Willow Bark Cardiovascular Effects and Aspirin Comparison
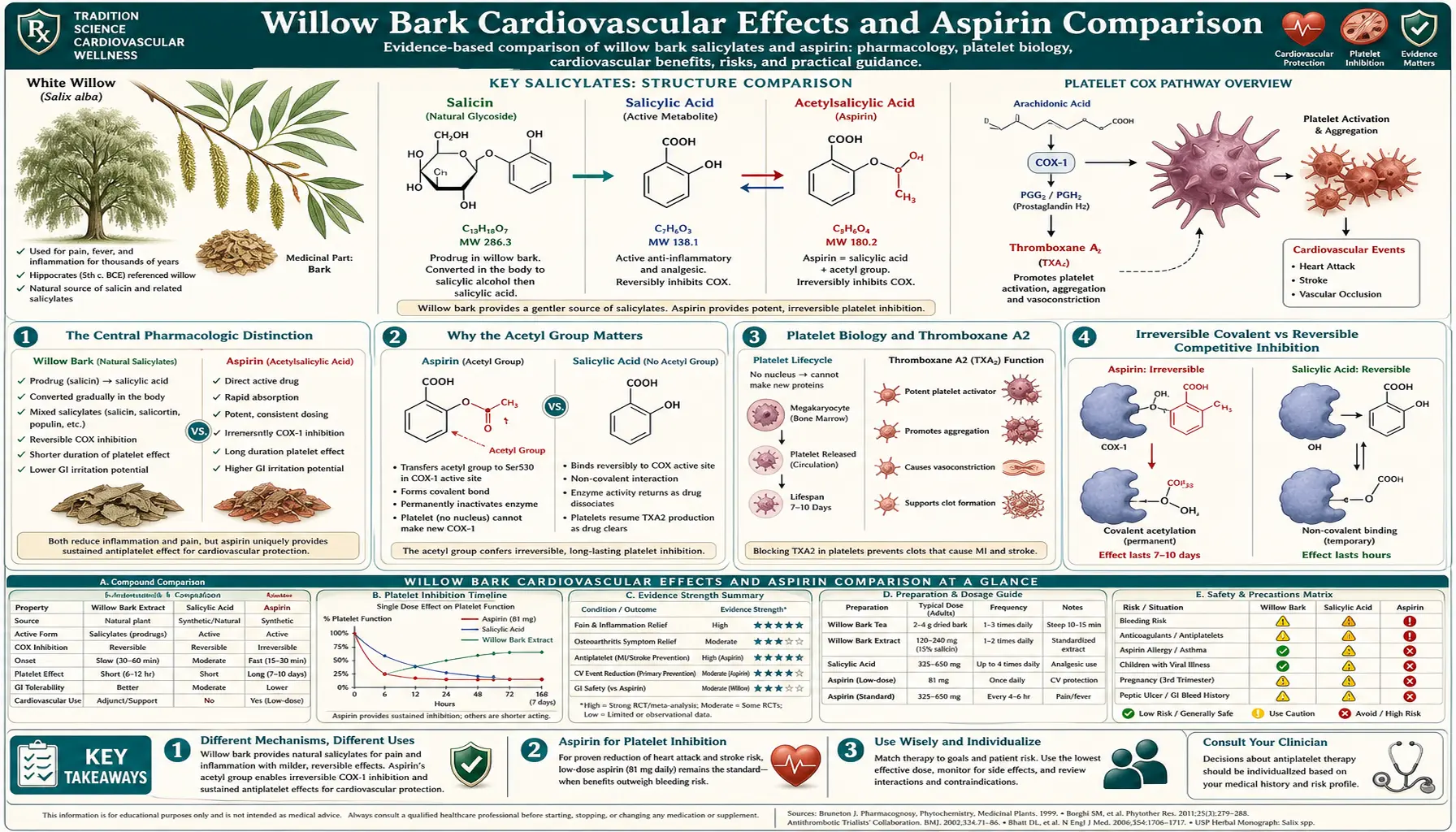
This is the most important clinical distinction in willow bark pharmacology, and it is consistently obscured in popular health writing: willow bark does NOT provide aspirin's antiplatelet cardioprotection. Aspirin's unique value in secondary prevention of myocardial infarction and stroke comes from its acetyl group covalently and irreversibly acetylating serine-529 on cyclooxygenase-1 in platelets, permanently disabling thromboxane A2 synthesis in those platelets for their 7-10 day lifespan. Salicin has no acetyl group. Salicylic acid produced from willow metabolism reversibly competes for the COX active site rather than covalently modifying it — effective for analgesia and anti-inflammatory effect, but inadequate for durable platelet inhibition. A patient taking low-dose aspirin (81 mg/day) for secondary cardiovascular prevention cannot substitute willow bark and maintain the same cardioprotective effect. This deep-dive walks through the acetylation pharmacology, the platelet biology, why aspirin is the only acetylated salicylate in clinical use, the secondary-prevention evidence base, and the appropriate (limited) cardiovascular role for willow bark.
