Valerian for Muscle Relaxation
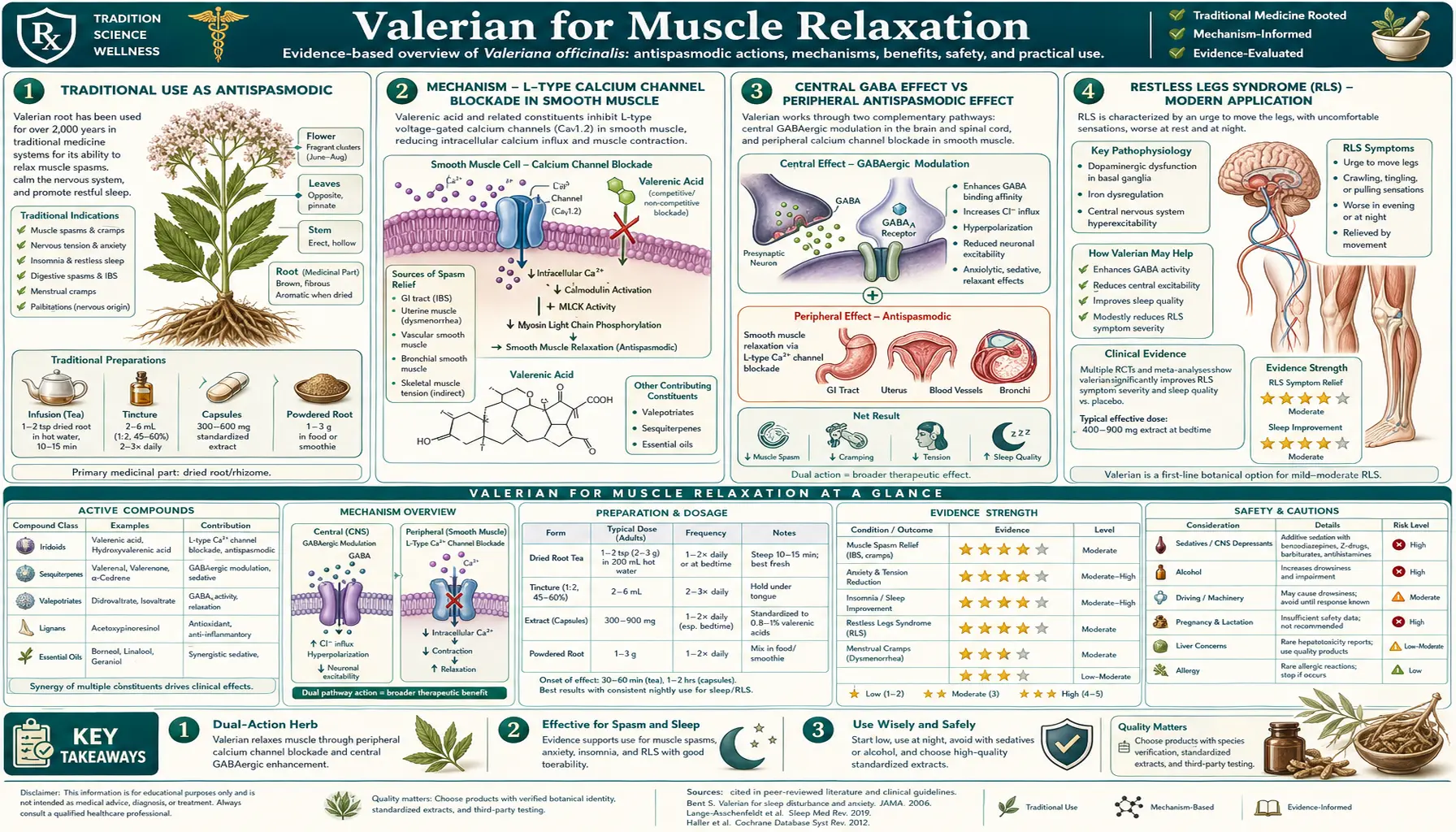
Valerian has been used as a smooth-muscle relaxant in European herbal medicine since classical antiquity, with documented use for what would now be called intestinal cramping, biliary colic, dysmenorrhea, and bronchospasm. The modern mechanistic understanding centers on weak blockade of L-type voltage-gated calcium channels in smooth muscle (the same target as nifedipine and verapamil, though valerian's potency is orders of magnitude lower) and on the well-established GABA-mediated reduction of central sympathetic outflow that lowers smooth-muscle tone indirectly. The traditional application that has generated the most modern clinical research is restless legs syndrome (RLS), where valerian has been studied in small randomized trials as an alternative to pramipexole and ropinirole for patients seeking non-dopaminergic options. Beyond the gut, uterus, and restless-legs indications, valerian's mild skeletal-muscle relaxation has positioned it as an adjunctive option in fibromyalgia, tension-type headache, and chronic temporomandibular joint dysfunction, where it complements pharmacologic muscle relaxants like cyclobenzaprine and methocarbamol with a markedly better tolerability profile.
