Valerian for Menstrual Cramps
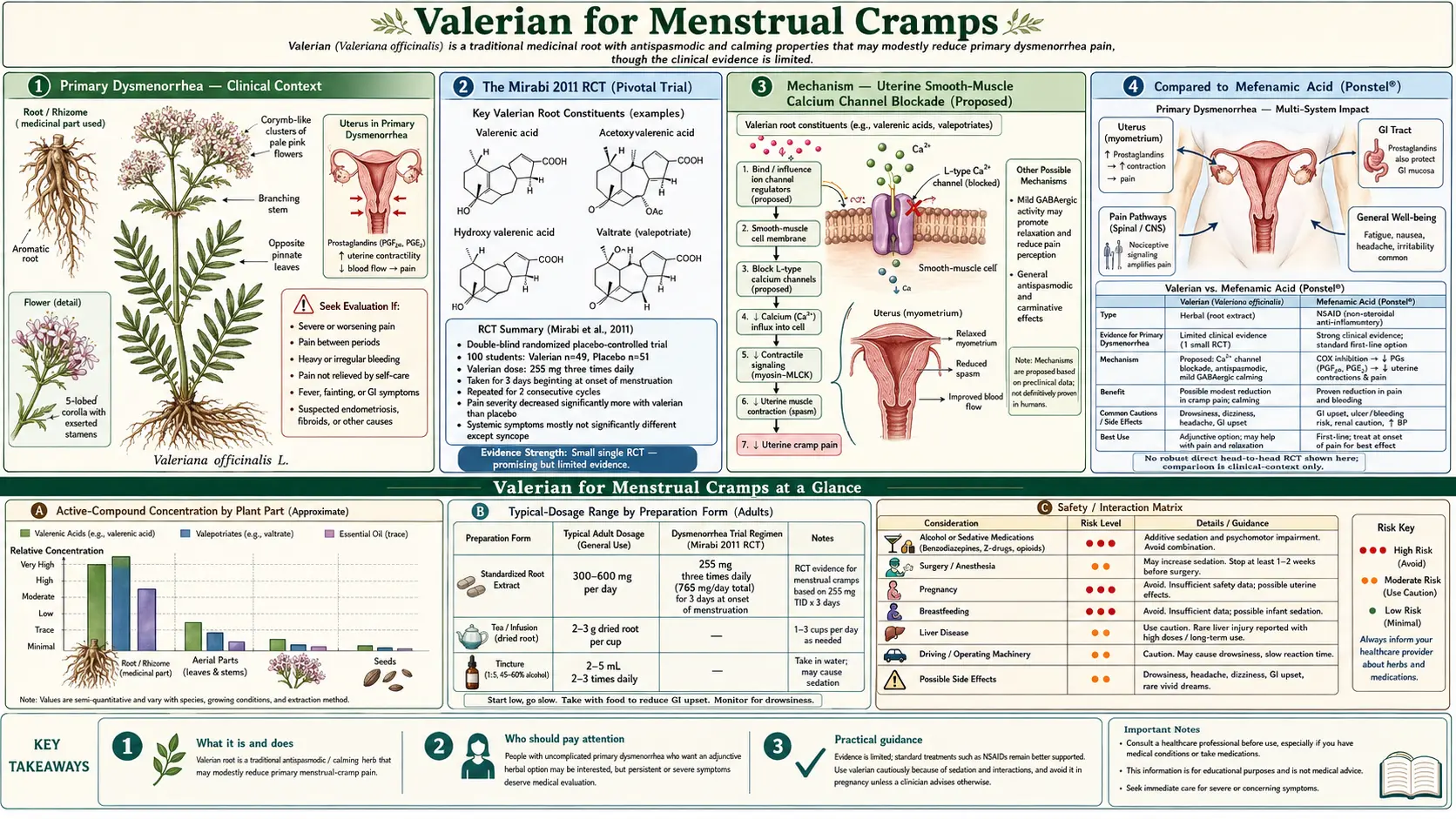
Primary dysmenorrhea — painful menstrual cramps without underlying pelvic pathology — affects roughly half of menstruating women and is severe enough to disrupt daily activity in 10-15%. The first-line pharmacologic treatment is NSAIDs (ibuprofen, naproxen, mefenamic acid), which work by inhibiting cyclooxygenase-mediated prostaglandin synthesis in the endometrium. Valerian has emerged from the Iranian, Turkish, and broader Middle Eastern gynecology research as a tolerable adjunct with documented benefit on cramp severity and the broader systemic symptoms of dysmenorrhea (nausea, fatigue, headache, mood). The pivotal trial is Mirabi et al. 2011 (International Journal of Gynaecology and Obstetrics), which compared valerian 255 mg three times daily with placebo over two menstrual cycles in 100 students with primary dysmenorrhea and found significant reduction in pain severity and systemic symptom burden. The proposed mechanism is uterine smooth-muscle calcium-channel blockade (the same final pathway as nifedipine, which has been used off-label for severe dysmenorrhea, though with substantially higher potency and worse tolerability than valerian). The clinical positioning is as a tolerable adjunct to or partial substitute for mefenamic acid in patients who cannot tolerate full NSAID dosing, who have NSAID-induced GI symptoms, or who prefer plant-based options. This page synthesizes the published evidence, the proposed mechanism, the comparison with mefenamic acid and other first-line treatments, and the practical dosing and timing for the dysmenorrhea indication.
Table of Contents
- Primary Dysmenorrhea — Clinical Context
- The Mirabi 2011 RCT (Pivotal Trial)
- Mechanism — Uterine Smooth-Muscle Calcium Channel Blockade
- Compared to Mefenamic Acid (Ponstel)
- Compared to Ibuprofen, Naproxen, and Other NSAIDs
