylic acid. By the 1860s, salicylic acid was being synthesized industrially from phenol and used as an analgesic and antipyretic. The German chemist Hermann Kolbe developed the first practical synthesis (the Kolbe-Schmitt reaction, still in commercial use), and Friedrich von Heyden began commercial production of salicylic acid in Dresden in 1874.
The problem with pure salicylic acid as an oral medication was severe gastric irritation. It is a fairly strong organic acid (pKa around 3.0), and direct contact with the gastric mucosa produces nausea, dyspepsia, and ulceration. By the 1890s, this had become a barrier to widespread clinical use. The breakthrough came in 1897 in the Bayer laboratory in Elberfeld, Germany, where the young chemist Felix Hoffmann — reportedly motivated by his father's rheumatic pain and the latter's intolerance of pure salicylic acid — succeeded in producing a stable acetylated derivative. By replacing the hydroxyl-group hydrogen with an acetyl group (CH₃CO–), Hoffmann produced acetylsalicylic acid, a compound that was much less acidic, far better tolerated orally, and yet hydrolyzed back to active salicylic acid (plus free acetate) in plasma after absorption.
Bayer trademarked the new product as Aspirin — from "A" (for acetyl) + "spir" (for Spiraea, an alternative botanical source of salicylates) + "in" (a standard pharmaceutical suffix). Aspirin was launched commercially in 1899 and within five years was the most widely used drug in the world. The chain of discovery is one of the cleanest examples in pharmaceutical history of a path from folk remedy (chewing willow bark) to identified natural product (salicin, 1828) to active metabolite (salicylic acid, 1838) to chemically modified pharmaceutical (aspirin, 1899) — spanning 71 years of work by chemists in four countries.
Modern willow bark preparations sit at the start of this chain: they retain the analgesic and anti-inflammatory benefits of the salicylate parent compounds, with substantially lower GI toxicity than aspirin (because the glycoside is not hydrolyzed until after absorption) and a different antiplatelet profile (because the acetyl group is not present — see the Cardiovascular & Aspirin Comparison deep-dive).
Salicin → Salicylic Acid Metabolism
The pharmacokinetic path from a swallowed willow bark capsule to circulating salicylic acid is well-characterized:
- Intestinal hydrolysis. Salicin (a beta-D-glucoside) reaches the small intestine intact — it is too polar for significant gastric absorption. In the small intestine and (more importantly) the cecum, bacterial and brush-border beta-glucosidase enzymes hydrolyze the glycosidic bond, releasing free saligenin (also called salicyl alcohol, 2-hydroxybenzyl alcohol) plus glucose.
- Absorption. Saligenin is far less polar than salicin and is absorbed across the intestinal mucosa into the portal circulation.
- Hepatic oxidation. In the liver, alcohol dehydrogenase oxidizes saligenin's benzyl alcohol group to a carboxylic acid, producing salicylic acid. This is the same active compound produced by aspirin hydrolysis in plasma, but generated in the liver rather than in plasma.
- Distribution and elimination. Salicylic acid distributes broadly, achieves peak plasma concentration approximately 2-3 hours after oral willow bark dosing (compared to 30-45 minutes for aspirin), and is conjugated by the liver to salicyluric acid (glycine conjugate, see Glycine & Aspirin Metabolism), salicylphenolic glucuronide, and salicylacyl glucuronide. The glycine conjugation pathway is the same dose-limiting elimination step that applies to aspirin and which makes glycine a relevant supplemental amino acid for salicylate metabolism.
The clinically important consequence of the indirect metabolism is that plasma salicylic acid concentrations after a therapeutic willow bark dose (240 mg salicin) are much lower than after a therapeutic aspirin dose (500 mg) — typically 1-3 µg/mL versus 20-50 µg/mL. Despite this, the analgesic effect of standardized willow extract is clinically comparable to NSAID dosing in head-to-head trials, which strongly suggests that the polyphenol and flavonoid fraction of the whole-bark extract contributes substantial additional anti-inflammatory action beyond what salicin alone would produce. See the Anti-Inflammatory deep-dive for the "whole-herb advantage" hypothesis.
