Tension Headache
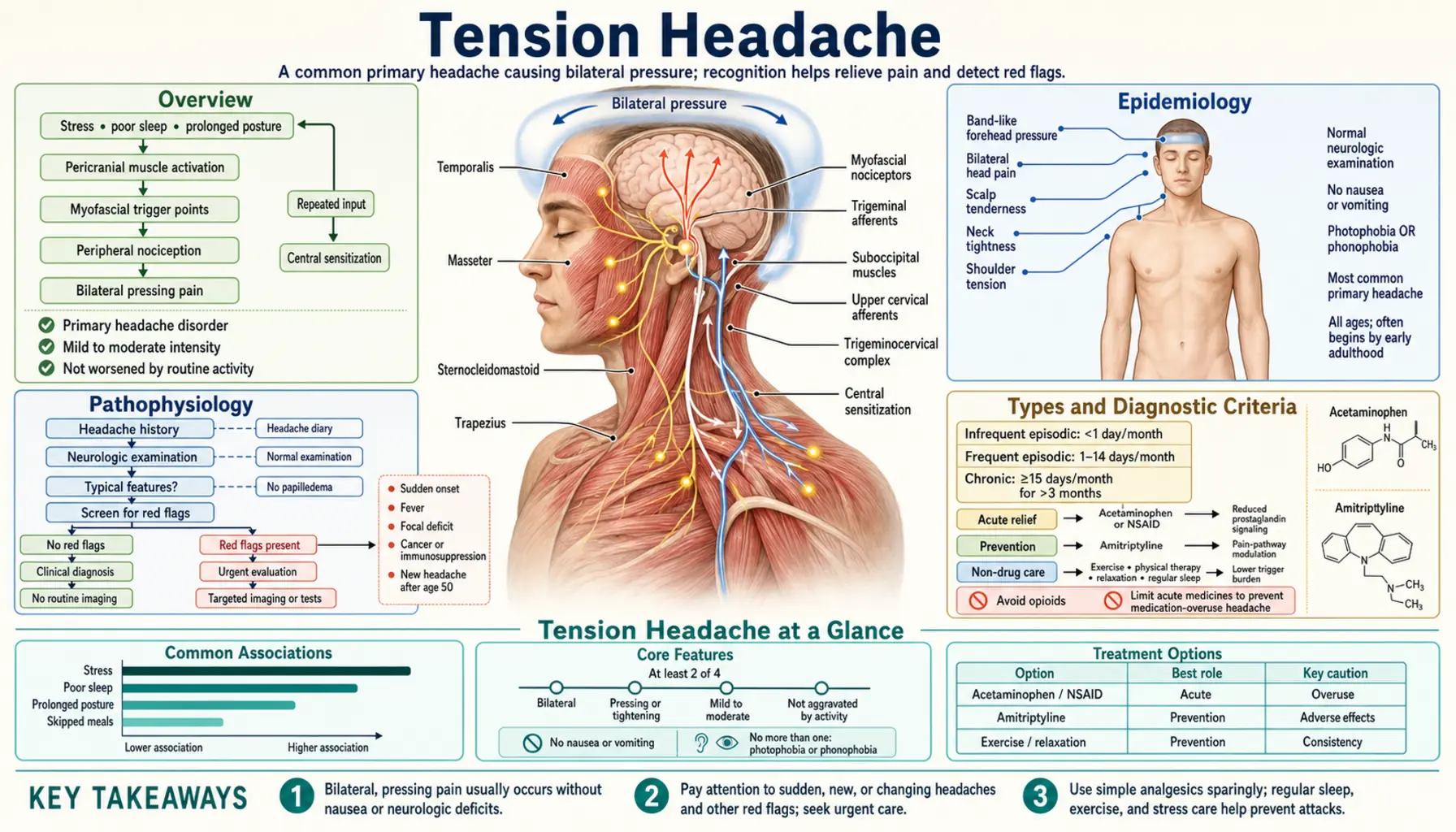
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Types and Diagnostic Criteria
- Clinical Presentation
- Triggers and Risk Factors
- Diagnosis
- Treatment — Episodic
- Treatment — Chronic Prevention
- Non-Pharmacological Approaches
- Recent Research and Advances
- Research Papers
- Connections
- Featured Videos
1. Overview
Tension headache — also called tension-type headache (TTH) — is the most common headache disorder in the world, and almost certainly the most common pain condition most people will ever experience. If you have ever felt a dull, steady pressure around your head after a stressful day at work, or woken with a tight band squeezing across your forehead and temples, you already know this headache from the inside. Estimates suggest that about 78% of the general population will experience a tension headache at some point in their lives.