Table of Contents
- The Central Pharmacologic Distinction
- Why the Acetyl Group Matters
- Platelet Biology and Thromboxane A2
- Irreversible Covalent vs Reversible Competitive Inhibition
- The Low-Dose Aspirin Cardioprotection Evidence
- What Willow Actually Does to Platelets
- Why Salicin Is Not an Aspirin Substitute
- Secondary Prevention: Aspirin Required, Willow Inadequate
- Primary Prevention: The Equation Has Shifted
- Limited Cardiovascular Applications for Willow
- Common Misconceptions to Avoid
- Key Research Papers
- Connections
- Featured Videos
The Central Pharmacologic Distinction
Walk into a typical health food store and ask about willow bark, and a common response is: "It's nature's aspirin — same thing, more natural." Read most popular health-website content on willow and you'll find similar language. The framing is not entirely wrong — willow bark and aspirin do share the same downstream active metabolite (salicylic acid) and the same principal mechanism of analgesic and anti-inflammatory action (cyclooxygenase inhibition). For pain management, anti-inflammatory effect, and fever reduction, willow bark is in fact a reasonable natural analog of aspirin with somewhat different pharmacokinetic and tolerability properties.
But for one specific indication — cardiovascular prophylaxis through platelet inhibition — the analogy breaks down completely. Aspirin's ability to prevent recurrent myocardial infarction and ischemic stroke depends on a pharmacologic property that willow bark does not share: the irreversible covalent acetylation of serine-529 on cyclooxygenase-1 in platelets, by the acetyl group that is specifically present in acetylsalicylic acid and absent from salicin or salicylic acid alone.
The clinical consequence is unambiguous: a patient who has had a previous myocardial infarction or ischemic stroke and is taking low-dose aspirin (81 mg daily) for secondary prevention CANNOT substitute willow bark and maintain the same cardioprotective effect. Willow bark does not durably inhibit platelet aggregation. It will not reduce the patient's risk of a second MI or recurrent stroke. Substituting willow for low-dose aspirin in a patient with established cardiovascular disease may meaningfully increase their cardiovascular event rate.
This is a frequent point of patient confusion. The purpose of this deep-dive is to walk through the pharmacology clearly enough that the distinction is understood and the substitution is not made inadvertently.
Why the Acetyl Group Matters
Aspirin's full chemical name is acetylsalicylic acid — the salicylic acid molecule with one of its hydroxyl-group hydrogens replaced by an acetyl group (CH₃CO–). That single chemical modification, made by Felix Hoffmann at Bayer in 1897, is what gives aspirin its unique cardiovascular properties.
The acetyl group can be transferred from acetylsalicylic acid to nucleophilic targets — in particular, the hydroxyl group of serine-529 in the active site of cyclooxygenase-1. When aspirin enters a platelet, the acetyl group is irreversibly transferred from acetylsalicylic acid to serine-529, leaving acetylated COX-1 plus free salicylic acid as the products. The acetylated serine-529 cannot participate in the COX-1 catalytic cycle — it permanently blocks the arachidonic acid substrate from reaching the heme-iron center where prostaglandin H2 is normally formed. The enzyme is permanently inactivated for the lifetime of that platelet.
Salicin (the willow bark glycoside) has no acetyl group available for transfer. Neither does salicylic acid, the downstream metabolite produced both from aspirin hydrolysis and from willow bark metabolism. Salicylic acid alone can occupy the COX-1 active site, blocking arachidonic acid binding, but it cannot covalently modify the enzyme. When the salicylic acid molecule dissociates from the active site (which it does reversibly, with a typical residence time of seconds-to-minutes), the enzyme returns to functional catalytic activity. There is no permanent inactivation.
This is the single most important pharmacologic distinction in the willow-versus-aspirin comparison. Aspirin is uniquely able to permanently modify platelet COX-1 because it carries an acetyl group. Willow bark, salicin, and salicylic acid alone all lack this acetyl group and cannot produce the equivalent durable effect on platelets.