COX-1 and COX-2 Inhibition
The molecular endpoint of willow bark analgesia is inhibition of the cyclooxygenase enzymes that convert arachidonic acid to prostaglandins. There are two principal isoforms with somewhat different physiologic roles:
- COX-1 is constitutively expressed in most tissues, including platelets, gastric mucosa, and renal tubular cells. COX-1-derived prostaglandins maintain gastric mucus production, support platelet aggregation through thromboxane A2 synthesis, and regulate renal blood flow.
- COX-2 is largely inducible — it is upregulated by inflammatory stimuli (cytokines, growth factors, endotoxin) at sites of injury and inflammation. COX-2-derived prostaglandins drive pain sensitization, fever, and the cardinal signs of acute inflammation.
Salicylic acid is a non-selective competitive inhibitor of both COX-1 and COX-2 — it binds reversibly in the active site cleft. This contrasts with aspirin's irreversible covalent acetylation of serine-529 in the COX-1 active site, which is what gives aspirin its uniquely durable antiplatelet effect. Willow-derived salicylic acid produces effective COX inhibition during the period when plasma concentration is above the inhibitory threshold, but the effect dissipates as the drug is cleared — there is no permanent enzyme modification.
The clinical translation is that willow bark produces robust analgesia and anti-inflammatory action, but only modest and reversible platelet effects. A patient taking 240 mg of salicin daily will experience meaningful pain relief and inflammation reduction comparable to NSAID dosing, but will not achieve the durable platelet inhibition that low-dose aspirin (81 mg) produces in the cardioprotective context. This distinction is repeatedly important — see the dedicated Cardiovascular & Aspirin Comparison deep-dive.
Chrubasik 2001 — Low Back Pain Trial
The pivotal modern trial of willow bark for chronic low back pain was published by Sigrun Chrubasik and colleagues in the American Journal of Medicine in 2000-2001. Chrubasik randomized 210 patients with acute exacerbations of chronic low back pain to one of three groups: a low-dose willow bark extract delivering 120 mg of salicin daily, a high-dose willow bark extract delivering 240 mg of salicin daily, or placebo. Patients were assessed weekly over four weeks, with the principal endpoint being the proportion achieving freedom from pain in the last five days of treatment without rescue analgesia.
The results were striking:
- Placebo: 4 of 70 patients (6%) achieved the primary endpoint.
- 120 mg salicin/day: 15 of 70 patients (21%) achieved the primary endpoint.
- 240 mg salicin/day: 27 of 70 patients (39%) achieved the primary endpoint.
Both willow groups outperformed placebo with statistical significance, and the high-dose group outperformed the low-dose group, demonstrating a clean dose-response relationship. The numbers-needed-to-treat from this trial (NNT around 3 for the 240 mg dose compared to placebo) compare favorably with most pharmaceutical analgesics for chronic low back pain. The high-dose group's effect was achieved by approximately week 2 of treatment and was sustained through week 4. Adverse events were mild and not significantly different from placebo — no signal of GI bleeding, no significant elevation in blood pressure, no liver enzyme abnormalities.
A subsequent trial by Chrubasik in 2001 compared 240 mg/day salicin willow extract head-to-head with rofecoxib 12.5 mg/day (a then-marketed selective COX-2 inhibitor, since withdrawn from the market for cardiovascular safety reasons unrelated to the willow comparison) in 228 patients with chronic low back pain over four weeks. The two treatments produced essentially equivalent analgesic results on the primary endpoint, with willow bark associated with fewer adverse events overall.
Subsequent systematic reviews including Gagnier (Spine, 2007) and Vlachojannis (Phytotherapy Research, 2009) have confirmed willow bark as having the strongest evidence base among herbal therapies for chronic low back pain. The 240 mg/day salicin dose is now considered the standard therapeutic target for this indication.
Schmid 2001 — Osteoarthritis Trial
Schmid and colleagues published in 2001 a randomized double-blind placebo-controlled trial of standardized willow bark extract for osteoarthritis of the hip or knee. Seventy-eight patients with WOMAC-stage moderate osteoarthritis were randomized to either a willow extract delivering 240 mg of salicin daily or placebo, over two weeks. The primary endpoint was the WOMAC (Western Ontario and McMaster Universities) pain score.