Despite how ordinary the name sounds, tension headache matters enormously at the population level. The episodic form — coming and going with stress, poor sleep, or missed meals — is usually manageable with simple over-the-counter medication. But a substantial minority of sufferers progress to chronic tension headache, defined as 15 or more headache days per month for longer than three months, and in that form the condition becomes a genuine disability: missed workdays, impaired concentration, damaged relationships, and a relentless drain on quality of life. Worldwide, roughly 3% of adults live with this chronic form — approximately 180 million people.
This page is written for the person who lives with these headaches, not just for clinicians. That means plain language about what is actually happening in your head, honest information about which treatments work and which do not, and practical tools for managing both the occasional and the persistent forms of this condition. Two ideas run through everything below. First, tension headache is not imaginary, not “just stress,” and not something you have to simply endure — effective treatments exist, both for acute attacks and for preventing chronic ones. Second, the line between episodic and chronic tension headache is not fixed: understanding the warning signs of progression — and the single biggest driver of that progression, medication overuse — gives you real power to protect yourself.
2. Epidemiology
Tension headache is a global phenomenon that touches nearly every culture and demographic. The 1-year prevalence of episodic tension-type headache ranges from approximately 38% to 74% across different populations studied worldwide — a staggeringly wide range that reflects the difficulty of asking the same question in different languages and healthcare cultures, but also the genuine ubiquity of the condition. The chronic form (15+ days/month) affects roughly 3% of adults globally, which translates to well over a hundred million people carrying this burden on any given day.
Age patterns reveal something important. Tension headache is most prevalent in adults aged 30 to 39 years — the peak years of professional and family demands — and then gradually declines with age. Women are somewhat more affected than men, with a ratio of roughly 1.4 to 1 in most large studies, though the gap is far smaller than in migraine, where women are three times more likely to be affected. The condition begins in childhood and adolescence for many people, long before the stressors of adult life arrive.
The economic impact is substantial and often invisible. Because individual tension headache attacks are not usually severe enough to prompt emergency visits or long hospitalizations, the cost shows up elsewhere: in lost work productivity, reduced concentration, and reduced quality of life for millions of people who show up to work or school carrying a headache they have silently learned to live with. A landmark global burden-of-disease analysis found that tension-type headache was one of the most prevalent conditions worldwide and a major contributor to years lived with disability. The headache that “everyone gets” turns out, in aggregate, to be one of humanity’s most expensive common ailments.
One critical epidemiological point deserves emphasis: chronic tension headache is not an inevitable progression from episodic tension headache. Studies show that transformation from episodic to chronic is not a one-way street. Many people with frequent episodic headaches never progress to chronic, and many people with chronic headache return to episodic frequency — especially when medication overuse is identified and addressed. Understanding and interrupting the progression pathway is one of the most practical things you can do for your own health.
3. Pathophysiology
What actually causes the pain in a tension headache? Honest answer: we do not fully understand it, and the answer turns out to differ between the episodic and chronic forms. The current scientific picture has two levels — one in the muscles of the head and neck (peripheral), and one in the brain’s own pain-processing centers (central).
Peripheral sensitization: the muscles
The most consistent physical finding in people with tension headache is increased tenderness of the pericranial muscles — the muscles around the skull, including the temporalis (temples), masseter (jaw), sternocleidomastoid (neck), trapezius (shoulders), and suboccipital (base of skull) muscles. When a clinician presses on these muscles in a person with tension headache, they find significantly more pain than in someone without headache. This tenderness is not imagined — it correlates with headache frequency and severity in systematic studies.
The leading peripheral theory is that sustained contraction or poor posture in these muscles activates pain-sensing nerve endings (nociceptors) in the muscle tissue. Hours of hunching over a keyboard, holding the phone between your shoulder and ear, or tensing your jaw during a stressful meeting can activate exactly these nociceptors. But here is an important nuance: the muscle tenderness alone does not explain everything. Many people have tight neck muscles without headache, and the relationship between objective muscle tension and pain varies considerably between individuals. The muscles are a central part of the story — probably the dominant part in episodic TTH — but not the whole story.
Central sensitization: the brain turns up the volume
In chronic tension headache, the picture shifts. With repeated, prolonged activation of pericranial nociceptors over weeks and months, the brain’s pain-processing systems can undergo a change called central sensitization — the nervous system essentially “turns up the volume” on pain signals, so that stimuli that would normally not be painful (or only mildly so) start triggering significant pain. The pain threshold lowers system-wide, not just in the head.
