Willow Bark for Headache and Migraine
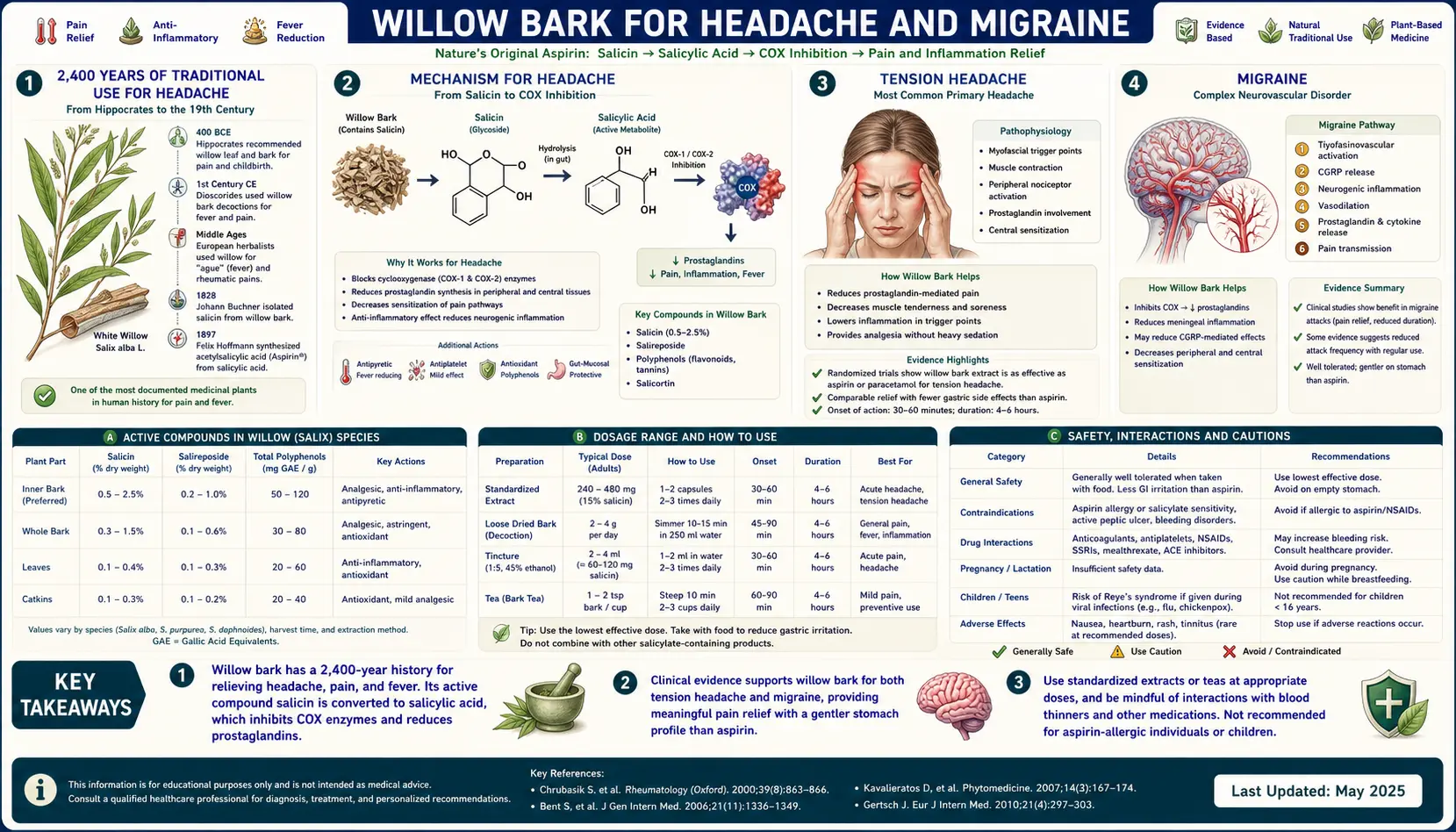
Willow bark has been used as a headache remedy for at least 2,400 years — Hippocrates' "powder of willow" was prescribed for cephalalgia in 5th-century-BCE Greece — and the mechanism is mechanistically straightforward: salicin-derived salicylic acid produces the same cyclooxygenase inhibition that makes aspirin effective for tension headache. The catch is timing. Willow's indirect metabolism (intestinal hydrolysis, hepatic oxidation) delays peak plasma salicylate to 2-3 hours after dosing, compared with 30-45 minutes for aspirin. For acute headache, this is a meaningful disadvantage. For chronic tension-pattern headache or migraine prophylaxis combined with feverfew, magnesium, and riboflavin, willow's longer-duration, GI-gentler profile becomes more attractive. This deep-dive walks through traditional use, the limited but encouraging modern pilot data, head-to-head comparison with aspirin and acetaminophen, and how to think about willow bark in modern headache management.