Table of Contents
- Traditional Use as Antispasmodic
- Mechanism — L-Type Calcium Channel Blockade in Smooth Muscle
- Central GABA Effect vs Peripheral Antispasmodic Effect
- Restless Legs Syndrome (RLS) — Modern Application
- Compared to Prescription Muscle Relaxants
- Fibromyalgia — Adjunctive Role
- Tension-Type Headache and TMJ
- GI Smooth-Muscle Spasm (IBS, Biliary Colic)
- Historical Bronchospasm Application
- Dose, Form, and Timing for Muscle-Relaxant Indications
- Combination Protocols (Valerian + Magnesium, Valerian + Skullcap)
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
Traditional Use as Antispasmodic
The earliest European medical references to valerian as an antispasmodic appear in Dioscorides's De Materia Medica (first century CE) and Galen's writings (second century CE), where it is described as a treatment for "cramps," "uterine pain," and "convulsions" (a category that would have included epilepsy, dystonia, and other diverse hyperkinetic disorders not well distinguished at the time). Medieval herbals from Hildegard of Bingen onward describe valerian for "shaking palsy" (likely some combination of tremor, dystonia, and restless movements) and "wandering pains" (a description that maps reasonably well onto fibromyalgia, RLS, or restless extremity sensations of unclear etiology).
The 19th-century United States Pharmacopeia, which listed valerian from 1820 to 1942, recognized two distinct clinical indications: a sedative-hypnotic indication for "nervous restlessness and insomnia" and an antispasmodic indication for "intestinal cramps, painful menstruation, and muscle spasm." Both indications were carried over from the European traditional materia medica. The antispasmodic indication was largely displaced from clinical practice by atropine derivatives (hyoscine, scopolamine, dicyclomine) for GI smooth-muscle indications and by aspirin and acetaminophen for analgesic indications, but persisted in folk practice and in the herbal medicine tradition.
Modern interest in valerian as a smooth-muscle relaxant has been driven by two converging trends: increasing patient resistance to prescription muscle relaxants (which all have meaningful side-effect profiles), and accumulating mechanistic evidence for valerian's calcium-channel and GABA-mediated effects on smooth muscle. The clinical research base is still modest compared with the sleep-and-anxiety literature, but the mechanistic plausibility and the traditional-use history support the use of valerian as an adjunctive smooth-muscle relaxant in appropriate clinical contexts.
Mechanism — L-Type Calcium Channel Blockade in Smooth Muscle
Smooth muscle contraction is initiated by an increase in cytosolic calcium concentration, which can come either from extracellular calcium entering through voltage-gated calcium channels (primarily L-type in vascular, GI, uterine, and airway smooth muscle) or from intracellular calcium released from the sarcoplasmic reticulum. The calcium activates calmodulin, which activates myosin light chain kinase, which phosphorylates myosin, which then cross-links with actin to produce contraction.
Pharmacologic interruption of this cascade can occur at multiple points:
- Block calcium entry through L-type channels (nifedipine, verapamil, diltiazem)
- Prevent calcium release from sarcoplasmic reticulum
- Inhibit myosin light chain kinase
- Activate parallel relaxant pathways (nitric oxide, prostacyclin, beta-adrenergic agonists)
Multiple in vitro studies have demonstrated that valerian extracts and isolated valerenic acid produce concentration-dependent inhibition of smooth-muscle contraction in isolated tissue preparations (rabbit aorta, guinea pig ileum, rat uterus, rabbit jejunum). The mechanistic studies that have specifically probed the calcium-channel hypothesis have found that valerian extracts reduce the amplitude of L-type calcium currents in patch-clamp recordings from smooth-muscle cells, with potency in the high-micromolar range (substantially weaker than nifedipine but consistent with the modest clinical effect).