This central sensitization is thought to be the key mechanism that transforms an episodic headache pattern into a chronic one. Once established, it means the headache has partly taken on a life of its own, independent of whatever peripheral trigger started it. This explains why treating chronic tension headache requires centrally-acting preventive medications like amitriptyline — which work on brain chemistry, not just muscle tension — rather than just pain relievers and posture correction.
The role of stress and the brain
Psychological stress is the trigger most consistently reported by tension headache patients, and there is biological plausibility behind this. Stress activates the hypothalamic-pituitary-adrenal (HPA) axis, produces cortisol fluctuations, disrupts sleep architecture, and increases baseline muscle tone — all of which feed into both the peripheral and central sensitization pathways. Anxiety and depression are significantly more common in people with chronic tension headache than in the general population, and this is a bidirectional relationship: pain causes distress, and distress amplifies pain.
What tension headache is not
Unlike migraine, tension headache does not involve the neurogenic inflammation and calcitonin gene-related peptide (CGRP) cascade that drives the throbbing, nausea, and light sensitivity of a migraine attack. Tension headache involves different pain-processing pathways, which is why triptans — the drugs that specifically target the migraine mechanism — are generally ineffective for tension headache. Serotonin and nitric oxide may play modulatory roles in both conditions, but the specific migraine cascade is absent. This distinction is clinically important: tension headache and migraine are genuinely different conditions that require different treatments, even though they can sometimes be hard to tell apart.
4. Types and Diagnostic Criteria
Tension headache is formally defined by the International Headache Society (IHS) International Classification of Headache Disorders, 3rd edition (ICHD-3), published in 2018. The ICHD-3 divides tension-type headache into two main categories based on frequency, with episodic TTH further split into infrequent and frequent subtypes.
Episodic tension-type headache (ETTH)
Episodic TTH means fewer than 15 headache days per month. It is further divided:
- Infrequent episodic TTH: fewer than 1 day per month on average (<12 days per year). Common in the general population; usually manageable with simple OTC treatment; low disability burden.
- Frequent episodic TTH: 1 to 14 days per month on average for more than 3 months. More likely to interfere with daily life; warrants evaluation for preventive treatment if attacks are frequent enough.
Chronic tension-type headache (CTTH)
Chronic TTH is defined as headache occurring on 15 or more days per month for more than 3 months. This is a clinically distinct condition from episodic TTH — not simply “more of the same” but a different entity driven significantly by central sensitization. CTTH is a major cause of disability and typically requires preventive pharmacological treatment plus behavioral intervention.
ICHD-3 diagnostic criteria
For a headache to be classified as tension-type, the ICHD-3 requires:
- At least 2 of these 4 pain characteristics:
- Bilateral location (both sides of the head, not just one side)
- Pressing or tightening quality — described as a “band around the head,” a vice, or a weight; not pulsating or throbbing
- Mild to moderate intensity (not severe)
- Not aggravated by routine physical activity such as walking or climbing stairs
- Both of the following:
- No nausea and no vomiting (mild nausea is permissible only in CTTH)
- No more than one of photophobia (light sensitivity) or phonophobia (sound sensitivity) — not both simultaneously
- Not better accounted for by another headache diagnosis
- Duration: 30 minutes to 7 days for episodic TTH; hours to continuous for CTTH
These criteria exist to distinguish tension headache from migraine, where the pattern is typically: unilateral, pulsating, moderate-to-severe, worsened by activity, with nausea and both photophobia AND phonophobia. In practice, headache types can overlap or co-exist, and some patients with frequent TTH also carry a migraine diagnosis. When in doubt, a neurologist or headache specialist can help sort out the pattern.
5. Clinical Presentation
The hallmark of tension headache is a pain that feels fundamentally different from migraine pain — and understanding that difference helps explain both the condition itself and why the treatments diverge sharply.
The characteristic pain
Most people describe tension headache as a dull, steady, pressing or squeezing pressure — like a tight band, helmet, or vice gripping the head. It is classically bilateral (both sides), though it may be more pronounced at the forehead, temples, back of the head, or all three simultaneously. The intensity is mild to moderate: enough to be distracting and unpleasant, but usually not enough to stop you from functioning. You can typically still walk up a flight of stairs without the headache worsening — a key distinction from migraine, which often intensifies with the slightest movement.
There is no aura (no visual disturbances, tingling, or speech changes before the headache), no throbbing or pulsating quality, and no significant nausea or vomiting. Light and sound sensitivity may be mildly present but not together — and in practice many tension headache sufferers find bright fluorescent lights uncomfortable, which can confuse the distinction with migraine until the overall pattern is assessed.