Platelet Biology and Thromboxane A2
Platelets are anucleate cell fragments derived from megakaryocytes in the bone marrow. They lack a nucleus, so they cannot synthesize new mRNA or new proteins. The COX-1 enzyme that platelets express was synthesized in the megakaryocyte before the platelet was released into circulation, and it must last the platelet's entire lifespan (typically 7-10 days). When that COX-1 is irreversibly inactivated by aspirin acetylation, the platelet cannot generate new functional COX-1 to replace it — it is permanently disabled for thromboxane A2 synthesis until it is removed from circulation and replaced by a new platelet from the bone marrow.
Thromboxane A2 (TXA2), the principal COX-1 product in platelets, is a powerful vasoconstrictor and platelet aggregator. When a blood vessel is injured, activated platelets release thromboxane A2 into the local environment, which recruits additional platelets to the injury site and amplifies the aggregation response. This is essential for normal hemostasis (stopping bleeding), but the same mechanism contributes to pathological platelet aggregation in coronary artery disease, where atherosclerotic plaque rupture exposes pro-thrombotic surface that triggers platelet aggregation and arterial thrombus formation.
By irreversibly inactivating platelet COX-1, aspirin reduces thromboxane A2 production and shifts the platelet activation threshold higher. In the setting of atherosclerotic plaque rupture, this reduction in platelet aggregation translates to a reduction in arterial thrombus formation and a reduction in myocardial infarction or ischemic stroke risk.
The bone marrow produces approximately 10% of the total platelet pool per day (replacing the senescent platelets that are removed by the spleen). With chronic daily aspirin dosing, the bone marrow's new platelets enter a circulation environment where aspirin is still present, and they too become acetylated within hours of release. The result is sustained 90-95% suppression of platelet COX-1 activity with daily 81 mg aspirin dosing — the dose is sufficient to fully acetylate the newly released 10% of platelets each day while leaving extraplatelet COX-2 largely uninhibited.
This sustained platelet COX-1 inhibition is the mechanism behind aspirin's cardioprotection. Willow bark does not produce it.
Irreversible Covalent vs Reversible Competitive Inhibition
The distinction between irreversible covalent modification and reversible competitive inhibition is fundamental to understanding why aspirin uniquely produces durable platelet inhibition:
- Reversible competitive inhibition (the willow-salicylic-acid mechanism for COX). The inhibitor molecule occupies the enzyme's active site and prevents substrate binding, but it does not chemically modify the enzyme. When the inhibitor dissociates (which happens continuously based on the equilibrium binding constant), the enzyme returns to active form. Inhibition lasts only as long as the inhibitor remains in the active site, which depends on inhibitor concentration. Once the inhibitor is cleared from circulation, enzyme activity returns to normal within minutes.
- Irreversible covalent inhibition (the aspirin mechanism for platelet COX-1). The inhibitor molecule transfers a chemical group to the enzyme's active site, permanently modifying the enzyme. The enzyme cannot return to its original functional form even after the inhibitor is cleared from circulation. In a cell with active protein synthesis, the modified enzyme is eventually replaced by newly synthesized enzyme, restoring function. In platelets, which cannot synthesize new proteins, the modified enzyme remains modified for the platelet's lifetime.
Almost all clinically used drug-enzyme interactions are reversible competitive inhibition. The aspirin-platelet-COX-1 interaction is one of the few clinically important examples of irreversible covalent inhibition. The clinical implication: a single low-dose aspirin produces platelet inhibition lasting 7-10 days. A single dose of willow bark or any other reversible salicylate produces platelet inhibition lasting hours. There is no way to achieve aspirin's durable platelet effect with a reversible inhibitor — the irreversibility is the entire mechanism.
The Low-Dose Aspirin Cardioprotection Evidence
Low-dose aspirin's cardioprotective effect has been demonstrated in an enormous body of randomized clinical trial evidence. The key studies and consensus:
- ISIS-2 (1988) — 17,187 patients with acute myocardial infarction randomized to streptokinase, aspirin (160 mg), both, or neither. Aspirin alone reduced 5-week vascular mortality by 23%; aspirin plus streptokinase reduced mortality by 42%. This trial established aspirin as standard-of-care in acute MI management.
- ATC meta-analysis (Antithrombotic Trialists' Collaboration, 2002 and 2009) — pooled analysis of 287 randomized trials in over 200,000 patients confirmed that antiplatelet therapy (predominantly aspirin) reduced serious vascular events by approximately 25% in patients with established cardiovascular disease. The benefit was clearest in patients with prior MI, prior stroke, prior TIA, established coronary artery disease, or established peripheral arterial disease.