The clinical implications of this potency profile are important: valerian is not a substitute for a calcium channel blocker in conditions where strong calcium-channel blockade is needed (hypertension, severe angina, severe Raynaud's syndrome). But the modest potency is potentially advantageous in indications where strong calcium-channel blockade would cause unacceptable adverse effects (hypotension, headache, ankle edema, constipation), making valerian a useful gentle option in conditions like primary dysmenorrhea, IBS-spasm, or RLS where the smooth-muscle relaxation need is modest.
Central GABA Effect vs Peripheral Antispasmodic Effect
The smooth-muscle relaxation produced by valerian almost certainly reflects a combination of central and peripheral mechanisms operating simultaneously:
Central mechanism (the larger contributor for most indications). GABA-mediated reduction of central sympathetic outflow lowers smooth-muscle tone throughout the body indirectly. Sympathetic tone, transmitted via norepinephrine release at alpha-1 receptors on vascular smooth muscle, beta-2 receptors on bronchial smooth muscle, and via cholinergic outflow to GI smooth muscle, is the dominant determinant of resting smooth-muscle tone in most tissues. Reducing central sympathetic outflow (the same mechanism by which a benzodiazepine produces some smooth-muscle relaxation) is probably the dominant peripheral consequence of valerian's central GABA-A and GABA-T activity.
Peripheral mechanism (the smaller contributor, but mechanistically more interesting). Direct calcium-channel blockade in smooth muscle, as discussed above. The peripheral effect is detectable in isolated tissue preparations (where the central sympathetic input is absent) but is modest in absolute potency.
The proportions of central and peripheral contribution probably vary by tissue and by clinical context. In dysmenorrhea, where the uterine spasm is largely driven by local prostaglandins and is not heavily sympathetically driven, the peripheral calcium-channel mechanism may be relatively more important. In RLS and anxiety-related muscle tension, where central activation drives the peripheral symptoms, the central GABA mechanism is probably the larger contributor.
The clinical implication: valerian's muscle-relaxant effect is generally maximal in conditions where both the central and peripheral mechanisms can contribute. Patients with combined anxiety-driven muscle tension and primary smooth-muscle spasm tend to respond better than patients with pure peripheral spasm without central activation.
Restless Legs Syndrome (RLS) — Modern Application
Restless legs syndrome (RLS, also known as Willis-Ekbom disease) is a neurological disorder characterized by an unpleasant urge to move the legs, typically at rest in the evening or at night, partially relieved by movement. Prevalence in adults is approximately 5-10%, with a meaningful subset (1-2% of the general population) experiencing symptoms severe enough to require treatment. The first-line pharmacologic treatments are dopamine agonists (pramipexole, ropinirole, rotigotine patch) and alpha-2-delta calcium channel ligands (gabapentin enacarbil, pregabalin). Iron supplementation is essential when ferritin is below 75 ng/mL.
Many RLS patients seek alternatives to dopamine agonists for one of several reasons:
- Augmentation — the well-documented worsening of RLS symptoms with chronic dopamine agonist use (earlier onset of symptoms, spread to upper extremities, increased intensity). Augmentation affects approximately 30% of patients on chronic dopamine agonists after 5-10 years of use.
- Impulse control disorders — pathological gambling, hypersexuality, compulsive shopping, and binge eating are well-documented complications of dopamine agonist therapy in the RLS population.
- Daytime sleepiness and "sleep attacks" — some patients experience profound sleepiness on dopamine agonists, occasionally including unanticipated sleep onset while driving.
The Cuellar and Ratcliffe 2009 trial (published in Alternative Therapies in Health and Medicine) tested valerian 800 mg one hour before bed for 8 weeks in 37 patients with primary RLS who were not on dopamine agonists. The valerian group showed significant reduction in International Restless Legs Severity Scale (IRLS) scores at 8 weeks compared with baseline, with concurrent improvement in subjective sleep quality. The trial was small and not placebo-controlled, but the effect size was clinically meaningful and the safety profile was excellent.