- Compared to Oral Contraceptives
- The Iranian and Turkish Gynecology Research Tradition
- Systemic Symptoms (Nausea, Fatigue, Headache, Mood)
- Combination Protocols (Valerian + Chamomile, Valerian + Fennel, Valerian + Ginger)
- Dosing and Timing for Dysmenorrhea
- Endometriosis and Secondary Dysmenorrhea
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
Primary Dysmenorrhea — Clinical Context
Dysmenorrhea is the medical term for painful menstrual periods. Primary dysmenorrhea is painful menstruation in the absence of identifiable pelvic pathology — the pain is generated by the normal physiologic processes of menstruation, primarily uterine contractions stimulated by prostaglandin release from the shedding endometrium. Secondary dysmenorrhea is painful menstruation due to an identifiable underlying condition (endometriosis, adenomyosis, fibroids, pelvic inflammatory disease, intrauterine device complications).
Primary dysmenorrhea typically begins within 6-12 months of menarche, once ovulatory cycles establish, and follows a characteristic pattern: cramping pain in the lower abdomen and back, beginning hours before or at the start of menstrual flow, peaking in the first 24-48 hours, and resolving within 2-3 days. Associated systemic symptoms (nausea, vomiting, diarrhea, headache, fatigue, dizziness) reflect the systemic effects of prostaglandin release.
The pathophysiology is dominated by prostaglandin F2-alpha (PGF2a) and prostaglandin E2 (PGE2), produced in the endometrium during menstruation from arachidonic acid via cyclooxygenase enzymes. PGF2a is a potent vasoconstrictor and uterine contractant; PGE2 contributes to inflammation and pain sensitization. Women with severe primary dysmenorrhea have measurably higher endometrial prostaglandin production than women with mild or no dysmenorrhea, providing the basis for the dominance of NSAIDs (cyclooxygenase inhibitors) in pharmacologic management.