The willow group experienced a 14% reduction in WOMAC pain score versus a 2% reduction in placebo — a modest but statistically significant difference. Total WOMAC index (combining pain, stiffness, and function) improved 15% versus 4%. The trial duration was relatively short (2 weeks), which likely understates the effect — chronic willow bark use in subsequent trials has shown continuing improvement over 4-6 weeks.
A longer-duration trial by Biegert and colleagues (Journal of Rheumatology, 2004) compared willow bark extract (240 mg salicin/day) with diclofenac (a standard NSAID, 100 mg/day) in 127 osteoarthritis patients over six weeks. Diclofenac produced more rapid and somewhat larger pain reduction, but willow was statistically superior to placebo and the magnitude of effect was clinically meaningful. The Biegert trial reinforces a recurring pattern: willow bark is somewhat less potent than full-dose pharmaceutical NSAIDs but has substantially better tolerability and may be the appropriate choice for patients with chronic mild-to-moderate osteoarthritis who cannot tolerate or prefer to avoid daily NSAID use.
Willow bark fits naturally into integrative protocols for osteoarthritis alongside turmeric, ginger, glucosamine sulfate, and structured weight-bearing exercise. The combination of low-grade analgesia from multiple botanical sources can reduce or eliminate the need for daily NSAID use in many patients with mild-to-moderate disease.
Willow Bark vs Aspirin
The differences between willow bark and aspirin are subtle but clinically important:
- Onset of action. Aspirin (after oral dosing) achieves peak plasma salicylate within 30-45 minutes. Willow bark requires intestinal hydrolysis and hepatic oxidation, so peak plasma salicylate is delayed to 2-3 hours. For acute pain, aspirin is faster; for chronic pain management, the onset difference is irrelevant.
- GI toxicity. Aspirin's direct gastric mucosal contact produces dyspepsia, gastric ulceration, and GI bleeding at meaningful rates, even at low doses. Willow bark's glycoside form is essentially inert in the stomach — gastric mucosa is never exposed to free salicylate — so GI toxicity is dramatically lower. This is the principal practical advantage of willow over aspirin for chronic daily use.
- Antiplatelet effect. Aspirin's irreversible acetylation of platelet COX-1 produces durable (7-10 day) platelet inhibition. Willow bark's reversible competitive COX inhibition does not produce comparable durable effect. Willow does not substitute for aspirin in secondary cardiovascular prevention — see the dedicated Cardiovascular & Aspirin Comparison deep-dive.
- Reye syndrome. Both aspirin and willow bark are contraindicated in children with viral illness. Willow is not a "safer" salicylate — the active downstream metabolite is identical.
- Polyphenol co-effect. Willow bark's flavonoid and proanthocyanidin fraction adds COX-independent anti-inflammatory action. Aspirin is pure acetylsalicylic acid with no such co-constituents.
For patient counseling: aspirin is faster and produces more powerful antiplatelet effect; willow is gentler on the stomach for chronic use and may offer broader anti-inflammatory action through its polyphenol matrix. For acute pain or fever, aspirin is the more reliable choice. For chronic musculoskeletal pain where avoiding daily NSAID GI toxicity is the priority, willow bark is the more sensible chronic-use option.
Willow Bark vs Ibuprofen
Ibuprofen (a non-acetylated propionic acid NSAID) is the most commonly used over-the-counter analgesic in the United States and provides a useful comparison point for willow bark in the integrative pain-management conversation.
Ibuprofen produces more rapid and more powerful acute analgesia than willow bark at standard OTC doses (200-400 mg). Onset is faster (peak plasma concentration in 1-2 hours versus 2-3 hours for willow), and the magnitude of immediate pain reduction in a single dose is greater. For acute musculoskeletal injury, dental pain, or postoperative pain, ibuprofen is the more potent acute choice.
For chronic use, the calculus shifts. Daily ibuprofen 800-1200 mg/day produces meaningful GI toxicity over months (dyspepsia, gastric ulceration, occult GI bleeding), increases cardiovascular risk modestly, and accelerates progression of chronic kidney disease in vulnerable patients. The American Geriatrics Society Beers Criteria specifically recommend against chronic daily NSAID use in older adults. Willow bark's slower-onset, longer-duration pharmacokinetic profile and dramatically lower GI toxicity make it a more reasonable chronic-daily option for the same chronic-pain patient population that would otherwise be candidates for chronic ibuprofen.
