Willow Bark Anti-Inflammatory Action
A persistent puzzle in willow bark pharmacology is that clinical effect outstrips what pure salicin pharmacokinetics would predict. A standard 240 mg daily salicin dose produces plasma salicylic acid concentrations of only 1-3 µg/mL — roughly an order of magnitude below the 20-50 µg/mL produced by therapeutic aspirin — yet head-to-head trials show willow extract producing analgesia and anti-inflammatory effect comparable to NSAID dosing. The resolution is the whole-herb advantage hypothesis: willow bark contains a substantial polyphenol and flavonoid fraction (catechins, proanthocyanidins, salicortin, tremulacin, isosalipurposide, picein) that produces COX-independent anti-inflammatory action through inhibition of NF-kappaB, TNF-alpha, and prostaglandin E2 synthesis. The Setty & Sigal 2005 rheumatoid arthritis pilot and several in vitro studies of standardized willow extract compared to equimolar pure salicin confirm that the whole extract is meaningfully more anti-inflammatory than the salicin content alone. This deep-dive maps the polyphenol fraction, the COX-independent mechanisms, and the clinical relevance for chronic inflammatory conditions.
Table of Contents
- The Whole-Herb Pharmacology Puzzle
- The Polyphenol & Flavonoid Fraction
- COX-Independent Anti-Inflammatory Pathways
- NF-kappaB Inhibition
- TNF-alpha and Pro-Inflammatory Cytokine Suppression
- Prostaglandin E2 Synthesis Suppression
- Setty & Sigal 2005 Rheumatoid Arthritis Pilot
- The Whole-Herb Advantage Hypothesis
- Applications in Chronic Inflammatory Conditions
- Why Extract Standardization Matters
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The Whole-Herb Pharmacology Puzzle
If willow bark's analgesic and anti-inflammatory action came only from its salicin content acting through salicylic acid's cyclooxygenase inhibition, the clinical effect should be modest. A 240 mg daily salicin dose, fully converted to salicylic acid, produces peak plasma concentrations of approximately 1-3 micrograms per milliliter. By contrast, therapeutic aspirin dosing (500-1000 mg) produces plasma salicylate concentrations of 20-50 µg/mL, and anti-inflammatory aspirin dosing in rheumatoid arthritis (historically used at 3-6 grams daily) targeted 150-300 µg/mL. On a salicylic acid basis alone, willow bark should produce only a fraction of the anti-inflammatory effect of even a single aspirin tablet.
Yet head-to-head clinical trials repeatedly show willow bark producing analgesia comparable to therapeutic NSAID dosing. The Chrubasik 2001 trial showed 240 mg salicin/day matching rofecoxib 12.5 mg/day for low back pain. The Biegert 2004 trial showed 240 mg salicin/day producing meaningful pain reduction in osteoarthritis, with diclofenac as a more potent active comparator. Patients report subjective anti-inflammatory benefit that does not match the salicin-only pharmacokinetic prediction.