First-line evidence-based treatments per ACOG (American College of Obstetricians and Gynecologists) and similar international guidelines:
- NSAIDs (ibuprofen 400-600 mg every 6 hours, naproxen 250-500 mg every 12 hours, mefenamic acid 500 mg every 6 hours) — the most effective single class
- Combined oral contraceptives or other hormonal suppression of ovulation
- Heat application (heating pads, hot water bottles)
- Exercise (moderate aerobic exercise has small but real effect)
- TENS (transcutaneous electrical nerve stimulation) — modest evidence
Adjunctive interventions with smaller but real evidence bases include omega-3 fatty acids, magnesium, thiamine, vitamin B6, and the herbal interventions including valerian, chamomile, fennel, ginger, and dill that this page and related pages cover.
The Mirabi 2011 RCT (Pivotal Trial)
The Mirabi et al. 2011 trial, published in International Journal of Gynaecology and Obstetrics, is the foundational and most-cited randomized controlled trial of valerian for primary dysmenorrhea. Parvaneh Mirabi and colleagues at Babol University of Medical Sciences in Iran enrolled 100 female students with documented primary dysmenorrhea and randomized them to one of two arms: valerian root capsules (255 mg three times daily, totaling 765 mg/day, given for three days starting from the onset of menstruation) or matching placebo, over two consecutive menstrual cycles.
The primary outcomes were:
- Pain severity, measured by visual analog scale (VAS) on the worst day of each cycle
- Severity of systemic manifestations, measured by a composite score covering nausea, vomiting, syncope, fatigue, diarrhea, and mood disturbance
Results at the end of the second cycle:
- Pain severity — the valerian group had significantly lower VAS pain scores compared with placebo. The effect was clinically meaningful (approximately 1.5-2 points on a 10-point VAS) and statistically significant (p<0.05).
- Systemic manifestations — the composite systemic score was significantly lower in the valerian group, with the largest individual effects on syncope (lightheadedness) and mood disturbance.
- Side effects — no significant difference between valerian and placebo for any adverse event. No serious adverse events.
The trial established that a relatively short course of valerian (three days per cycle, starting at menses onset) at a moderate dose (765 mg/day in divided doses) produces measurable benefit on both pain and systemic symptoms in primary dysmenorrhea. This is one of the cleaner positive RCTs in the valerian clinical literature, with a well-defined population, an objective outcome measure, a reasonable dose, and a clinically meaningful effect size.
The trial does have limitations: single-center, modest sample size, no head-to-head comparison with mefenamic acid or other NSAID, no objective measure of uterine contractility (such as intrauterine pressure recording), no biochemical correlates (such as endometrial prostaglandin levels). A larger multi-center replication with active comparator would strengthen the evidence base. Such a replication has not been published, though several follow-up Iranian and Turkish studies have extended the framework.
Mechanism — Uterine Smooth-Muscle Calcium Channel Blockade
The proposed mechanism for valerian's analgesic effect in dysmenorrhea is uterine smooth-muscle relaxation via L-type voltage-gated calcium channel blockade, the same mechanism discussed in detail on the Muscle Relaxation page. The uterus, like the gut, contains abundant smooth muscle with L-type calcium channels mediating excitation-contraction coupling.
The mechanistic plausibility is supported by several lines of evidence:
- In vitro tissue studies — isolated rat uterus preparations (the standard pharmacologic model) show concentration-dependent inhibition of spontaneous and oxytocin-induced contractions by valerian extracts and isolated valerenic acid. The potency is modest (high-micromolar range) but the effect is consistent and dose-dependent.
- Clinical analogy with prescription calcium channel blockers — nifedipine, a potent L-type calcium channel blocker primarily marketed for hypertension and Raynaud's syndrome, has documented off-label use in severe dysmenorrhea and in preterm labor (tocolysis). The same mechanism produces both clinical effects. The tolerability of nifedipine is poor (headache, flushing, ankle edema, reflex tachycardia), which limits its use for dysmenorrhea despite documented efficacy. Valerian's much weaker calcium-channel effect avoids these adverse effects while providing modest benefit.