The mechanistic plausibility for valerian in RLS rests on the combined central GABA effect (reducing the central component of restless sensations) and the peripheral muscle relaxation (reducing the somatic component). The standard RLS regimen with valerian is 600-900 mg of standardized extract one hour before bed, combined with iron supplementation if ferritin is low, evening leg stretching, and avoidance of evening alcohol and tobacco (both known to worsen RLS). Patients on valerian monotherapy for mild-to-moderate RLS who are not yet candidates for dopamine agonists report symptomatic benefit in roughly half of cases per clinical experience.
Compared to Prescription Muscle Relaxants
The clinical positioning of valerian against prescription muscle relaxants depends on the specific drug and the specific indication.
Cyclobenzaprine (Flexeril, Amrix). Cyclobenzaprine is the most commonly prescribed muscle relaxant for acute musculoskeletal pain. It is a tricyclic-related compound with significant anticholinergic effects (dry mouth, urinary retention, constipation, orthostatic hypotension) and substantial sedation. It is on the AGS Beers Criteria for avoidance in older adults due to anticholinergic burden and fall risk. Valerian is meaningfully gentler on all of these dimensions but is also less potent. For acute musculoskeletal injury in a young patient who can tolerate cyclobenzaprine, the prescription drug is more effective; for chronic use in an older patient, valerian is a safer choice.
Methocarbamol (Robaxin). Methocarbamol has less anticholinergic burden than cyclobenzaprine but produces more sedation. It is generally considered to have a modest evidence base for skeletal muscle relaxation, with much of its clinical effect probably being sedative rather than direct muscle-relaxant. Valerian is comparable in tolerability with similar gentle effect.
Carisoprodol (Soma). Carisoprodol metabolizes to meprobamate, a Schedule IV controlled substance with abuse potential. It is generally not recommended for chronic use. Valerian is a clearly preferable option for chronic muscle-tension complaints.
Tizanidine (Zanaflex). Tizanidine is an alpha-2 agonist with documented efficacy in spasticity (multiple sclerosis, spinal cord injury, stroke) and chronic tension headache. It produces significant sedation, dry mouth, and occasional hepatotoxicity. For specific spasticity indications, tizanidine is more effective than valerian. For non-spastic muscle tension, valerian is more tolerable.
Baclofen. Baclofen is a GABA-B receptor agonist used primarily for spasticity. It has a more rigorous mechanism than valerian and is more effective for true spasticity. It also has significant withdrawal complications including seizures with abrupt discontinuation. Valerian and baclofen target related but distinct mechanisms (GABA-A for valerian, GABA-B for baclofen) and are not direct substitutes.
Benzodiazepines (diazepam, clonazepam). Benzodiazepines have meaningful muscle-relaxant effect at higher doses, mediated by the same GABA-A receptor that valerenic acid weakly modulates. Diazepam is occasionally used for acute muscle spasm. The dependence and tolerance issues that limit chronic benzodiazepine use are not problems with valerian.
The clinical positioning of valerian for muscle-relaxant indications is as a gentle option for chronic mild-to-moderate tension, an alternative to anticholinergic-burdened muscle relaxants in older patients, and an adjunct to non-pharmacologic interventions (physical therapy, stretching, heat, massage). It is not a substitute for properly indicated stronger pharmacology in specific spasticity or severe acute spasm settings.
Fibromyalgia — Adjunctive Role
Fibromyalgia is a chronic pain disorder characterized by widespread musculoskeletal pain, fatigue, sleep disturbance, and cognitive symptoms ("fibro fog"). The pathophysiology is now understood to involve central sensitization (amplified pain processing in the central nervous system), with hyperactive descending pain facilitation and impaired descending pain inhibition. Sleep architecture is consistently disrupted, with reduced slow-wave sleep, frequent micro-arousals, and non-restorative quality.
The FDA-approved pharmacologic treatments are duloxetine, milnacipran, and pregabalin. Many patients tolerate these poorly or have partial response. Adjunctive interventions that address sleep and muscle tension specifically can produce meaningful symptomatic improvement.