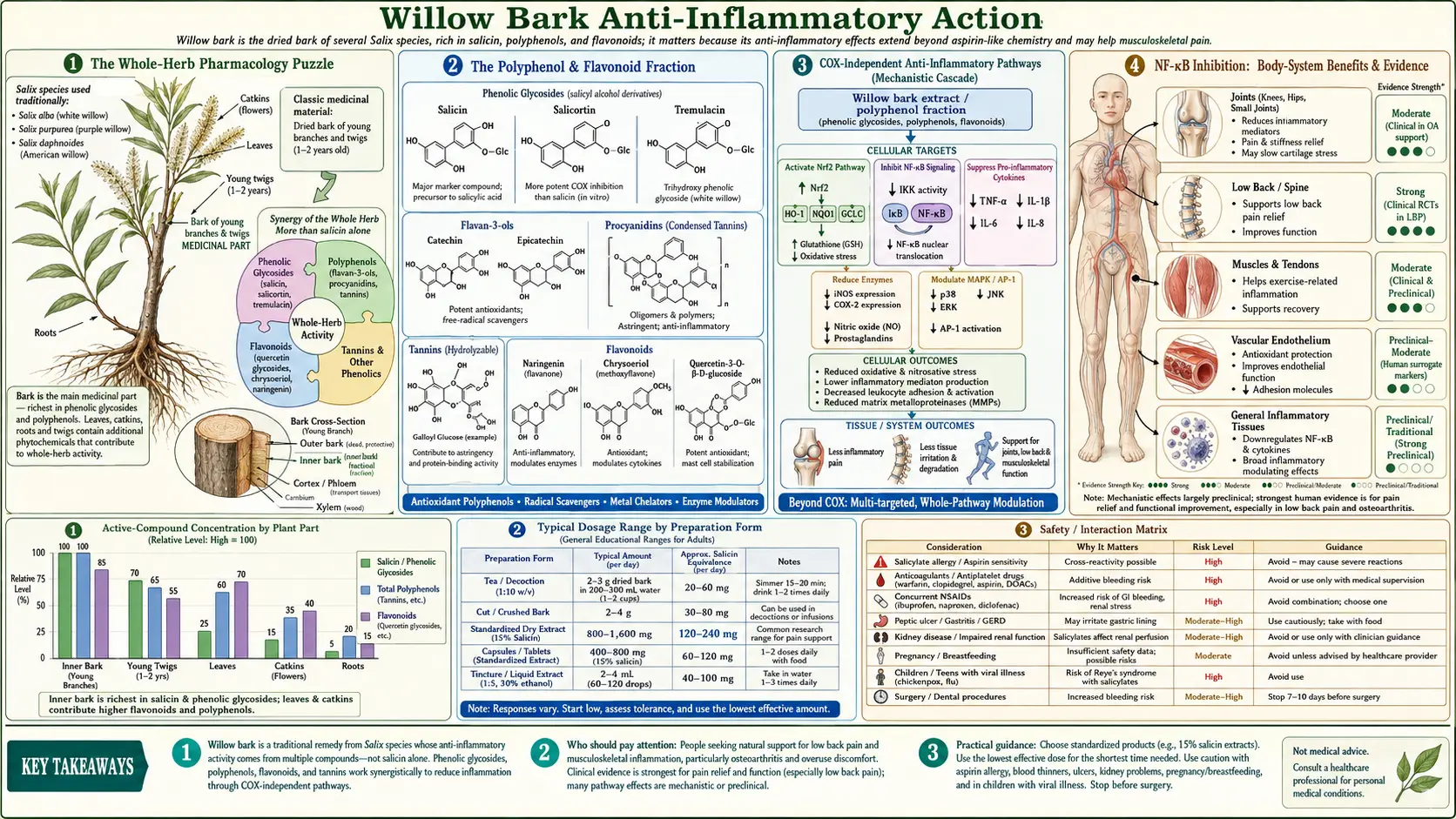
The resolution to the puzzle is that willow bark is not just a slow-release salicin delivery vehicle. The whole bark extract contains a substantial polyphenol and flavonoid fraction that produces independent anti-inflammatory action through cyclooxygenase-independent mechanisms. The total clinical effect is the sum of (1) salicin-derived salicylic acid producing modest COX inhibition plus (2) the polyphenol fraction producing additional NF-kappaB, TNF-alpha, and PGE2 suppression. This multi-component anti-inflammatory effect is the "whole-herb advantage" — the reason willow extract outperforms equimolar pure salicin in mechanistic and clinical endpoints.
The Polyphenol & Flavonoid Fraction
Standardized willow bark extracts contain at least four classes of secondary metabolites beyond salicin:
- Salicin-related glycosides — salicortin, tremulacin, picein, salireposide. These are structurally related to salicin and can themselves be hydrolyzed to release salicylic-acid-precursor moieties, contributing to the total salicylate pool.