- Effect on systemic symptoms — the systemic symptoms of dysmenorrhea (nausea, syncope, fatigue) are largely mediated by prostaglandin-driven sympathetic dysregulation and visceral pain signaling. Valerian's central anxiolytic and sympatholytic effects provide a plausible mechanism for the documented benefit on systemic symptoms, in addition to the direct uterine effect.
Secondary mechanisms that may contribute include:
- Central pain modulation via GABA-A — valerenic acid's GABA-A modulation provides central pain reduction independent of the uterine mechanism
- Anxiolytic effect on pain perception — reduction of anxiety amplification of pain, particularly in patients with anticipatory anxiety about menstrual pain
- Sleep improvement — better sleep during menses (often disrupted by pain) reduces pain sensitization the following day
- Possible direct prostaglandin modulation — some in vitro evidence suggests valerian extracts may have weak effects on cyclooxygenase activity, though this is not a primary mechanism and the potency is far below NSAIDs
The clinical interpretation: valerian's modest analgesic effect in dysmenorrhea is mechanistically plausible and operates through multiple parallel low-potency pathways. It is unlikely to fully replace NSAIDs in moderate-to-severe primary dysmenorrhea but is appropriate as an adjunct or as a partial substitute in patients with NSAID intolerance.
Compared to Mefenamic Acid (Ponstel)
Mefenamic acid (Ponstel in the US, Ponstan in much of the world) is a fenamate NSAID that has been specifically promoted for primary dysmenorrhea since the 1970s. It is one of the most-prescribed dysmenorrhea-specific medications globally, particularly in countries where the Iranian, Turkish, and broader Middle Eastern medical traditions dominate. The standard dose is 500 mg every 6 hours starting at the onset of menstrual flow.
Mefenamic acid's pharmacology is unusual among NSAIDs: in addition to the standard cyclooxygenase inhibition shared with all NSAIDs, it has been reported to have additional activity blocking prostaglandin receptors at the target tissue, which may explain its particular reputation for dysmenorrhea efficacy. Clinical trials consistently show mefenamic acid producing larger reductions in dysmenorrhea pain than equivalent NSAID doses of ibuprofen or naproxen.
The downside is the side effect profile: mefenamic acid produces more GI symptoms (nausea, dyspepsia, diarrhea) than other NSAIDs, particularly when used for more than 1-2 days. Long-term use is associated with renal effects (interstitial nephritis), and pediatric use has been associated with rare cases of fatal hemolytic anemia.
The Mirabi trial did not directly compare valerian with mefenamic acid, but follow-up trials in the Iranian gynecology literature have made the comparison. The Khodadost et al. and similar trials suggest that valerian produces approximately 70-80% of the analgesic effect of mefenamic acid in primary dysmenorrhea, with substantially better tolerability. The clinical decision algorithm that has emerged in the Iranian and Turkish practice setting:
- Mild dysmenorrhea — valerian monotherapy (765 mg/day) often sufficient
- Moderate dysmenorrhea — mefenamic acid first-line; valerian for patients with GI intolerance to NSAIDs
- Severe dysmenorrhea — mefenamic acid as first-line; valerian as adjunct to allow lower NSAID dose; consider hormonal suppression as alternative
- Dysmenorrhea with prominent systemic symptoms — combination of mefenamic acid for pain plus valerian for systemic symptoms (mood, sleep, nausea)
In Western practice the algorithm typically uses ibuprofen or naproxen rather than mefenamic acid (which is less commonly prescribed in the US), but the principles transfer.
Compared to Ibuprofen, Naproxen, and Other NSAIDs
Ibuprofen and naproxen are the most-prescribed NSAIDs globally and the first-line treatment for primary dysmenorrhea in most Western practice settings. Standard regimens:
- Ibuprofen — 400-600 mg every 6 hours starting at onset of menses or, preferably, in anticipation 1-2 days before predicted menses
- Naproxen — 250-500 mg every 12 hours (the longer half-life reduces dosing burden)
- Diclofenac — 50 mg every 8 hours; effective but with higher cardiovascular risk in chronic use
- Celecoxib (COX-2 selective) — 200 mg every 12 hours; useful in patients with NSAID-related GI sensitivity, but cardiovascular risk profile limits chronic use
The valerian-vs-NSAID comparison for dysmenorrhea has the same general shape as the mefenamic acid comparison: NSAIDs produce larger acute analgesic effect, but valerian has substantially better tolerability and avoids the GI, renal, and cardiovascular concerns that limit chronic NSAID use.