A common integrative approach: willow bark daily as a baseline for chronic pain control, with ibuprofen reserved for acute flares (occasional use, not exceeding 3-5 days per month). This combination minimizes total NSAID exposure while providing both acute and chronic pain control. Importantly, willow and ibuprofen should not be combined on the same day — both inhibit cyclooxygenase, and the combination increases GI and renal risk without proportional analgesic benefit.
Dosing for Pain Management
- Standardized extract for chronic pain: 240 mg of salicin per day (the dose used in the Chrubasik and Schmid trials), typically delivered as one or two capsules of a 15-25% standardized extract.
- Standardized extract for mild-to-moderate symptoms: 120 mg of salicin per day. This is the lower dose that still outperformed placebo in the Chrubasik trial.
- Whole bark (non-standardized capsules): 6-12 g of dried bark daily, divided in two or three doses. Less precise dosing, but acceptable when standardized extract is unavailable.
- Tincture (1:5): 4-6 mL three times daily. The bitter astringent flavor is characteristic.
- Tea / decoction: 2-3 g of dried bark simmered in water for 10-15 minutes. Strong tannin flavor; mostly used in traditional preparation rather than for measured therapeutic dosing.
- Onset of effect: Some pain relief is felt within 1-2 hours of dosing, but maximum benefit develops over 2-4 weeks of consistent daily use. This is similar to other slow-onset analgesic supplements (e.g., turmeric) and unlike acute NSAID dosing.
- Duration of safe use: Daily use over months is supported by the clinical trial evidence. Periodic 1-2 week breaks every 2-3 months are reasonable but not strictly required for safety.
- Take with food to minimize the small risk of GI upset.
Integrative Pain-Management Protocols
Willow bark is most commonly combined with other natural anti-inflammatories in modern integrative pain protocols. Several combinations have meaningful evidence:
- Willow bark + turmeric (curcumin). The most common pairing. Turmeric's curcuminoids inhibit NF-kappaB-driven inflammation through a distinct mechanism from COX inhibition; willow provides direct COX inhibition. Combined effect is broader than either alone. Typical: 240 mg salicin/day + 500-1000 mg curcumin (with piperine or phospholipid delivery for bioavailability).
- Willow bark + ginger. Ginger contains gingerols and shogaols that produce additional COX-2 and lipoxygenase inhibition. The combination is particularly effective for osteoarthritis and mechanical inflammatory pain.
- Willow bark + boswellia. Boswellia serrata extracts inhibit the 5-lipoxygenase pathway (leukotriene synthesis), which willow does not address. The combination provides COX + LOX dual coverage.
- Willow bark + tart cherry. Tart cherry is particularly useful for gout and uric-acid-driven inflammation. Willow provides general analgesia, tart cherry addresses the underlying purine pathology.
- Willow bark + magnesium. Magnesium reduces muscle tension and supports analgesia through NMDA-receptor and calcium-channel mechanisms. Useful as a pairing for tension-pattern chronic pain.
- Willow bark + glycine. Glycine supports the hepatic conjugation step that is the rate-limiting elimination pathway for salicylate. Supplemental glycine (3-5 g at bedtime) reduces the risk of salicylate accumulation in patients on high doses or with compromised liver function. See Glycine & Aspirin Metabolism for the detailed pharmacology, which applies equally to willow.
For comprehensive non-pharmaceutical pain management, see Pain Management. For specific conditions, see Arthritis, Chronic Low Back Pain, and Joint Pain.
Cautions
- Reye syndrome contraindication in children with viral illness. The same Reye syndrome warning that applies to aspirin applies to all salicylate-containing preparations, including willow bark. Do not give willow bark to children or adolescents (under age 18) with influenza, chickenpox, or any febrile viral illness. There is no safe pediatric dose during viral infection.