- Catechins and proanthocyanidins — flavonoid polymers structurally similar to those in green tea, dark cocoa, and red wine. These contribute substantial antioxidant capacity and have well-documented anti-inflammatory action through NF-kappaB pathway inhibition.
- Flavonols and flavones — quercetin glycosides (isoquercitrin, rutin), kaempferol glycosides, and apigenin derivatives. Flavonols inhibit lipoxygenase, NF-kappaB, and several pro-inflammatory cytokines.
- Phenolic acids and tannins — gallic acid, ellagic acid, and condensed tannins. These contribute astringent properties (the characteristic mouthfeel of strong willow tea) and additional antioxidant capacity.
The polyphenol content of standardized willow extracts is substantial: total phenolic content typically 12-18% by mass, with total flavonoid content of 3-6%. By comparison, salicin content in the same standardized extracts is typically 15-25%. On a mass basis, polyphenols and flavonoids together are comparable to or larger than the salicin fraction — not a trace constituent, but a major component of the active extract.
The polyphenol fraction is also reasonably bioavailable. Catechins and flavonols are absorbed across the small intestine (partially as glycosides via SGLT1 and as aglycones after deconjugation), achieve plasma concentrations in the 0.1-1 µM range after dietary or extract dosing, and circulate as sulfate, glucuronide, and methylated conjugates that retain biological activity. The polyphenol fraction is not just a passive accompaniment to salicin — it reaches the systemic circulation and acts on the same molecular targets that drive chronic inflammation.
COX-Independent Anti-Inflammatory Pathways
The polyphenol fraction of willow bark produces anti-inflammatory action through mechanisms that do not involve the cyclooxygenase enzymes. The principal pathways are:
- NF-kappaB transcription factor inhibition. NF-kappaB is the master transcription factor regulating pro-inflammatory gene expression — it controls transcription of TNF-alpha, IL-1, IL-6, COX-2, iNOS, and dozens of other inflammatory mediators. Polyphenol inhibition of NF-kappaB activation produces broad reduction in inflammatory gene expression upstream of the prostaglandin pathway.
- TNF-alpha synthesis suppression. Multiple studies of standardized willow extract show suppression of TNF-alpha production from LPS-stimulated macrophages and monocytes. TNF-alpha is the central pro-inflammatory cytokine in rheumatoid arthritis, inflammatory bowel disease, psoriasis, and several other chronic inflammatory conditions.
- Lipoxygenase (LOX) inhibition. Flavonoids in willow extract inhibit 5-lipoxygenase, the enzyme that converts arachidonic acid to leukotrienes. Leukotrienes drive bronchoconstriction, vascular permeability, and neutrophil recruitment in asthma and chronic inflammation. This is a pathway aspirin does not address.
- Direct free radical scavenging. Polyphenols and tannins scavenge superoxide, hydroxyl radicals, and peroxyl radicals. This reduces oxidative damage to inflamed tissue and reduces the oxidant signaling that further amplifies NF-kappaB activation.
- Cell-adhesion molecule downregulation. Polyphenols reduce expression of ICAM-1, VCAM-1, and E-selectin on activated endothelium, reducing neutrophil and monocyte recruitment into inflamed tissue.
The combined effect of these pathways is broad anti-inflammatory action that suppresses inflammatory signaling at multiple steps — upstream of COX-2 induction (via NF-kappaB), in parallel to COX-2 (via 5-LOX), and downstream of mediator release (via cell-adhesion molecule blockade). Salicin-derived salicylic acid adds direct COX inhibition on top of this polyphenol-mediated framework.
NF-kappaB Inhibition
NF-kappaB (nuclear factor kappa-light-chain-enhancer of activated B cells) is the central transcription factor in pro-inflammatory gene expression. In the resting cell, NF-kappaB is sequestered in the cytoplasm bound to its inhibitor IkappaB. Inflammatory stimuli (TNF-alpha, IL-1, LPS, reactive oxygen species, T-cell receptor engagement) activate the IKK (IkappaB kinase) complex, which phosphorylates IkappaB and targets it for proteasomal degradation. Free NF-kappaB translocates to the nucleus and drives transcription of dozens of inflammatory genes.