Pericranial tenderness: the clinical signature
One of the most reproducible physical findings in tension headache — one that can be examined in a clinical visit — is increased tenderness of the pericranial muscles when pressed. Clinicians use a standardized palpation technique, pressing small circles into the temporal, masseter, sternocleidomastoid, trapezius, and suboccipital muscle groups and rating pain on a scale. People with tension headache, especially CTTH, score significantly higher on this “Total Tenderness Score” than headache-free controls. The muscles of the neck and scalp are, in a literal sense, physically sensitized in ways that can be measured and documented.
Key differences from migraine
Because the two conditions are sometimes confused and can co-exist, here is a side-by-side summary of the key distinguishing features:
- Location: Tension headache is bilateral; migraine is typically unilateral (one side)
- Quality: Tension = pressing or tightening; Migraine = pulsating or throbbing
- Severity: Tension = mild-to-moderate; Migraine = moderate-to-severe (often disabling)
- Nausea/vomiting: Absent in tension headache; present in ~90% of migraine attacks
- Physical activity: Tension headache is NOT worsened by movement; migraine typically IS
- Light and sound: At most one of these in tension headache; both are typical in migraine
- Aura: No aura in tension headache; aura (visual or sensory) precedes ~30% of migraines
- Duration: Tension = 30 min to 7 days; Migraine = 4 to 72 hours
A practical tip: if the headache is severe enough that you cannot function, or if it is accompanied by significant nausea, or if you find yourself going to lie down in a dark quiet room, migraine is the more likely diagnosis and the treatments differ significantly from those for tension headache.
6. Triggers and Risk Factors
Tension headache has well-characterized triggers — factors that reliably precede attacks in many sufferers. Recognizing your personal trigger pattern is one of the most practical steps toward reducing headache frequency, because many triggers are modifiable. A headache diary (recording when headaches occur, how long they last, what preceded them, and what helped) kept for 4 to 6 weeks is one of the most useful tools a patient can bring to their clinician.
Common triggers
- Psychological stress: The most consistently reported trigger across studies. Both the acute stress of a difficult day and the “let-down” effect (headaches appearing on weekends or vacations after stress releases) are recognized patterns.
- Sleep disturbances: Too little sleep, too much sleep, inconsistent sleep schedules, and poor sleep quality all increase headache frequency. Sleep and headache have a bidirectional relationship — each worsens the other.
- Hunger and skipped meals: Low blood sugar is a potent headache trigger for many people. Regular meal timing is straightforward prevention.
- Dehydration: Even mild dehydration reliably triggers headaches in susceptible individuals. Adequate daily fluid intake is simple, no-cost prevention.
- Poor posture: Hours in a forward-head posture at a computer or phone puts sustained load on the posterior neck muscles and upper trapezius — a direct route to pericranial muscle sensitization.
- Eyestrain: Prolonged screen time, uncorrected refractive errors, or working in poor lighting can contribute, particularly to forehead and temple tension.
- Caffeine: Both excessive caffeine consumption and caffeine withdrawal are recognized headache triggers. Regular coffee drinkers who miss their morning dose often experience a withdrawal headache by late morning.
- Alcohol: Can trigger or worsen tension headache, especially the day after consumption.
- Weather and environmental changes: Barometric pressure changes, high humidity, and bright glare are reported by many sufferers, though the precise mechanisms are less clear.
- Anxiety and depression: Both are significantly more common in people with frequent or chronic tension headache and act as both triggers and perpetuating factors.
Risk factors for progression to chronic TTH
Not everyone with episodic tension headache develops the chronic form. Key risk factors for progression include:
- Medication overuse: The single most important modifiable risk factor. Using simple analgesics or triptans on more than 10 to 15 days per month can itself cause “medication overuse headache” (MOH), sometimes called rebound headache, which transforms episodic into chronic pattern. This is a cruel trap — the medication that relieves the headache today increases the probability of a headache tomorrow.
- Female sex
- Anxiety and depression
- High stress levels and poor coping strategies
- Sleep disorders
- Obesity
- High baseline headache frequency
7. Diagnosis
Tension headache is a clinical diagnosis — made by history and physical examination, not by scans or blood tests. There is no brain MRI finding, no blood test, and no nerve test that “shows” tension headache. Neuroimaging is normal in tension headache and is only warranted when the history suggests a secondary cause (a headache with an underlying structural problem driving it).