- Secondary prevention guidelines — ACC/AHA, ESC, NICE, and WHO guidelines all recommend low-dose aspirin (typically 75-100 mg daily) for secondary prevention in patients with established cardiovascular disease, unless contraindicated by bleeding history or active GI bleeding.
The mechanism is the durable platelet inhibition described above. Every randomized trial that has demonstrated aspirin's secondary prevention benefit has used acetylated salicylates — either aspirin itself or related acetylated derivatives. No randomized trial has ever demonstrated equivalent cardioprotection from non-acetylated salicylates (including willow bark, salicin alone, salicylic acid alone, or the sodium salicylate formulations historically used as anti-inflammatories before aspirin).
This is the strongest possible evidence-based argument that willow bark cannot substitute for aspirin in secondary cardiovascular prevention. The drug-class effect that produces the cardioprotection requires the acetyl group, and the entire trial evidence base used acetylated formulations.
What Willow Actually Does to Platelets
To be precise about willow bark's effect on platelets: it is not nothing. Several mechanisms produce mild reversible antiplatelet effect:
- Plasma salicylic acid from willow metabolism produces low-level reversible COX-1 inhibition in platelets while it is present, for the duration of measurable plasma concentration. After clearance, platelet function returns to normal.
- Polyphenol antiplatelet effects. Some willow polyphenols (catechins, proanthocyanidins) have mild antiplatelet activity, similar to that seen with green tea, dark chocolate, and red wine. The effect is real but small.
- Possible direct salicylate reversible inhibition. At sufficiently high plasma salicylic acid concentrations (not achieved at typical willow doses, but theoretically possible at supratherapeutic doses), reversible COX-1 inhibition could produce measurable platelet inhibition during peak plasma concentration.
The net effect: willow bark at therapeutic doses (240 mg salicin/day) produces approximately 10-20% reduction in platelet aggregation during peak plasma salicylate concentration, returning to baseline within 4-6 hours. By comparison, low-dose aspirin (81 mg/day) produces sustained 90-95% suppression of platelet thromboxane A2 production over 24 hours, every day.
The mild willow antiplatelet effect is enough to be clinically relevant for bleeding risk — willow bark should be discontinued before surgery, has additive bleeding risk with anticoagulants, and contributes to peri-procedural bleeding concerns — but it is far from sufficient to provide aspirin's secondary prevention cardioprotection.
Why Salicin Is Not an Aspirin Substitute
The simple summary:
- Aspirin = acetylsalicylic acid. The acetyl group covalently modifies platelet COX-1, producing irreversible enzyme inactivation lasting the platelet's 7-10 day lifespan.
- Willow bark salicin → salicylic acid. No acetyl group. Salicylic acid produces reversible competitive COX inhibition, lasting only while plasma concentration is sufficient.
You could in principle imagine taking pharmaceutical-grade salicin and chemically acetylating it — the resulting compound would actually be a synthetic acetylsalicin and would have somewhat different properties from aspirin (because of the glycoside attachment), but the more direct path is what Bayer's Felix Hoffmann did in 1897: take salicylic acid (the active downstream metabolite) and acetylate it, producing acetylsalicylic acid = aspirin. The acetylation step is what produces the irreversible platelet inhibition, regardless of whether you start with salicin or salicylic acid.
This is also why other naturally occurring salicylates — methyl salicylate (in wintergreen and birch), salicylate in meadowsweet, salicylate in poplar bark — all behave similarly to willow bark and similarly differently from aspirin. None of them are acetylated. None of them produce the durable platelet inhibition. The historical use of these natural sources for fever and pain is consistent across cultures and centuries, but their cardiovascular profile is fundamentally different from aspirin's.
Secondary Prevention: Aspirin Required, Willow Inadequate
For patients with established cardiovascular disease — previous myocardial infarction, previous ischemic stroke or TIA, established coronary artery disease (with prior PCI or CABG), established peripheral arterial disease, or stable angina — low-dose aspirin (75-100 mg daily) is a Class I recommendation in all major cardiovascular practice guidelines (ACC/AHA, ESC, NICE) unless contraindicated by active bleeding, salicylate allergy, or specific high-bleeding-risk circumstances.
The cardioprotective effect — approximately 25% reduction in serious vascular events in established CVD — is one of the most robust findings in cardiovascular medicine. The number-needed-to-treat (NNT) for secondary prevention is approximately 30 for the prevention of one serious vascular event over 5 years in the general post-MI population.