Standardized willow bark extract inhibits NF-kappaB activation through multiple mechanisms documented in cell-culture studies:
- Suppression of IKK activity, reducing IkappaB phosphorylation
- Stabilization of IkappaB by interfering with its proteasomal degradation
- Direct interference with NF-kappaB DNA-binding activity in some studies
- Reduction in the expression of NF-kappaB target genes (COX-2, iNOS, TNF-alpha, IL-6) at the mRNA and protein level
This NF-kappaB suppression is a polyphenol effect — it is reproduced by isolated catechin, quercetin, and procyanidin fractions, and is not seen with pure salicin at comparable concentrations. The clinical translation is broad anti-inflammatory action upstream of any individual mediator, which explains why willow extract effects extend to conditions where pure aspirin would have limited utility (chronic autoimmune inflammation, gut inflammation, vascular inflammation).
TNF-alpha and Pro-Inflammatory Cytokine Suppression
TNF-alpha is the central pro-inflammatory cytokine in many chronic inflammatory diseases. The success of TNF-alpha-blocking biologics (infliximab, adalimumab, etanercept, certolizumab, golimumab) in rheumatoid arthritis, psoriasis, ankylosing spondylitis, and inflammatory bowel disease demonstrates how central TNF-alpha is to chronic inflammatory pathology. Anything that reduces TNF-alpha production produces broad anti-inflammatory benefit.
Standardized willow bark extract significantly suppresses TNF-alpha production in LPS-stimulated monocyte and macrophage cell-culture models, at concentrations achievable with oral dosing. The effect is dose-dependent and is partially attributable to NF-kappaB inhibition (since TNF-alpha is an NF-kappaB target gene) and partially to direct polyphenol effects on the TNF-alpha promoter.
The clinical relevance: patients with chronic conditions driven primarily by TNF-alpha-mediated inflammation (rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, Crohn's disease) may benefit from willow bark as adjunctive therapy alongside standard care. The magnitude of effect from any natural anti-inflammatory is much smaller than from biological TNF-alpha blockade, but the additive benefit from a well-tolerated daily herbal anti-inflammatory can be meaningful for symptom control between flares. This is one of the practical applications explored in the Setty & Sigal 2005 rheumatoid arthritis pilot.
Similar mechanistic effects on IL-1-beta and IL-6 have been documented in some studies, with willow extract reducing inflammatory cytokine production across the broader pattern, not just TNF-alpha alone.
Prostaglandin E2 Synthesis Suppression
Prostaglandin E2 (PGE2) is the dominant pro-inflammatory prostaglandin in mammalian tissue. It drives the cardinal signs of acute inflammation (heat, redness, swelling, pain), is the principal fever-inducing prostaglandin at the hypothalamus, and contributes to chronic inflammatory pain through peripheral nociceptor sensitization. PGE2 synthesis depends on both COX-1 (constitutive) and COX-2 (inducible) activity acting on arachidonic acid substrate.
Standardized willow bark extract suppresses PGE2 synthesis through three mechanisms operating in parallel:
- Direct COX inhibition by salicin-derived salicylic acid — the classical mechanism, accounting for some fraction of the total PGE2 suppression.
- Reduced COX-2 induction via NF-kappaB inhibition — polyphenol-mediated NF-kappaB suppression reduces the inflammatory upregulation of COX-2 expression, which is normally the dominant source of PGE2 in inflamed tissue. Less COX-2 enzyme means less PGE2 even if individual COX-2 molecules are not directly inhibited.
- Phospholipase A2 suppression — some polyphenol constituents of willow extract reduce activity of cytosolic phospholipase A2, the enzyme that releases arachidonic acid from membrane phospholipids. Less arachidonic acid substrate means less downstream prostaglandin synthesis regardless of COX activity.