The clinical situations where valerian is most useful as a substitute or substantial partial substitute for NSAIDs:
- Patients with NSAID-related dyspepsia, gastritis, or PUD history
- Patients on anticoagulation (warfarin, DOACs) where NSAID-induced bleeding risk is concerning
- Patients with chronic kidney disease where chronic NSAID use is contraindicated
- Patients with NSAID allergy or AERD (aspirin-exacerbated respiratory disease)
- Patients who explicitly prefer plant-based or non-pharmacologic options
- Adolescent patients whose parents prefer to avoid early establishment of regular NSAID use
The clinical situations where valerian is generally inadequate as monotherapy and where NSAIDs should be primary:
- Moderate-to-severe primary dysmenorrhea (VAS pain >6)
- Dysmenorrhea associated with documented endometriosis or adenomyosis
- Acute pain rescue (valerian's slow onset is not useful for acute pain)
- Dysmenorrhea that has been previously well-controlled with NSAIDs without intolerance
Compared to Oral Contraceptives
Combined oral contraceptives (estrogen-progestin pills) are highly effective for primary dysmenorrhea, typically reducing pain severity by 70-80% through suppression of ovulation and thinning of endometrial prostaglandin production. They are appropriate for patients who also desire contraception or who have severe dysmenorrhea not adequately controlled by NSAIDs.
Valerian and oral contraceptives are complementary rather than competitive in clinical practice. Patients on OCPs generally have minimal dysmenorrhea and do not need valerian for this indication. Patients who cannot tolerate OCPs (smokers over 35, history of migraine with aura, history of VTE, breastfeeding) often use valerian and NSAID combinations as the alternative approach.
For patients on OCPs who continue to experience breakthrough dysmenorrhea (perhaps 10-15% of OCP users), valerian is a reasonable adjunct. The combination is well-tolerated and the mechanisms are non-overlapping (OCP suppresses ovulation and endometrial development; valerian relaxes uterine smooth muscle and modulates central pain perception).
Continuous (extended-cycle) OCPs that eliminate the placebo week and skip menstrual bleeding entirely have become the modern preferred approach for severe primary dysmenorrhea. This eliminates the dysmenorrhea symptom entirely and is the appropriate first-line for OCP-tolerant patients with severe symptoms.
The Iranian and Turkish Gynecology Research Tradition
The most active research community studying valerian in dysmenorrhea is in Iran, with additional contributions from Turkey, Iraq, and the broader Middle Eastern academic medicine ecosystem. Iranian universities (Babol University of Medical Sciences, Tehran University of Medical Sciences, Tarbiat Modares University, and others) have published several dozen randomized controlled trials of herbal interventions for primary dysmenorrhea over the past 15 years, frequently using mefenamic acid as the active comparator.
The herbs studied include valerian, chamomile, fennel (Foeniculum vulgare), ginger (Zingiber officinale), dill (Anethum graveolens), saffron (Crocus sativus), peppermint (Mentha piperita), and many others. The research tradition reflects both the strong local pharmacy curriculum and the cultural prominence of herbal medicine in Iranian, Persian, and broader Middle Eastern medical practice.