Willow bark does not produce this effect. A patient with established cardiovascular disease who replaces their low-dose aspirin with willow bark is removing the cardioprotective intervention without an effective substitute. The expected consequence is an increase in cardiovascular event rate proportional to the duration of aspirin discontinuation.
The practical clinical guidance:
- Do not substitute willow bark for aspirin in secondary cardiovascular prevention. This is the central message of this deep-dive.
- If GI tolerance of low-dose aspirin is poor, the appropriate alternative is enteric-coated aspirin (which delays gastric exposure), or aspirin combined with a proton pump inhibitor (which reduces gastric acid and ulcer risk), or under cardiology guidance, an alternative antiplatelet such as clopidogrel. Willow bark is not a valid substitute.
- If true aspirin allergy or major bleeding risk requires discontinuation, the alternative antiplatelet strategy should be developed in consultation with the patient's cardiologist. Willow bark plays no role in this decision.
- Willow bark can still be used for pain management or anti-inflammatory effect alongside low-dose aspirin in patients with established CVD — but with awareness that the additive bleeding risk needs to be balanced against analgesic benefit. Many cardiologists prefer acetaminophen as the pain-management adjunct for CVD patients on aspirin, to minimize the additive bleeding burden.
See Aspirin for comprehensive coverage of aspirin's cardiovascular indications and Aspirin Side Effects for the bleeding and GI considerations that complicate aspirin use.
Primary Prevention: The Equation Has Shifted
The role of aspirin in primary prevention — daily aspirin in patients without established cardiovascular disease, intended to prevent a first cardiovascular event — has shifted substantially in recent guidelines based on three large 2018 trials (ASPREE, ARRIVE, ASCEND). These trials showed that in low-to-moderate cardiovascular risk patients without established CVD, the bleeding risk of daily aspirin (approximately 1 major bleed per 200 patient-years) approximately balances or exceeds the cardiovascular event prevention benefit.
Current 2019 ACC/AHA guidelines and 2022 USPSTF recommendations reflect this:
- For most adults without established CVD, routine daily aspirin is no longer recommended for primary prevention.
- For adults aged 40-59 with elevated cardiovascular risk (10-year ASCVD risk ≥ 10%), aspirin may be considered after shared decision-making weighing benefit and bleeding risk.
- For adults aged 60 and older without established CVD, the USPSTF recommends against initiating aspirin for primary prevention.
For patients in the no-longer-aspirin primary-prevention category, willow bark is not an obvious substitute either — the rationale for using aspirin in primary prevention required aspirin's antiplatelet effect, and that effect is what current evidence does not support for low-risk patients. Willow bark for these patients would be primarily for anti-inflammatory or pain-management indications, not for cardiovascular protection.
The clinical principle: do not start willow bark with the expectation of cardiovascular protection. The evidence does not support primary cardiovascular benefit from willow bark, and the antiplatelet effect is insufficient to confer aspirin-like secondary prevention.
Limited Cardiovascular Applications for Willow
What cardiovascular-adjacent applications does willow bark legitimately have?
- Anti-inflammatory effect in atherosclerosis-relevant inflammation. Chronic systemic inflammation contributes to atherosclerosis progression. Willow bark's anti-inflammatory effect (COX inhibition + NF-kappaB / TNF-alpha suppression) may modestly reduce inflammatory markers like CRP and IL-6. This is theoretically beneficial for long-term atherosclerosis but has not been demonstrated to translate to cardiovascular event reduction in clinical trials. Treating elevated CRP without a specific anti-inflammatory cardiovascular indication is not standard of care.
- Pain management for cardiovascular patients with chronic musculoskeletal pain. Patients with CVD often need pain management for arthritis, chronic back pain, or post-procedural pain. Willow bark's gentler GI profile and the absence of significant cardiovascular-specific harm (no QT prolongation, no significant blood pressure effects, no congestive heart failure risk) make it a reasonable option in this population. Awareness of additive bleeding risk with concurrent aspirin or anticoagulant is required.
- Adjunctive blood pressure considerations. Unlike NSAIDs (which can raise blood pressure by 2-5 mmHg through renal prostaglandin effects and sodium retention), willow bark at therapeutic doses appears to have minimal effect on blood pressure. This may be preferable to NSAIDs in patients with hypertension. But this is not the same as having a blood pressure benefit.