The three-mechanism PGE2 suppression is meaningfully broader than aspirin's pure COX inhibition. This is part of why willow extract's analgesic effect is clinically larger than the modest plasma salicylate concentrations would predict — the polyphenol fraction reduces PGE2 production at the substrate (arachidonic acid release) and enzyme expression (COX-2 induction) levels, not just at the catalytic activity level.
Setty & Sigal 2005 Rheumatoid Arthritis Pilot
Aradhana R. Setty and Leonard H. Sigal published a comprehensive review in Seminars in Arthritis and Rheumatism in 2005 on herbal medications in rheumatology practice, with willow bark as one of the featured monographs. The review summarized then-available evidence including a small pilot study of standardized willow bark extract in rheumatoid arthritis.
The pilot data showed modest but statistically significant improvement in tender joint count, swollen joint count, and patient-reported pain in 26 RA patients on background DMARDs who added willow extract (240 mg salicin/day) for six weeks. The effect size was smaller than would be expected from full-dose NSAID addition, but the safety profile was excellent — no GI events, no liver enzyme elevation, no renal function changes, no significant medication interactions in this small sample. The authors concluded that willow bark warranted further study as an adjunctive anti-inflammatory in RA patients seeking to reduce or avoid daily NSAID use.
Subsequent larger trials of willow bark in rheumatoid arthritis have been limited, partly because the rheumatology field shifted heavily toward biologic DMARD therapy (TNF-alpha blockade, IL-6 blockade, JAK inhibitors) in the years after 2005, leaving less academic interest in herbal adjuncts. The clinical practice question, however, is real and recurring: many RA patients on biologic therapy still have residual inflammatory pain and stiffness between doses. A well-tolerated herbal anti-inflammatory like willow bark can fill that gap without the GI and renal liabilities of chronic NSAID use.
The Setty & Sigal pilot is best understood not as definitive evidence but as proof of concept: standardized willow bark produces measurable anti-inflammatory effect even in patients already on optimized standard care, and the safety profile supports chronic use. Patients should not substitute willow for DMARD or biologic therapy — the magnitude of effect is far smaller — but adjunctive use for residual symptoms is reasonable.
The Whole-Herb Advantage Hypothesis
The "whole-herb advantage" hypothesis proposes that standardized whole-plant extracts produce clinically larger effects than equimolar doses of their principal active constituent because of synergistic action of the co-constituents. The willow bark / salicin example is one of the cleanest demonstrations of this hypothesis in herbal medicine:
- Standardized willow extract delivering 240 mg/day salicin produces analgesia comparable to therapeutic NSAID dosing.
- Pure salicin alone at the same 240 mg/day dose produces much smaller analgesic effect in the limited pure-salicin studies that have been done.
- Pure salicylic acid at the calculated equivalent dose produces predictable but again smaller anti-inflammatory effect than willow extract.
The gap between (1) and (2)/(3) is the polyphenol contribution. The whole extract carries salicin plus catechins, proanthocyanidins, flavonols, and tannins; the polyphenol fraction adds NF-kappaB inhibition, TNF-alpha suppression, PGE2 substrate reduction, and direct antioxidant effects. The total clinical impact exceeds what salicin alone would predict because the inflammatory cascade has multiple intervention points and the extract addresses several simultaneously.
This is the central pharmacologic argument for using standardized willow bark extract rather than pure isolated salicin or pure salicylic acid (or aspirin) when the goal is chronic anti-inflammatory effect rather than acute analgesia. Aspirin is faster and produces more potent acute COX inhibition; standardized willow extract produces broader chronic anti-inflammatory effect with the multi-mechanism polyphenol contribution.
The whole-herb advantage also explains why crude willow bark tea, willow tincture, and standardized capsule formulations can all produce meaningful clinical effect — they all preserve the polyphenol fraction along with salicin. Purified salicin tablets, by contrast, have never been a successful pharmaceutical product, despite the obvious commercial logic of an isolated active ingredient. The same is true for many herbal medicines (turmeric/curcumin, milk thistle/silymarin, green tea/EGCG): the whole-plant or whole-extract preparations often outperform the isolated principal compound.