Table of Contents
- 2,400 Years of Traditional Use for Headache
- Mechanism for Headache
- Tension Headache
- Migraine
- Acute Treatment vs Prophylactic Use
- Willow Bark vs Aspirin for Headache
- Willow Bark vs Acetaminophen for Headache
- Combination Protocols for Migraine Prevention
- Avoiding Medication Overuse Headache
- Dosing for Headache
- Cautions
- Key Research Papers
- Connections
- Featured Videos
2,400 Years of Traditional Use for Headache
Headache is one of the oldest documented indications for willow bark in Western medicine. Hippocrates of Cos (c. 460-370 BCE) recommended willow leaves and willow bark for cephalalgia (headache), gynecological pain in labor, and fever. The Hippocratic prescription — chew the bitter young bark or brew a tea from the powdered older bark — was carried forward by Dioscorides in the 1st century CE and remained a staple of Western herbal medicine through the medieval and early modern periods.
Independent North American ethnobotanical use is well documented: the Cherokee chewed inner willow bark for headache and toothache; the Iroquois Confederacy used Salix nigra (black willow) decoction for headache and fever; the Lenape and other Algonquian peoples used willow preparations for "head pain" and as part of fever-management compresses. The convergent discovery on two continents that willow bark relieves headache is strong evidence the effect is real and substantial — humans across cultures independently identified the same plant for the same purpose without communication.
Edward Stone's 1763 Royal Society paper specifically cited reduction in headache as one of the symptoms responsive to willow bark in his 50-patient case series. By the 19th century, willow bark and isolated salicin were standard analgesics in European pharmacopoeias for headache, fever, and rheumatism. Bayer's 1899 launch of aspirin (acetylsalicylic acid) was marketed heavily as a headache remedy, and aspirin's commercial success cemented salicylates as the dominant first-line headache treatment for the entire 20th century until acetaminophen (paracetamol) emerged as a comparable OTC option in the 1950s and the triptans transformed migraine-specific management starting with sumatriptan in 1991.
The historical record makes clear that willow has been used for headache continuously across 2,400 years of Western medicine. Modern willow extract preparations sit at the start of the salicylate analgesic chain that produces aspirin's headache effect — the same downstream mechanism, just with the slower-onset, gentler-on-the-stomach pharmacokinetic profile of the natural glycoside form.
Mechanism for Headache
Most headache pain is mediated by activation of trigeminovascular nociceptive pathways and by sensitization of central pain processing in the spinal trigeminal nucleus and thalamus. Prostaglandins, particularly PGE2 and PGI2 (prostacyclin), are key inflammatory mediators that:
- Sensitize peripheral nociceptors to other algogenic stimuli (kinins, serotonin, histamine), lowering the threshold for pain
- Dilate cerebral and meningeal vessels, contributing to the throbbing component of vascular headache
- Promote release of CGRP (calcitonin gene-related peptide), the principal neurotransmitter mediator of migraine, from trigeminal sensory neurons
- Drive neurogenic inflammation in the dura mater, a key element of migraine pathophysiology
Salicin-derived salicylic acid's cyclooxygenase inhibition reduces prostaglandin synthesis, which interrupts this cascade at several steps. Plus, the willow polyphenol fraction's NF-kappaB inhibition reduces the inflammatory upregulation of COX-2 in stressed brain tissue and reduces secondary cytokine production that amplifies headache pain. The combined effect is a broad-spectrum reduction in headache-relevant inflammatory signaling, similar in mechanism to aspirin but somewhat broader because of the polyphenol contribution discussed in the Anti-Inflammatory deep-dive.