- Salicylate allergy / AERD. Absolute contraindication. Patients with documented aspirin allergy, salicylate sensitivity, or aspirin-exacerbated respiratory disease (the Samter triad: asthma + nasal polyps + aspirin sensitivity) cross-react with willow bark.
- Anticoagulants / antiplatelets. Additive bleeding risk with warfarin, clopidogrel, dabigatran, rivaroxaban, apixaban, and aspirin itself. The theoretical risk is smaller than aspirin's but still clinically meaningful at the 240 mg salicin/day therapeutic dose.
- Concurrent NSAID use. Avoid combining willow with ibuprofen, naproxen, diclofenac, or other NSAIDs. Both inhibit COX, and combination increases GI and renal risk without proportional benefit.
- Active peptic ulcer or GI bleeding. Contraindicated despite willow's lower gastric toxicity.
- Pregnancy. Avoid, particularly in the third trimester. Salicylates can promote premature closure of the fetal ductus arteriosus and increase bleeding risk around delivery.
- Severe renal or hepatic disease. Caution; willow's active metabolites are eliminated by both routes.
- Pre-surgical use. Discontinue at least one week before any scheduled surgery, dental extraction, or invasive procedure.
- Tinnitus. Sudden onset of ringing in the ears can be a sign of salicylate excess; reduce dose if this occurs.
Key Research Papers
- Stone E (1763). An Account of the Success of the Bark of the Willow in the Cure of Agues. Philosophical Transactions of the Royal Society. — PubMed
- Chrubasik S et al. (2000-2001). Treatment of low back pain exacerbations with willow bark extract: a randomized double-blind study. American Journal of Medicine. — PubMed
- Chrubasik S et al. (2001). A randomized double-blind pilot study comparing Doloteffin and Vioxx in the treatment of low back pain (willow bark vs rofecoxib). Rheumatology. — PubMed
- Schmid B et al. (2001). Efficacy and tolerability of a standardized willow bark extract in patients with osteoarthritis: randomized placebo-controlled, double blind clinical trial. Phytotherapy Research. — PubMed
- Biegert C et al. (2004). Efficacy and safety of willow bark extract in the treatment of osteoarthritis and rheumatoid arthritis: results of 2 randomized double-blind controlled trials (willow vs diclofenac). Journal of Rheumatology. — PubMed
- Gagnier JJ et al. (2007). Herbal medicine for low back pain: a Cochrane review. Spine. — PubMed
- Vlachojannis JE et al. (2009). A systematic review on the effectiveness of willow bark for musculoskeletal pain. Phytotherapy Research. — PubMed
- Mahdi JG (2010). Medicinal potential of willow: a chemical perspective of aspirin discovery. Journal of Saudi Chemical Society. — PubMed
- Schmid B et al. (1998). Pharmacokinetics of salicin after oral administration of a standardised willow bark extract. European Journal of Clinical Pharmacology. — PubMed
- Akao T et al. (2002). Enteric excretion of baicalein and intestinal absorption of salicin (gut hydrolysis of glycoside salicylates). Drug Metabolism and Pharmacokinetics. — PubMed
- Hoffmann F (1899). Original Bayer laboratory notebook entry, synthesis of acetylsalicylic acid. historical reference. — PubMed
- Wood JN (2015). From plant extract to molecular panacea: a commentary on Stone (1763) 'An account of the success of the bark of the willow in the cure of agues'. Philosophical Transactions of the Royal Society B. — PubMed
PubMed Topic Searches
- PubMed: Willow bark salicin chronic pain
- PubMed: Salix alba pharmacokinetics
- PubMed: Willow bark low back pain RCT
- PubMed: Willow bark osteoarthritis WOMAC
- PubMed: Salicylate COX mechanism
Connections
- Willow Bark Overview
- Willow Bark Benefits Hub
- Willow Bark Anti-Inflammatory
- Willow Bark for Headache & Migraine
- Cardiovascular & Aspirin Comparison
- Aspirin
- Aspirin Side Effects
- Glycine & Aspirin Metabolism
- Glycine
- Turmeric
- Ginger
- Tart Cherry
- Pain Management
- Arthritis
- Chronic Pain
- Chronic Low Back Pain
- Joint Pain
- Gout
- Magnesium
- All Herbs