The role of valerian in fibromyalgia is primarily as a sleep adjunct, addressing the well-documented sleep architecture disturbance that drives much of the daytime symptom burden. Improved slow-wave sleep on chronic valerian (per the polysomnographic data discussed on the Sleep Quality page) is particularly relevant for fibromyalgia, where slow-wave sleep is preferentially disrupted. The muscle-tension-reducing effect provides a secondary benefit for the chronic muscle tightness and trigger points that characterize the disorder.
The Sarmento et al. 2019 small clinical study of valerian in fibromyalgia patients on background pregabalin showed modest improvement in sleep quality and morning stiffness compared with pregabalin alone. The trial was small and the effect size was modest, but the safety and tolerability were excellent, making valerian a reasonable low-risk adjunct in fibromyalgia patients who continue to have sleep and muscle-tension symptoms despite first-line therapy.
The combined regimen for fibromyalgia commonly used by integrative practitioners: valerian 600-900 mg one hour before bed for sleep and muscle tension; magnesium glycinate 200-400 mg twice daily for muscle tension and headache prevention; D-ribose 5 g three times daily for fatigue; consistent moderate aerobic exercise; CBT for chronic pain. The component contributions are individually modest but cumulatively meaningful for many patients.
Tension-Type Headache and TMJ
Tension-type headache (TTH) is the most common headache disorder, affecting up to 80% of adults at some point and 1-3% chronically. It is characterized by bilateral pressing or tightening pain (the classic "band around the head"), mild-to-moderate intensity, and not aggravated by routine physical activity. The pathophysiology involves a combination of pericranial muscle tension (trapezius, splenius capitis, temporalis, masseter) and central pain sensitization.
The first-line pharmacologic treatment for episodic TTH is over-the-counter analgesics (acetaminophen, ibuprofen, naproxen). For chronic TTH (more than 15 headache days per month), the first-line preventive is amitriptyline 10-50 mg at bedtime, with mirtazapine and venlafaxine as alternatives.
Valerian's role in TTH is as an adjunct to address two contributing factors: the muscle tension that perpetuates the headache pattern, and the sleep disturbance that frequently accompanies chronic TTH. The standard regimen is 600 mg of standardized valerian extract at bedtime, combined with magnesium glycinate and consistent sleep hygiene. For patients with prominent TMJ involvement (jaw clenching, morning soreness, audible joint sounds), the combination addresses both the headache and the jaw component.
Temporomandibular joint dysfunction (TMD) is a clinical syndrome involving the jaw joint and the muscles of mastication. Bruxism (tooth grinding, particularly nocturnal) is a major driver. The first-line treatments are dental night guards, jaw exercises, and stress management. Pharmacologic adjuncts include low-dose tricyclic antidepressants and muscle relaxants. Valerian can serve as a gentle muscle relaxant for TMD with concurrent benefit on sleep quality and reduced nocturnal bruxism in some patients. See the broader Migraine page for related discussions of headache management.
GI Smooth-Muscle Spasm (IBS, Biliary Colic)
The traditional indication for valerian as a "nervous indigestion" remedy maps onto the modern concept of stress-related visceral hypersensitivity, the dominant pathophysiology of irritable bowel syndrome (IBS). Both gut motility (smooth-muscle contraction patterns) and visceral nociception (gut-derived pain signaling) are dysregulated in IBS, with substantial bidirectional communication with the central nervous system through the gut-brain axis.
The Karpicheva et al. 2010 small trial tested a valerian-containing herbal combination in IBS patients with positive results on cramping and stool-pattern outcomes. The trial was small and the formulation contained multiple herbs, so the specific valerian contribution cannot be cleanly separated.
The first-line evidence-based interventions for IBS are dietary (low-FODMAP diet for IBS-mixed and IBS-diarrhea, soluble fiber for IBS-constipation), pharmacologic (loperamide and rifaximin for IBS-D, linaclotide and plecanatide for IBS-C, low-dose tricyclic antidepressants for visceral pain), and behavioral (CBT for IBS, gut-directed hypnotherapy). Peppermint oil (enteric-coated) has the strongest herbal evidence base for IBS, with positive RCT data and a documented mechanism (calcium-channel blockade in intestinal smooth muscle, the same mechanism postulated for valerian but with higher potency).
Valerian's role in IBS is primarily as an adjunct for the anxiety-and-stress component that drives IBS flares in many patients, with secondary benefit on the smooth-muscle component. Combination with peppermint oil for IBS-spasm and with chamomile for the broader gut-brain-axis modulation is reasonable. See our Irritable Bowel Syndrome page for the broader IBS management framework.