The key clinical caveat is timing. Willow bark's indirect metabolism — intestinal hydrolysis of salicin to saligenin, hepatic oxidation to salicylic acid — takes 2-3 hours to reach peak plasma salicylate concentration. Aspirin reaches peak in 30-45 minutes. For acute headache where rapid relief is the priority, aspirin's faster onset is a meaningful advantage. For chronic recurrent headache or for tension-pattern headache that builds slowly, willow's slower-onset, longer-duration profile can be acceptable or even preferable.
Tension Headache
Tension-type headache (TTH) is the most common primary headache disorder, affecting 30-78% of adults at some point. Episodic tension headache (less than 15 days per month) and chronic tension headache (15 or more days per month) together account for the substantial majority of headaches in the general population. The pain is typically bilateral, pressing or tightening rather than throbbing, mild to moderate intensity, not aggravated by routine physical activity, and without prominent nausea or photophobia (which would suggest migraine instead).
The pharmacological response of tension headache to NSAIDs is well-documented: aspirin 500-1000 mg or ibuprofen 400 mg produces meaningful pain reduction in 50-60% of acute tension headache episodes within 1-2 hours. Acetaminophen 1000 mg has slightly smaller effect but is the preferred choice when NSAID is contraindicated. The COX-inhibition mechanism is responsible for the analgesic effect.
Modern clinical trials specifically of willow bark for tension headache are limited — the indication has not attracted significant pharmaceutical-industry research interest because aspirin is generic, OTC, fast-acting, and well-established. However, the mechanism is identical to aspirin (cyclooxygenase inhibition by salicylic acid), and clinical experience supports willow bark as a reasonable choice for patients seeking a slower-onset, GI-gentler alternative to chronic NSAID use for recurrent tension headache. A typical therapeutic dose of 120-240 mg of salicin produces roughly the same analgesic mechanism as a low-to-moderate dose of aspirin, with the onset and duration profile discussed above.
For patients with chronic tension headache who are taking daily or near-daily NSAID or aspirin, transitioning to willow bark may reduce GI toxicity and the risk of medication-overuse headache (see below). The slower onset of willow makes it less attractive as PRN acute treatment, but as a daily background analgesic for chronic tension headache it works through a sensible mechanism.
Migraine
Migraine is a different clinical entity from tension headache: typically unilateral throbbing pain, moderate to severe intensity, aggravated by routine activity, accompanied by nausea, photophobia, phonophobia, and sometimes preceded by visual or sensory aura. Migraine pathophysiology involves cortical spreading depression, trigeminovascular activation, CGRP release, and meningeal neurogenic inflammation. The triptan class (sumatriptan, rizatriptan, others) and the newer CGRP-receptor antagonists (rimegepant, ubrogepant) target migraine-specific mechanisms and are the most effective acute migraine treatments. The CGRP-antibody class (erenumab, fremanezumab, galcanezumab, eptinezumab) targets migraine prevention.
NSAIDs and aspirin remain useful in migraine, particularly for mild-to-moderate attacks and as part of combination protocols. Aspirin 900-1000 mg (high dose) has demonstrated efficacy in randomized trials for acute migraine, particularly when combined with metoclopramide for anti-emetic effect and improved gastric absorption. Ibuprofen 600-800 mg has similar evidence.
The role of willow bark in migraine is more limited than in tension headache. The slower onset (2-3 hours to peak plasma salicylate) is a significant disadvantage for acute migraine, where the typical attack reaches peak intensity within 1-2 hours and the patient wants relief immediately. The triptan class produces meaningful relief within 30-60 minutes; even aspirin and ibuprofen at therapeutic doses act faster than willow. Willow bark is not the right choice for acute moderate-to-severe migraine.
The exception is in migraine prophylaxis: chronic daily preventive treatment intended to reduce attack frequency rather than acute symptom relief. Willow bark's slower-onset, longer-duration profile and substantially lower GI toxicity make it a reasonable adjunctive component of natural migraine prevention protocols, particularly combined with magnesium, riboflavin (B2), CoQ10, and feverfew — see the combination protocols section below.
For comprehensive migraine information see Migraine.