Applications in Chronic Inflammatory Conditions
Willow bark's multi-mechanism anti-inflammatory profile makes it a reasonable adjunctive therapy in several chronic inflammatory conditions:
- Osteoarthritis — the best-established indication after low back pain. The Schmid 2001 and Biegert 2004 trials demonstrated meaningful WOMAC pain reduction. Works well in combination with turmeric, ginger, and glucosamine sulfate. See Arthritis.
- Rheumatoid arthritis — adjunctive to standard DMARD/biologic therapy for residual inflammatory pain. The Setty & Sigal 2005 pilot supports this use. Not a substitute for disease-modifying therapy.
- Ankylosing spondylitis — the inflammatory back pain typical of AS responds to willow extract similarly to chronic mechanical back pain. Adjunctive to NSAID or biologic disease-modifying therapy.
- Psoriatic arthritis — adjunctive use for joint pain alongside standard care; willow's polyphenol fraction may modestly help skin inflammation as well.
- Gout (between attacks) — willow extract's anti-inflammatory action may modestly reduce subacute gout-related joint discomfort. Not for acute gout attacks (which require higher-potency intervention). Combination with tart cherry for purine-related inflammation is sensible. See Gout.
- Tendinopathy and bursitis — chronic soft-tissue inflammation often responds to willow extract similarly to chronic NSAID use, with better tolerability for daily long-term use.
- Fibromyalgia — the inflammatory component of fibromyalgia is debated, but the broad anti-inflammatory effect of willow extract is well-tolerated as adjunctive care alongside standard fibromyalgia management.
For broad pain management protocols see Pain Management and the Pain Management deep-dive.
Why Extract Standardization Matters
The whole-herb advantage hypothesis has an important corollary: the polyphenol fraction of the extract matters as much as the salicin content. Standardized willow extracts are typically calibrated to either 15% or 25% salicin content, but the polyphenol fraction can vary substantially based on:
- Willow species. Salix alba (white willow), Salix purpurea (purple willow), Salix daphnoides (violet willow), and Salix fragilis (crack willow) all contain salicin but differ in their polyphenol profiles. Most clinical trials have used Salix purpurea or mixtures dominated by S. alba.
- Harvest season. Spring-harvested bark typically has higher salicin content than fall-harvested. Polyphenol content varies less seasonally.
- Bark age. Young bark (3-5 year old branches) has higher salicin and polyphenol content than old bark from mature trunk wood.
- Extraction solvent. Aqueous extracts capture salicin and polyphenols efficiently. Alcoholic extracts also capture the polyphenols. Pure salicin isolation (which would be the ultimate "pharmaceutical purification") leaves the polyphenol fraction behind and loses the whole-herb advantage.
- Stabilization. Polyphenols are oxidation-sensitive. Extracts that are properly stabilized (encapsulated, antioxidant-protected, stored cool and dark) retain anti-inflammatory potency. Old or improperly stored extracts may lose polyphenol activity even while retaining stable salicin content.
For consumers, this argues for purchasing standardized extracts from reputable manufacturers that report both salicin content (the regulatory standardization marker) and ideally total polyphenol content (a quality indicator). The trial-grade extracts used in the Chrubasik and Schmid trials were typically prepared by Steigerwald Arzneimittelwerk (the "Assalix" brand in Europe, distributed in the US under various labels) and Bionorica (the "Proaktiv" brand). These provide the most reliable reference points for what an effective willow preparation looks like.
Cautions
- Reye syndrome in children with viral illness — absolute pediatric contraindication during viral infection. The polyphenol fraction does not change the Reye risk; salicin is still the precursor of salicylic acid.
- Salicylate allergy / AERD — absolute contraindication.