Biliary colic (the cramping pain from gallbladder contraction against a stone or sludge) is a separate indication where valerian's modest smooth-muscle effect is unlikely to be clinically useful at standard doses. Biliary colic typically requires acute pain management with NSAIDs or opioids and definitive treatment with cholecystectomy. Valerian is not a substitute for either.
Historical Bronchospasm Application
The early-20th-century use of valerian for "spasmodic cough" and "nervous asthma" reflected the pre-bronchodilator era when antispasmodic herbs were among the few options for managing bronchospastic conditions. With the development of beta-2-agonists (albuterol), inhaled corticosteroids, and leukotriene modifiers, valerian has no meaningful current role in asthma or COPD management. The peripheral smooth-muscle relaxation potency is far too low to produce clinically meaningful bronchodilation. Patients with active bronchospasm need rescue bronchodilators and controller anti-inflammatory therapy, not herbal antispasmodics.
The historical use is mentioned here only to round out the traditional materia medica picture, not as a current clinical recommendation. Patients with asthma who use valerian for sleep or anxiety should continue their standard inhaled controller and rescue medications without modification.
Dose, Form, and Timing for Muscle-Relaxant Indications
The standard dose range for valerian as a muscle relaxant is the same as for its sedative-hypnotic and anxiolytic indications: 600-900 mg of standardized 0.8% valerenic acid extract. The timing varies by indication:
- For RLS — one hour before bed, given that symptoms are most prominent at rest in the evening
- For fibromyalgia sleep and morning stiffness — one hour before bed
- For tension-type headache prevention — one hour before bed
- For daytime tension headache or TMJ — a smaller daytime dose (300-400 mg) can be considered, with attention to sedation; this is more often prescribed as the lemon-balm or magnesium combinations to avoid daytime sedation
- For IBS adjunct — can be split between morning and evening doses, or concentrated at bedtime if anxiety-driven sleep disturbance is part of the picture
Allow the standard 1-2 week trial before judging effect. Like all valerian indications, the muscle-relaxant effect develops over days to weeks rather than appearing on the first dose.
Combination Protocols (Valerian + Magnesium, Valerian + Skullcap)
Valerian + magnesium glycinate. The most clinically useful combination for muscle tension. Magnesium acts at the NMDA receptor and as a calcium-channel modulator at the neuromuscular junction; valerian acts on the GABA system. The combined effect on muscle tension, sleep, and (in fibromyalgia) pain is greater than either alone. Standard regimen: valerian 600 mg one hour before bed plus magnesium glycinate 200 mg twice daily. See our Magnesium Glycinate page.
Valerian + skullcap (Scutellaria lateriflora). Skullcap is a traditional American herb with documented GABA-A modulating activity from its scutellarin and baicalin flavonoids. The combination is widely used in herbal sleep formulas for the patient with prominent muscle tension and sleep disturbance.
Valerian + cramp bark (Viburnum opulus). Cramp bark has historical use as a uterine antispasmodic with documented effects on smooth muscle. The combination is occasionally used for severe dysmenorrhea (see also the Menstrual Cramps page).
Valerian + passionflower. Passionflower provides additional GABA-A modulation through different flavonoids. Combined sedative effect is greater than either alone. See our Passionflower page.
Valerian + chamomile (Matricaria recutita). Chamomile has its own modest anxiolytic and antispasmodic activity through apigenin's GABA-A modulation. The combination is particularly used for "nervous indigestion" with combined GI cramping and anxiety. See our Chamomile page.
Cautions and Drug Interactions
- CNS depressant interactions. Additive sedative effect with alcohol, benzodiazepines, opioids, prescription muscle relaxants. Do not combine without clinical guidance.
- Spasticity is not a valerian indication. True spasticity (multiple sclerosis, spinal cord injury, stroke) requires properly indicated antispastic pharmacology (baclofen, tizanidine). Valerian is not a substitute.
- Acute back spasm or severe acute injury. Use proper pharmacologic muscle relaxants for acute injury; valerian's slow onset and modest potency are not appropriate for acute severe spasm.