The pooled findings across this research literature support several conclusions:
- Multiple herbs produce measurable benefit — valerian, ginger, chamomile, and fennel all have positive RCT data in primary dysmenorrhea with comparable effect sizes
- None of the herbs reaches NSAID-level efficacy — head-to-head comparisons with mefenamic acid consistently show NSAIDs producing larger pain reduction, with herbs typically achieving 60-80% of the NSAID effect
- Tolerability is consistently better with herbs than with NSAIDs — the GI symptom rate is lower across all of the studied herbs versus NSAID comparators
- Combination herbal protocols appear to be additive — ginger plus valerian, or chamomile plus fennel, produce larger effects than either alone in the small comparative studies that have looked at this
This regional research tradition has not been heavily incorporated into Western dysmenorrhea guidelines (which still focus almost exclusively on NSAIDs and OCPs), but it provides a substantial empirical base for the herbal adjunctive options that integrative practitioners and patients in the West increasingly seek out.
The Mirabi 2011 trial is a representative example of this research tradition, both in study design (active herb vs placebo, primary dysmenorrhea population, two-cycle duration, VAS pain primary outcome with systemic symptom secondary outcome) and in the institutional setting (Babol University of Medical Sciences) and authorship (Iranian gynecology and pharmacology faculty).
Systemic Symptoms (Nausea, Fatigue, Headache, Mood)
One of the strongest findings of the Mirabi 2011 trial and consistent with the broader clinical experience is that valerian's benefit in dysmenorrhea is not confined to the uterine cramping pain but extends to the systemic symptoms that frequently accompany it. The composite "systemic manifestations" score in the Mirabi trial covered nausea, vomiting, syncope (lightheadedness), fatigue, diarrhea, and mood disturbance; the valerian group had statistically significant improvement in this composite versus placebo.
This is mechanistically consistent with valerian's broader pharmacology:
- Anxiolytic effect reduces the mood-disturbance and anticipatory-anxiety component of dysmenorrhea
- Sympathetic-tone reduction reduces the syncope/lightheadedness and palpitations
- Sleep effect reduces the fatigue, particularly when menstrual pain is disrupting sleep
- GI smooth-muscle effect reduces the diarrhea and abdominal cramping outside the uterine component
- Central pain modulation reduces the headache component, which is itself driven in part by prostaglandin-mediated cerebral vasodilation
The systemic-symptom benefit is one of the clearer advantages of valerian over single-mechanism analgesics. NSAIDs primarily address the uterine pain through prostaglandin inhibition but do less for the mood and sleep components. Acetaminophen is even more narrowly targeted. The Mirabi trial's documentation of multi-symptom improvement supports the clinical observation that patients on valerian for dysmenorrhea often report "feeling better overall during my period" rather than just "less cramping."
For patients with prominent menstrual-cycle mood symptoms (PMS or PMDD), the broader pattern of valerian's benefit may be more useful than the cramp-specific application. The combination of valerian with calcium, magnesium, and vitamin B6 (the standard PMS supplement stack) is widely used and has modest supporting evidence.
Combination Protocols (Valerian + Chamomile, Valerian + Fennel, Valerian + Ginger)
The Iranian and Turkish gynecology research has examined several herbal combinations for dysmenorrhea, with valerian appearing as a component in many protocols.
Valerian + chamomile. Chamomile (Matricaria recutita) contains apigenin, a flavonoid with GABA-A modulating activity, and bisabolol with antispasmodic effects. The combination addresses uterine spasm and central anxiety through partially overlapping mechanisms. Chamomile tea (1-2 cups daily during menses) plus valerian capsules is a common Iranian and Turkish protocol. See our Chamomile page.
Valerian + fennel. Fennel (Foeniculum vulgare) is a documented antispasmodic with positive RCT data in primary dysmenorrhea. The Modaress Nejad 2006 trial showed fennel extract approaching mefenamic acid's efficacy in some pain measures. The combination with valerian addresses uterine and gastrointestinal smooth-muscle spasm simultaneously. Particularly useful in patients with prominent GI symptoms during menses.
Valerian + ginger. Ginger (Zingiber officinale) has multiple positive RCTs in primary dysmenorrhea (Ozgoli 2009, Rahnama 2012, and others), with effect sizes comparable to NSAIDs. The mechanism involves cyclooxygenase inhibition (giving ginger pharmacology that overlaps with NSAIDs in target) plus anti-inflammatory and antiemetic effects. Combination with valerian addresses pain (overlapping pharmacology) plus anxiety and sleep (valerian-specific effects). The ginger plus valerian combination is one of the more empirically supported herbal regimens for dysmenorrhea.