The bottom line: willow bark is reasonable for pain management and anti-inflammatory effect in patients who happen to have cardiovascular disease, with attention to additive bleeding risk. Willow bark is not a cardiovascular prophylactic intervention and should not be marketed or used as one.
Common Misconceptions to Avoid
Common patient and consumer misconceptions about willow bark and cardiovascular protection:
- "Willow is just a natural form of aspirin, so I can use it instead of my low-dose aspirin." Incorrect. Willow lacks the acetyl group that produces aspirin's cardioprotective platelet inhibition. Substitution will reduce cardiovascular protection.
- "My doctor said to take a baby aspirin every day, but I prefer natural alternatives, so I take willow bark instead." If the doctor's recommendation is for secondary cardiovascular prevention, this substitution is medically inappropriate. The patient should discuss with the prescribing clinician.
- "Willow bark thins the blood like aspirin." Partially true but misleading. Willow has mild reversible antiplatelet effect at high doses, but does not produce sustained platelet inhibition. It is not equivalent to aspirin's "blood thinning" for cardiovascular indications.
- "Willow bark prevents heart attacks naturally." Not supported by evidence. No randomized trial has demonstrated willow bark cardiovascular event prevention.
- "Willow is safer than aspirin for the heart." Willow is not "safer for the heart" because it provides less cardioprotection — that's actually less safe for patients who need cardioprotection. Willow may be safer for the stomach, but not for the heart.
The clear messaging for patients:
- Willow bark is good for pain management and anti-inflammatory effect.
- Willow bark is gentler on the stomach than chronic aspirin.
- Willow bark is not a substitute for low-dose aspirin in cardiovascular protection.
- If you are taking low-dose aspirin for cardiovascular protection, continue it as prescribed.
- If you want to use willow bark for pain management while taking low-dose aspirin, discuss with your physician for additive bleeding risk monitoring.
Key Research Papers
- Roth GJ, Majerus PW (1975). The mechanism of the effect of aspirin on human platelets. I. Acetylation of a particulate fraction protein. Journal of Clinical Investigation. — PubMed
- Patrono C (1994). Aspirin as an antiplatelet drug. NEJM. — PubMed
- ISIS-2 Collaborative Group (1988). Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. Lancet. — PubMed
- Antithrombotic Trialists' Collaboration (2002). Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high-risk patients. BMJ. — PubMed
- Antithrombotic Trialists' Collaboration (2009). Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet. — PubMed
- Vane JR (1971). Inhibition of prostaglandin synthesis as a mechanism of action for aspirin-like drugs. Nature New Biology. — PubMed
- McNeil JJ et al. (2018). Effect of aspirin on disability-free survival in the healthy elderly (ASPREE trial). NEJM. — PubMed
- Gaziano JM et al. (2018). Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE trial). Lancet. — PubMed
- ASCEND Study Collaborative Group (2018). Effects of aspirin for primary prevention in persons with diabetes mellitus. NEJM. — PubMed
- Krasselt M, Baerwald C (2019). Sex, symptom severity, and quality of life in rheumatology (relevant to willow bark anti-inflammatory use in CVD patients). Clinical Reviews in Allergy and Immunology. — PubMed
- Shara M, Stohs SJ (2015). Efficacy and safety of white willow bark (Salix alba) extracts. Phytotherapy Research. — PubMed
- Krivoy N et al. (2001). Effect of salicis cortex extract on human platelet aggregation. Planta Medica. — PubMed
- Bjarnason I et al. (2018). Mechanisms of damage to the gastrointestinal tract from NSAIDs (relevant to aspirin GI toxicity). Gastroenterology. — PubMed
- USPSTF (2022). Aspirin use to prevent cardiovascular disease: US Preventive Services Task Force recommendation statement. JAMA. — PubMed
PubMed Topic Searches
- PubMed: Aspirin acetylation platelet COX-1
- PubMed: Non-acetylated salicylate platelet function
- PubMed: Low-dose aspirin secondary prevention
- PubMed: Willow bark platelet aggregation
- PubMed: Thromboxane A2 platelet
Connections
- Willow Bark Overview
- Willow Bark Benefits Hub
- Willow Bark for Pain Management
- Willow Bark Anti-Inflammatory
- Willow Bark for Headache & Migraine
- Aspirin
- Aspirin Health Benefits
- Aspirin Side Effects
- Glycine
- Glycine & Aspirin Metabolism
- Heart Disease
- Atherosclerosis
- Stroke
- Pain Management
- Turmeric
- Ginger
- Magnesium
- All Herbs