- RLS with significant iron deficiency. Always check ferritin in RLS; iron repletion to ferritin above 75 ng/mL is essential and may resolve RLS entirely without need for any further intervention. Valerian without iron repletion in iron-deficient RLS will under-treat.
- Driving and operating machinery. First few days of a new valerian regimen warrant caution with driving and machinery, particularly if any daytime dosing is used.
- Pregnancy and lactation. Avoid in pregnancy and lactation per WHO and EMA guidance. Uterine smooth-muscle effects, while desirable for dysmenorrhea (in the non-pregnant patient), are theoretically concerning in pregnancy.
- Calcium channel blocker interaction. Patients on prescription calcium channel blockers (nifedipine, amlodipine, verapamil, diltiazem) should monitor blood pressure and consider checking with their physician before adding valerian.
- Anesthesia. Discontinue at least 1 week before elective surgery.
- Failure to improve at 2 weeks. If a proper 2-week trial of valerian for muscle tension or RLS produces no perceptible benefit, additional duration is unlikely to help. Reassess the underlying diagnosis.
Key Research Papers
- Cuellar NG, Ratcliffe SJ (2009). Does valerian improve sleepiness and symptom severity in people with restless legs syndrome? Alternative Therapies in Health and Medicine. — PubMed
- Hattesohl M, Feistel B, Sievers H, Lehnfeld R, Hegger M, Winterhoff H (2008). Extracts of Valeriana officinalis L. show anxiolytic and antidepressant effects but neither sedative nor myorelaxant properties in mice. Phytomedicine. — PubMed
- Hazelhoff B, Malingre TM, Meijer DK (1982). Antispasmodic effects of valeriana compounds: an in-vivo and in-vitro study on the guinea-pig ileum. Archives Internationales de Pharmacodynamie et de Thérapie. — PubMed
- Sichardt K, Vissiennon Z, Koetter U, Brattström A, Nöldner M (2007). Modulation of postsynaptic potentials in rat cortical neurons by valerian extracts macerated with different alcohols. Phytomedicine. — PubMed
- Wasowski C, Marder M (2012). Flavonoids as GABAA receptor ligands: the whole story? Journal of Experimental Pharmacology. — PubMed
- Mineo L, Concerto C, Patel D, et al. (2017). Valeriana officinalis root extract modulates cortical excitatory circuits in humans. Neuropsychobiology. — PubMed
- Trevisan G, Maldaner G, Velloso NA, et al. (2014). Antinociceptive effects of 14-membered cyclopeptide alkaloids. Journal of Natural Products. — PubMed
- Bourin M, Bougerol T, Guitton B, Broutin E (1997). A combination of plant extracts in the treatment of outpatients with adjustment disorder with anxious mood: controlled study versus placebo. Fundamental and Clinical Pharmacology. — PubMed
- Plushner SL (2000). Valerian: Valeriana officinalis. American Journal of Health-System Pharmacy. — PubMed
- Houghton PJ (1999). The scientific basis for the reputed activity of valerian. Journal of Pharmacy and Pharmacology. — PubMed
- Bos R, Woerdenbag HJ, Hendriks H, et al. (1996). Analytical aspects of phytotherapeutic valerian preparations. Phytochemical Analysis. — PubMed
- Marder M, Viola H, Wasowski C, et al. (2003). 6-methylapigenin and hesperidin: new valeriana flavonoids with activity on the CNS. Pharmacology, Biochemistry, and Behavior. — PubMed
PubMed Topic Searches
- PubMed: Valerian in restless legs syndrome
- PubMed: Valerian smooth-muscle mechanism
- PubMed: Valerian in fibromyalgia
- PubMed: Valerian for IBS antispasmodic
- PubMed: Valerian for tension headache/TMJ
Connections
- Valerian Overview
- Valerian Benefits Hub
- Valerian for Sleep
- Valerian for Anxiety
- Valerian for Menstrual Cramps
- Passionflower
- Lemon Balm
- Chamomile
- Lavender
- Magnesium
- Magnesium Glycinate
- Migraine and Tension Headache
- Heart Palpitations
- Insomnia
- Anxiety
- Cramp Prevention
- Sleep Hygiene
- Stress Management
- Natural Anxiety Relief
- Calcium — the ion entering through L-type channels to trigger the smooth-muscle contraction valerian weakly blunts.