Red flag symptoms requiring urgent evaluation
Most tension headaches do not require urgent medical attention. But certain warning signs indicate a headache that may have a dangerous underlying cause and requires prompt evaluation:
- Thunderclap headache: Maximum-intensity pain that arrives in seconds to minutes (“the worst headache of my life”) — possible subarachnoid hemorrhage
- Headache with fever, stiff neck, or rash — possible meningitis
- Headache with focal neurological symptoms (weakness, vision changes, speech difficulty, confusion)
- Headache that is progressively worsening over weeks
- New headache over age 50 — possible temporal arteritis or space-occupying lesion
- Headache associated with head trauma
- Headache that consistently wakes you from sleep (warrants evaluation even though tension headaches can occasionally do this)
The clinical evaluation
When you see a clinician for headache evaluation, they will take a detailed headache history: frequency, duration, character of pain, location, associated symptoms (nausea, light or sound sensitivity, aura), triggers, what relieves the pain, medication use including over-the-counter drugs and their frequency, and the impact on daily life. A neurological examination and palpation of the pericranial muscles will typically be performed. The ICHD-3 criteria above will be applied — explicitly or implicitly — to classify the headache type.
A headache diary kept for at least 4 weeks before the appointment is one of the most useful things a patient can bring. It converts vague recollections into objective data: how many headache days per month, what medications were used and how often, what triggers preceded attacks. This single document can make the difference between a precise diagnosis and an educated guess.
8. Treatment — Episodic
For the individual tension headache attack, simple analgesics are the mainstay of treatment and they work well when used judiciously. The key word is judiciously — because the biggest risk in treating episodic tension headache is overusing the same medications that relieve it, which can transform episodic into chronic headache over time.
First-line medications (OTC)
All three of the following are effective and recommended by major guidelines:
- Aspirin 500–1000 mg: Effective and inexpensive. Clinical trials show a Number Needed to Treat (NNT) of approximately 3 for complete relief at 2 hours — meaning roughly 1 in 3 people who take aspirin for a tension headache will have complete relief who would not have had it without the drug. Take with food to reduce gastric irritation. Avoid in children under 16, people with stomach ulcers, and those on blood thinners.
- Ibuprofen 200–800 mg: Also highly effective, NNT approximately 3–4. Non-steroidal anti-inflammatory drugs (NSAIDs) as a class tend to outperform acetaminophen in most head-to-head tension headache trials. Take with food; avoid with kidney problems or a history of stomach ulcers.
- Acetaminophen (paracetamol) 500–1000 mg: Effective and generally the safest option for people who cannot take NSAIDs (stomach ulcer history, kidney disease, anticoagulant use). NNT slightly higher than NSAIDs in most studies. Do not exceed recommended daily doses; liver toxicity is a real risk with overuse, especially combined with alcohol.
- Naproxen 375–550 mg: A longer-acting NSAID; useful when headaches tend to last many hours. Slower onset than ibuprofen.
Caffeine combinations
Fixed-dose combinations of analgesics with caffeine (such as aspirin + acetaminophen + caffeine) show modestly superior efficacy compared to the analgesic alone in well-conducted trials. Caffeine enhances absorption and analgesic effect. A 2005 multicenter randomized trial by Diener et al. confirmed this superiority over single-substance and dual-combination preparations. However, caffeine-containing preparations carry a higher risk of medication overuse headache with frequent use, so the same “use sparingly” rule applies with greater force.
What to avoid
- Opioids (codeine, tramadol, oxycodone): Not recommended for tension headache. They carry high dependency risk, are no more effective than simple OTC analgesics for headache, and are major drivers of medication overuse headache.
- Butalbital combinations: Common in the US (e.g., Fioricet); similarly high MOH risk and no clear advantage over simpler agents. Avoid.
- Triptans (sumatriptan, rizatriptan, etc.): These are migraine-specific drugs. Clinical trials consistently show they are not effective for pure tension headache. If triptans dramatically help your headache, that is actually diagnostic evidence pointing toward migraine rather than TTH.
The medication overuse rule
The most important practical rule for episodic tension headache treatment: do not use headache-relief medication on more than 10 to 15 days per month. Exceeding this threshold — regardless of which analgesic you use — significantly increases the risk of transforming episodic headache into chronic daily headache driven by medication overuse. If you are finding yourself reaching for pain relief more than 2 to 3 days per week consistently, discuss this with your clinician. That frequency is the signal to consider preventive treatment rather than simply escalating acute treatment.
Non-medication relief for acute attacks
Several non-pharmacological measures provide meaningful relief for individual headache attacks and are particularly useful when you want to limit medication use:
- Peppermint oil applied to the forehead and temples (10% ethanol solution): A randomized trial showed efficacy comparable to acetaminophen 1000 mg for acute tension headache. Apply to forehead and temples at headache onset; avoid contact with eyes. An impressively cost-effective option.