Acute Treatment vs Prophylactic Use
The acute-vs-prophylactic distinction is central to thinking about willow bark in headache management:
- Acute treatment (PRN dosing at headache onset, intended to abort or relieve the current headache). The relevant pharmacokinetic property is time-to-peak plasma concentration. Aspirin (30-45 min), ibuprofen (1-2 hr), and the triptans (30-60 min for oral, 10-15 min for subcutaneous sumatriptan) all act faster than willow bark (2-3 hr). For acute treatment, willow is generally not first-line.
- Prophylactic / preventive treatment (daily dosing intended to reduce attack frequency or severity over weeks-to-months). The relevant pharmacokinetic property is steady-state plasma concentration with daily dosing, not time-to-peak. Willow bark dosed daily at 240 mg salicin reaches stable plasma salicylate within 2-3 days and maintains it indefinitely with continued use. The GI tolerability and absence of antiplatelet effect become advantages rather than disadvantages over the duration of chronic use.
The integrative headache-management protocol that makes most sense:
- Identify the patient's headache pattern (episodic tension, chronic tension, episodic migraine, chronic migraine, mixed)
- For acute headache treatment, use a fast-onset agent appropriate to the headache type (aspirin or ibuprofen for tension headache; triptan for moderate-to-severe migraine; combination triptan + NSAID for refractory acute migraine)
- For headache prevention (chronic tension headache or frequent migraine), consider willow bark as part of a daily prophylactic regimen alongside other natural preventive agents
- Minimize total acute-medication-day exposure to avoid medication-overuse headache (see below)
Willow Bark vs Aspirin for Headache
For acute headache, aspirin has clear advantages over willow bark:
- Faster onset (30-45 minutes versus 2-3 hours)
- Higher peak plasma salicylate (20-50 µg/mL after a typical 500-1000 mg aspirin dose, versus 1-3 µg/mL after a typical 240 mg willow salicin dose)
- More potent acute COX-1 and COX-2 inhibition
- Well-established clinical trial evidence for both tension headache and acute migraine
For chronic daily headache prophylaxis, the calculus shifts somewhat:
- Willow has substantially lower GI toxicity than chronic daily aspirin. The risk of gastric ulceration and GI bleeding is the principal limit on chronic aspirin use.
- Willow does not produce durable platelet inhibition, which is an advantage for patients who need to maintain normal coagulation but a disadvantage for patients who have cardiovascular comorbidities where aspirin's antiplatelet effect is desired. See the Cardiovascular & Aspirin Comparison deep-dive.
- Both equally produce the salicylate Reye-syndrome risk in children — willow is NOT a "safer" salicylate for pediatric use during viral illness.
- Willow's polyphenol fraction may add modest additional anti-inflammatory benefit beyond aspirin's pure COX inhibition.
The practical recommendation: aspirin for acute headache treatment in adults without contraindications. Willow bark for chronic prophylactic use, particularly when chronic NSAID GI toxicity is a concern.
Willow Bark vs Acetaminophen for Headache
Acetaminophen (paracetamol) is the other common OTC headache analgesic and is mechanistically quite different from both willow bark and aspirin. Acetaminophen produces analgesic and antipyretic effect through central nervous system mechanisms that are only partially understood — it weakly inhibits CNS cyclooxygenase (particularly the COX-3 splice variant in brain), activates descending serotonergic and cannabinoid analgesic pathways, and modulates the spinal nociceptive transmission. It is NOT a significant peripheral COX inhibitor and has essentially no anti-inflammatory effect at clinical doses.
Key clinical differences:
- Acetaminophen has no anti-inflammatory effect. For pure tension headache (which is not significantly inflammatory), this matters less. For migraine (which involves substantial neurogenic inflammation), willow's anti-inflammatory action provides additional mechanism not addressed by acetaminophen.
- Acetaminophen is safer in pregnancy than willow or aspirin, particularly in the third trimester. Acetaminophen is the standard-of-care analgesic in pregnancy for both headache and other pain.
- Acetaminophen lacks willow's GI side effects entirely (no COX-1 inhibition, no gastric mucosal effects).
- Acetaminophen has hepatotoxicity at doses above 4000 mg/day or with alcohol use. Willow bark has minimal hepatotoxic potential at therapeutic doses.
- Acetaminophen lacks willow's polyphenol fraction — no NF-kappaB inhibition, no TNF-alpha suppression, no antioxidant benefit.