- Anticoagulant interaction — some polyphenols (proanthocyanidins, catechins) have mild antiplatelet effects independent of salicylate, which may modestly compound bleeding risk with warfarin or other anticoagulants.
- Active inflammatory bowel disease flare — the tannin fraction in willow extract may be irritating to actively inflamed gut mucosa. Use cautiously, if at all, during IBD flares; better tolerated between flares.
- Iron malabsorption. Tannins in willow extract can bind dietary iron and reduce absorption when taken with iron-containing meals. Take willow extract at a different time from iron-rich meals or iron supplements if iron status is borderline.
- Pregnancy and breastfeeding — avoid, particularly in third trimester. Both salicylate effects on the fetal ductus arteriosus and the broader polyphenol fraction are inadequately studied in pregnancy.
- Concurrent NSAID use — avoid, both for the COX/COX overlap and for the polyphenol fraction's additional NF-kappaB suppression which can complicate inflammatory response measurement.
- Pre-surgical use — discontinue at least one week before scheduled surgery.
Key Research Papers
- Setty AR, Sigal LH (2005). Herbal medications commonly used in the practice of rheumatology: mechanisms of action, efficacy, and side effects (willow bark pilot in rheumatoid arthritis). Seminars in Arthritis and Rheumatism. — PubMed
- Khayyal MT et al. (2005). Mechanisms involved in the anti-inflammatory effect of a standardized willow bark extract. Arzneimittel-Forschung. — PubMed
- Bonaterra GA et al. (2010). Anti-inflammatory effects of the willow bark extract STW 33-I (Proaktiv) in LPS-activated human monocytes and differentiated macrophages. Phytomedicine. — PubMed
- Fiebich BL, Chrubasik S (2004). Effects of an ethanolic salix extract on the release of selected inflammatory mediators in vitro. Phytomedicine. — PubMed
- Wagner I et al. (2003). The effects of standardized willow bark extract on cyclooxygenase-2 expression and prostaglandin E2 production. Phytotherapy Research. — PubMed
- Nahrstedt A et al. (2007). Willow bark extract: the contribution of polyphenols to the overall effect. Wiener Medizinische Wochenschrift. — PubMed
- Sulaiman MR et al. (2008). Antinociceptive and antioedematogenic activities of Salix alba ethanol extract. Pharmaceutical Biology. — PubMed
- Maistro EL et al. (2019). Salicin (a willow bark glycoside) modulates the inflammatory response by regulating the NF-kappaB pathway. Drug and Chemical Toxicology. — PubMed
- Shara M, Stohs SJ (2015). Efficacy and safety of white willow bark (Salix alba) extracts. Phytotherapy Research. — PubMed
- Cameron M, Chrubasik S (2014). Oral herbal therapies for treating osteoarthritis. Cochrane Database of Systematic Reviews. — PubMed
- Esh CJ et al. (2018). The effect of salicortin on cytokine release in human PBMC. Pharmacological Reports. — PubMed
- Drummond EM et al. (2013). Inhibition of proinflammatory biomarkers in THP1 macrophages by polyphenols derived from chamomile, meadowsweet, and willow bark. Phytotherapy Research. — PubMed
PubMed Topic Searches
- PubMed: Willow bark anti-inflammatory mechanism
- PubMed: Salix alba polyphenols flavonoids
- PubMed: Willow bark NF-kappaB TNF-alpha
- PubMed: Willow bark rheumatoid arthritis
- PubMed: Whole-herb advantage phytochemistry
Connections
- Willow Bark Overview
- Willow Bark Benefits Hub
- Willow Bark for Pain Management
- Willow Bark for Headache & Migraine
- Cardiovascular & Aspirin Comparison
- Turmeric (Curcumin)
- Ginger
- Tart Cherry
- Aspirin
- Pain Management
- Arthritis
- Gout
- Chronic Pain
- Joint Pain
- Chronic Low Back Pain
- Glycine & Aspirin Metabolism
- Magnesium
- All Herbs