- Cold or warm packs applied to the neck and shoulders
- Rest in a quiet, dimly lit environment
- Neck and shoulder stretching and gentle self-massage of pericranial muscles
- Correcting the posture that triggered the headache — getting up from the screen, moving around, adjusting monitor height
9. Treatment — Chronic Prevention
When tension headaches are occurring 15 or more days per month, preventive (prophylactic) treatment is indicated. The goal shifts from relieving individual attacks to reducing the baseline frequency, severity, and duration of headaches over months — and reducing the reliance on acute analgesics that is itself feeding the cycle.
First-line: Amitriptyline
Amitriptyline, a tricyclic antidepressant, is the best-evidenced preventive medication for chronic tension headache and the first choice in major international guidelines. It works on serotonin and norepinephrine pathways in the brain, likely modulating the central sensitization that underlies CTTH. Critically, the analgesic effect is independent of its antidepressant effect — amitriptyline reduces headache frequency even in patients who are not depressed, and at doses lower than those used for depression (typically 10–75 mg taken at bedtime, sometimes up to 150 mg in refractory cases).
The evidence base includes the landmark Holroyd et al. JAMA 2001 trial — a rigorous randomized controlled trial that tested amitriptyline alone, behavioral stress management therapy alone, and their combination in patients with CTTH. Key findings: amitriptyline and stress management therapy each produced significant reductions in headache frequency compared with placebo. But the combination of both together produced substantially greater improvement than either alone — a finding that established the template for modern CTTH management: pharmacological plus behavioral treatment simultaneously, not one after the other. The NNT for amitriptyline in CTTH is approximately 3, meaning one in three patients achieves meaningful reduction in headache frequency who would not have done so on placebo alone.
Common side effects: dry mouth, morning drowsiness, constipation, and weight gain. These often improve with time and are minimized by starting at a low dose (10 mg at bedtime) and titrating slowly over weeks. The bedtime dosing takes advantage of the sedating effect rather than fighting it.
Second-line options
- Mirtazapine: An alternative antidepressant with emerging evidence in CTTH, useful when amitriptyline is not tolerated or contraindicated. Also taken at bedtime; side effects include increased appetite and sedation.
- Venlafaxine: A serotonin-norepinephrine reuptake inhibitor (SNRI) with supportive evidence for tension headache prevention; fewer anticholinergic side effects than amitriptyline.
- Topiramate: Limited evidence for TTH specifically (stronger evidence in migraine prevention); occasionally used when other options have failed.
What does NOT work in chronic tension headache
Several treatments that are highly effective in migraine have specifically been tested in CTTH and shown not to work — an important point because the two headache types are sometimes confused:
- Triptans: Multiple trials confirm triptans are not effective in tension-type headache.
- Beta-blockers (propranolol, metoprolol): Well-established migraine preventives; evidence for TTH is weak and inconsistent.
- OnabotulinumtoxinA (Botox): Highly effective in chronic migraine (FDA-approved for that indication); multiple large randomized trials have specifically tested it in CTTH and found it is not more effective than placebo for tension headache. The Silberstein et al. Cephalalgia 2006 trial was one of the definitive negative studies. Patients who see “Botox for headaches” advertised should know it works specifically for chronic migraine, not for CTTH.
Addressing medication overuse: the necessary first step
If CTTH has been driven or perpetuated by medication overuse, withdrawal of the overused medication is an essential prerequisite to any preventive treatment working effectively. This is called medication overuse headache (MOH). Withdrawing the analgesic will initially worsen headaches for one to two weeks during a withdrawal period, but without this step, preventive medications are unlikely to be effective. Gradual tapering under medical supervision, often with bridge treatment during the withdrawal period, is usually recommended over abrupt cessation.
10. Non-Pharmacological Approaches
The most durable improvements in chronic tension headache come from approaches that address the underlying mechanisms — central sensitization, stress reactivity, muscle tension patterns, and sleep disruption — rather than just suppressing the symptom. Non-pharmacological treatments have excellent evidence, no medication overuse risk, and effects that persist after the active treatment period ends.
Biofeedback
Electromyographic (EMG) biofeedback is one of the best-documented behavioral treatments for tension headache. The patient receives real-time feedback (visual or auditory) about muscle tension in the pericranial and neck muscles, and learns to consciously relax those muscles. Over 8 to 12 training sessions, many patients develop lasting voluntary control over muscle tension patterns that were previously automatic and unconscious. Biofeedback reduces both headache frequency and intensity in well-designed trials, with effects comparable to drug treatment. The skill, once learned, is permanent and carries no side effects.
Progressive muscle relaxation training
Progressive muscle relaxation (PMR) — systematically tensing and then releasing muscle groups throughout the body — teaches the body to recognize and reduce baseline muscle tension. Regular practice reduces headache frequency in tension headache patients and addresses one of the core peripheral mechanisms of the condition. It can be learned from a therapist and practiced independently at home once the technique is established.