For acute tension headache in non-pregnant adults, acetaminophen and willow bark produce roughly comparable analgesic effect with different side effect profiles. For migraine, the anti-inflammatory mechanism gives willow a modest theoretical edge over acetaminophen. For pregnancy and breastfeeding, acetaminophen is preferred.
Combination Protocols for Migraine Prevention
Willow bark fits naturally into multi-component natural migraine prevention protocols, where the goal is reducing attack frequency by 50% or more over 3-6 months of daily use. Several evidence-supported combinations:
- Magnesium (typically magnesium glycinate or magnesium citrate, 300-600 mg elemental daily). Multiple RCTs support magnesium for migraine prevention, with effect size of 20-40% attack frequency reduction over placebo. See Magnesium.
- Riboflavin (Vitamin B2) (400 mg daily). The 1998 Schoenen trial showed 50% reduction in migraine days versus placebo over 3 months. Now a Level A recommendation by the American Headache Society for migraine prevention.
- CoQ10 (100 mg three times daily, total 300 mg daily). The 2005 Sandor trial showed 50% reduction in migraine frequency in 47.6% of patients versus 14.4% of placebo controls over 3 months.
- Feverfew (Tanacetum parthenium, 100-300 mg standardized extract daily). Older trials showed modest preventive effect; meta-analyses are mixed but suggest a small-to-moderate preventive benefit.
- Willow bark (240 mg salicin daily) added on top of the above provides a daily background of anti-inflammatory action via COX inhibition + polyphenol effects. Particularly relevant when the patient also has chronic mechanical pain (back, joints) that benefits from the same anti-inflammatory profile.
The typical combination regimen looks like: magnesium glycinate 400 mg + riboflavin 400 mg + CoQ10 300 mg + feverfew 200 mg + willow bark extract delivering 240 mg salicin, all taken daily, with 3 months of consistent use before assessing response. Trial-grade evidence for each component individually is reasonable; trial-grade evidence for the specific combination is more limited but mechanistically sensible.
For comprehensive non-pharmacologic migraine management see Migraine.
Avoiding Medication Overuse Headache
Medication overuse headache (MOH, formerly called "rebound headache") is a real and underrecognized complication of frequent acute headache medication use. It occurs when acute medications taken too often (typically more than 10-15 days per month for triptans, NSAIDs, or analgesics; more than 10 days per month for combination analgesics or opioids) themselves induce chronic daily headache.
The mechanism involves CNS sensitization, downregulation of endogenous antinociceptive pathways, and rebound vasodilation as the medication wears off. Patients caught in this cycle often increase medication frequency to chase relief, worsening the underlying MOH problem.
Willow bark's role in this context is dual:
- Risk: Daily willow bark used as acute treatment for daily headache can contribute to MOH similarly to daily aspirin or NSAID use. The salicylate exposure is real.
- Mitigation: Daily willow bark used for headache PREVENTION (as part of a prophylactic regimen) rather than for acute symptom relief allows reduction in acute medication days, which can break the MOH cycle.
The practical guideline: use willow bark as a daily prophylactic agent (combined with the magnesium / riboflavin / CoQ10 / feverfew preventive stack), and reserve specific fast-onset agents (triptans for migraine, ibuprofen for tension headache) for acute breakthrough symptoms. Target acute-medication-day exposure of less than 10 days per month to avoid MOH.
Dosing for Headache
- For acute tension headache: 240 mg salicin (typically one or two standardized extract capsules). Onset is slow (1-2 hours for partial effect, 2-3 hours for peak). Not ideal for acute migraine.
- For chronic tension headache prophylaxis: 240 mg salicin daily, taken at the same time each day with food. Effect builds over 2-4 weeks.
- For migraine prophylaxis (as part of combination protocol): 240 mg salicin daily, combined with magnesium, riboflavin, CoQ10, and feverfew per the protocol above. Three-month trial before assessing response.
- For migraine acute treatment: Willow is NOT first-line. Use a triptan or NSAID + metoclopramide instead. Willow may be useful as add-on in mild attacks but is too slow-onset for primary acute use.
- Combining with other natural headache agents: Magnesium, riboflavin, CoQ10, and feverfew all have favorable interaction profiles with willow. Glycine 3-5 g at bedtime supports the glycine-conjugation elimination pathway and is sensible co-supplementation.
Cautions
- Reye syndrome in children with viral illness — absolute pediatric contraindication. Children with febrile viral illness (especially influenza, chickenpox) must not receive willow bark for headache or any other indication.
- Salicylate allergy / AERD — absolute contraindication. Patients with aspirin-sensitive asthma will cross-react with willow.
- Acute severe headache with red flags — sudden severe "thunderclap" headache, headache with fever and neck stiffness, headache with focal neurologic findings, headache after head trauma, or new headache after age 50 requires urgent evaluation, not herbal therapy. Willow is appropriate only for benign primary headache disorders that have been diagnostically clarified.
- Migraine with aura and stroke risk — women with migraine with aura have modestly elevated stroke risk. While willow does not provide aspirin's antiplatelet cardioprotection, this group should not interpret willow use as cardiovascular protection.
- Anticoagulants — additive bleeding risk with warfarin, clopidogrel, DOACs. Important consideration for older headache patients on cardiovascular medications.
- Concurrent NSAID use — avoid concurrent willow + ibuprofen / naproxen / diclofenac use on the same day.
- Pregnancy — avoid; acetaminophen is the preferred headache analgesic during pregnancy.
- Medication overuse headache — track acute medication days carefully; willow used too frequently for acute headache can contribute to MOH.
- Tinnitus — high-dose salicylates produce reversible tinnitus. If ringing in ears develops, reduce dose.
Key Research Papers
- Diener HC et al. (2005). Efficacy and safety of 6.25 mg t.i.d. feverfew CO2-extract (MIG-99) in migraine prevention — a randomized, double-blind, multicentre, placebo-controlled study. Cephalalgia. — PubMed
- Schoenen J et al. (1998). Effectiveness of high-dose riboflavin in migraine prophylaxis. A randomized controlled trial. Neurology. — PubMed
- Sandor PS et al. (2005). Efficacy of coenzyme Q10 in migraine prophylaxis: a randomized controlled trial. Neurology. — PubMed
- Diener HC et al. (2004). The fixed combination of acetylsalicylic acid, paracetamol and caffeine is more effective than single substances and dual combination for the treatment of headache. Cephalalgia. — PubMed
- Lipton RB et al. (2005). Efficacy and safety of acetaminophen, aspirin, and caffeine in alleviating migraine headache pain. Archives of Neurology. — PubMed
- Kirthi V et al. (2013). Aspirin with or without an antiemetic for acute migraine headaches in adults. Cochrane Database of Systematic Reviews. — PubMed
- Mauskop A, Varughese J (2012). Why all migraine patients should be treated with magnesium. Journal of Neural Transmission. — PubMed
- Chrubasik S et al. (2001). Treatment of low back pain exacerbations with willow bark extract: a randomized double-blind study. American Journal of Medicine. — PubMed
- Pareek A et al. (2011). Feverfew (Tanacetum parthenium L.): A systematic review. Pharmacognosy Reviews. — PubMed
- Vlachojannis JE et al. (2009). A systematic review on the effectiveness of willow bark for musculoskeletal pain. Phytotherapy Research. — PubMed
- Headache Classification Committee of the International Headache Society (2018). The International Classification of Headache Disorders, 3rd edition. Cephalalgia. — PubMed
- Diener HC, Limmroth V (2004). Medication-overuse headache: a worldwide problem. Lancet Neurology. — PubMed
PubMed Topic Searches
- PubMed: Willow bark headache
- PubMed: Salicylate headache mechanism
- PubMed: Migraine prophylaxis natural supplement
- PubMed: Tension headache NSAID
- PubMed: Feverfew/riboflavin/magnesium migraine
Connections
- Willow Bark Overview
- Willow Bark Benefits Hub
- Willow Bark for Pain Management
- Willow Bark Anti-Inflammatory
- Cardiovascular & Aspirin Comparison
- Headache
- Migraine
- Migraine (Neurology)
- Aspirin
- Pain Management
- Magnesium
- Glycine
- Glycine & Aspirin Metabolism
- Turmeric
- Ginger
- Chronic Pain
- All Herbs
- Tension Headache — the headache type willow bark suits best, since its COX-inhibition mechanism matches the aspirin response documented for TTH.