Cognitive-behavioral therapy (CBT)
Cognitive-behavioral therapy addresses the thought patterns and behavioral responses to stress that trigger and perpetuate tension headache. CBT for headache typically includes stress management skills, sleep hygiene, activity pacing, and cognitive restructuring of pain-related thought patterns such as catastrophizing. It is particularly effective in people whose tension headaches are closely coupled to psychological stress and in those with comorbid anxiety or depression. The Holroyd et al. JAMA 2001 trial demonstrated that behavioral stress management was as effective as amitriptyline when used alone, and significantly superior when combined with it.
Physical therapy and posture correction
For people whose tension headaches have a strong musculoskeletal component — particularly those with features suggesting a cervicogenic (neck-driven) component, poor posture from prolonged desk or screen work, or restricted cervical range of motion — physical therapy can be highly effective. Interventions include cervical manual therapy, trigger point treatment, stretching programs, and ergonomic correction. Improving workplace ergonomics (monitor height, chair support, keyboard position) addresses a postural root cause rather than just the symptom.
Regular aerobic exercise
Regular physical exercise is one of the most robustly supported non-pharmacological interventions for tension headache prevention. Randomized trials show that aerobic exercise 3 times per week for 30 minutes significantly reduces headache frequency and intensity in TTH patients. Exercise reduces stress reactivity, improves sleep, lowers baseline muscle tension, and has favorable effects on mood and anxiety — all of which intersect directly with the tension headache pathophysiology. The effect is dose-dependent and requires consistency to maintain, but the benefits are real and substantial.
Acupuncture
Acupuncture has a solid evidence base in tension headache prevention. A 2016 Cochrane systematic review by Linde et al. analyzed randomized trials and concluded that acupuncture is as effective as prophylactic drug treatment for CTTH, with a significantly better response than sham or placebo acupuncture. For patients who prefer to minimize medication, or who have not responded well to pharmacological prevention, acupuncture is a reasonable and evidence-supported choice — a distinction that places it above many other complementary approaches for this condition.
Sleep hygiene
Because disrupted sleep is both a trigger and a consequence of tension headache, targeted sleep hygiene is often an underutilized but high-yield intervention. Core components: consistent sleep and wake times (including weekends), limiting caffeine after midday, avoiding screens for 30 to 60 minutes before bed, keeping the bedroom cool and dark, and addressing sleep disorders such as insomnia and sleep apnea where present. Treating comorbid sleep apnea has in some cases produced meaningful reductions in headache frequency even without specific headache treatment.
Mindfulness and stress reduction
Mindfulness-based stress reduction (MBSR) programs have shown benefit in chronic pain conditions including headache. Regular mindfulness practice appears to reduce pain catastrophizing, improve emotional regulation, and modulate central pain sensitization over time. It complements CBT well and can be an accessible starting point for patients who are hesitant about more intensive behavioral therapy programs.
11. Recent Research and Advances
Tension headache research has advanced on several fronts over the past decade, though the condition still receives less funding than migraine despite its greater prevalence in the population.
The central sensitization model has been substantially strengthened by quantitative sensory testing studies showing that people with CTTH have measurably lower pain thresholds not just in the head but across the whole body — confirming that chronic tension headache is a central nervous system phenomenon, not purely a local muscle problem. This has important treatment implications: it explains why whole-body interventions like exercise, CBT, and amitriptyline work, and why purely local treatments (massage, trigger point injections) provide only temporary relief in CTTH.
The relationship between tension headache and sleep disorders has received increasing attention. Polysomnography studies show altered sleep architecture in CTTH patients, and treating comorbid insomnia or sleep apnea can produce meaningful reductions in headache frequency — sometimes even without specific headache treatment. Sleep is increasingly seen as a core therapeutic target rather than just a modifiable trigger to be listed and ignored.
Research into medication overuse headache has clarified the mechanisms by which acute analgesic overuse produces chronic headache: neuroimaging studies show changes in orbitofrontal cortex function and descending pain modulation pathways in MOH patients that partially reverse with successful withdrawal. This neurobiological understanding has helped legitimize MOH as a genuine physiological phenomenon rather than a behavioral label attached to patients who are “overusing” medication out of poor judgment.
The digital health space has produced validated smartphone apps for headache diary tracking, biofeedback delivery, and CBT skill practice, making these evidence-based tools more accessible outside of specialist clinic settings. Early trial data suggest that app-delivered behavioral interventions produce meaningful reductions in headache frequency at a fraction of the cost of in-person therapy — a significant access improvement for a condition this prevalent.
Finally, novel preventive targets are being explored. While CGRP-targeting drugs (which have transformed migraine prevention) appear less effective in TTH because of the different underlying mechanism, there is growing interest in glutamatergic and endocannabinoid pathways in central sensitization that may yield new therapeutic targets for refractory CTTH in coming years.
12. References & Research
Historical Background
The concept of “tension headache” emerged gradually through the 20th century as clinicians sought to distinguish the dull, bilateral pressure headache from the unilateral throbbing of migraine. Early theories emphasized scalp and neck muscle contraction as the primary mechanism — hence the original name “muscle contraction headache.” The International Headache Society’s first formal classification in 1988 introduced standardized diagnostic criteria, and subsequent revisions (ICHD-2 in 2004, ICHD-3 in 2018) refined the episodic and chronic subtypes. The shift toward understanding central sensitization as the key mechanism of chronic TTH in the 1990s and 2000s represented a major conceptual advance, distinguishing CTTH from simply “frequent episodic TTH” and explaining why it requires centrally-acting preventive treatments rather than just local muscle management. Bendtsen and Jensen’s 2006 review in Current Opinion in Neurology crystallized this model and has shaped treatment guidelines globally.
Key Research Papers
- Stovner LJ, Hagen K, Jensen R, et al. The global burden of headache: a documentation of headache prevalence and disability worldwide. Cephalalgia. 2007;27(3):193–210. PMID: 17381554.
- Holroyd KA, O’Donnell FJ, Stensland M, et al. Management of chronic tension-type headache with tricyclic antidepressant medication, stress management therapy, and their combination: a randomized controlled trial. JAMA. 2001;285(17):2208–2215. PMID: 11325322.
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. PMID: 29368949.
- Jensen R, Stovner LJ. Epidemiology and comorbidity of headache. Lancet Neurol. 2008;7(4):354–361. PMID: 18339350.
- Bendtsen L, Jensen R. Tension-type headache: the most common, but also the most neglected, headache disorder. Curr Opin Neurol. 2006;19(3):305–309. PMID: 16702840.
- Linde K, Allais G, Brinkhaus B, et al. Acupuncture for the prevention of tension-type headache. Cochrane Database Syst Rev. 2016;4:CD007587. PMID: 27092807.
- Bendtsen L, Evers S, Linde M, et al. EFNS guideline on the treatment of tension-type headache – report of an EFNS task force. Eur J Neurol. 2010;17(11):1318–1325. PMID: 20482606.
- Silberstein SD, Göbel H, Jensen R, et al. Botulinum toxin type A in the prophylactic treatment of chronic tension-type headache: a multicentre, double-blind, randomized, placebo-controlled parallel-group study. Cephalalgia. 2006;26(7):790–800. PMID: 16776691.
- Mathew NT. The prophylactic treatment of chronic daily headache. Headache. 2006;46(10):1552–1564. PMID: 17115983.
- Fumal A, Schoenen J. Tension-type headache: current research and clinical management. Lancet Neurol. 2008;7(1):70–83. PMID: 18093564.
- Steiner TJ, Stovner LJ, Jensen R, Uluduz D, Katsarava Z. Migraine remains second among the world’s causes of disability, and first among young women: findings from GBD2019. J Headache Pain. 2020;21(1):137. PMID: 33234101.
- Diener HC, Pfaffenrath V, Pageler L, Peil H, Aicher B. The fixed combination of acetylsalicylic acid, paracetamol and caffeine is more effective than single substances and dual combination for the treatment of headache. Cephalalgia. 2005;25(10):776–787. PMID: 16162254.
PubMed Searches
The following PubMed searches link directly to current, peer-reviewed literature on tension headache. Each opens a live PubMed query in a new tab so you can explore the most recent studies on any aspect of this condition.
- Tension headache prevalence and epidemiology
- Central sensitization in tension headache
- ICHD-3 diagnostic criteria for tension headache
- Amitriptyline for chronic tension headache prevention
- Biofeedback treatment for tension headache
- CBT for tension headache
- Acupuncture for tension headache (RCTs)
- Medication overuse (rebound) headache
- Pericranial muscle tenderness in tension headache
- Ibuprofen and aspirin efficacy in tension headache
- Aerobic exercise for tension headache prevention
- Tension headache vs migraine: differential diagnosis
Connections
- Pain & Allergy
- Migraine
- Cluster Headaches
- Chronic Pain
- Neuropathic Pain
- Complex Regional Pain Syndrome
- Trigeminal Neuralgia
- Migraine (Neurology)
- Neurology
- Willow Bark for Headache & Migraine
- All Conditions
- Headache — the general symptom page covering every headache type, red flags, and when to seek care.