Valerian + cramp bark (Viburnum opulus). Cramp bark, as the name suggests, has a strong reputation in Western herbalism for menstrual cramps, with documented uterine antispasmodic effects in animal models. The combination is widely used in Western herbal practice though less studied in formal RCTs.
Valerian + magnesium glycinate. Magnesium has independent RCT data in dysmenorrhea (Quaranta 2007 and others), with effect sizes around 30-50% reduction in pain scores. The mechanism involves calcium-channel modulation (parallel to valerian's mechanism) and central NMDA receptor effects. The combination is logical and well-tolerated. See our Magnesium Glycinate page.
Valerian + omega-3 fatty acids. Omega-3 fatty acids (EPA + DHA) compete with arachidonic acid as cyclooxygenase substrate, shifting prostaglandin production toward less inflammatory PGE3 series and away from the inflammatory PGE2 and PGF2a series that drive dysmenorrhea. Daily EPA + DHA supplementation reduces dysmenorrhea severity in trials, with effect that develops over months rather than within a single cycle.
The integrative protocol that has emerged for chronic primary dysmenorrhea: daily omega-3 fish oil (1-2 g EPA + DHA), daily magnesium glycinate (200-400 mg), valerian during menses (600-900 mg/day starting at menses onset for 2-3 days), NSAID as needed for breakthrough pain. The components are individually modest but cumulatively provide meaningful symptom control with excellent tolerability.
Dosing and Timing for Dysmenorrhea
The standard valerian regimen for dysmenorrhea, based on the Mirabi trial and follow-up Iranian and Turkish studies:
- Dose — 250-300 mg of standardized valerian extract three times daily, totaling 750-900 mg/day during menses
- Duration — start at the onset of menstrual flow, continue for 3 days, then discontinue until next menses
- Form — capsules of standardized 0.8% valerenic acid extract; tincture forms can be used but are less convenient
- Timing of doses — morning, mid-afternoon, and evening; the bedtime dose provides sleep benefit during the typically sleep-disrupting menses period
An alternative regimen is anticipatory dosing — start valerian 1-2 days before predicted menses to allow some accumulation, then continue through the first 2-3 days of flow. This may produce better effect for patients with very acute and severe onset on the first day.
Practical considerations:
- The daytime doses can produce mild sedation in some patients, particularly the first cycle. Many patients find that they tolerate this fine after the first cycle. Some adjust to twice-daily dosing (morning and bedtime) to avoid midday sedation.
- Combine with heat application (heating pad on lower abdomen or back) which has independent analgesic effect through gate-control mechanisms.
- Allow 2-3 cycles before judging effect. Individual variability in response is substantial, and the first cycle's response may not be representative.
- Continue background NSAIDs as needed for breakthrough pain. Valerian is generally an adjunct rather than a substitute for NSAIDs in most patients with moderate or severe dysmenorrhea.
Endometriosis and Secondary Dysmenorrhea
Endometriosis is a chronic condition in which endometrial-like tissue grows outside the uterus, producing chronic pelvic pain, dysmenorrhea, dyspareunia (painful intercourse), and frequently infertility. It affects approximately 10% of reproductive-age women and is a major cause of secondary dysmenorrhea (painful menses due to identifiable pathology rather than normal physiology).
The first-line treatments for endometriosis are hormonal suppression (combined OCPs, progestins, GnRH agonists or antagonists, danazol), NSAIDs for pain, and surgical excision of lesions for definitive diagnosis and tissue reduction. The condition is chronic and often requires combination therapy over many years.
The role of valerian in endometriosis is much more limited than in primary dysmenorrhea. The pain in endometriosis is driven by ectopic endometrial tissue with associated inflammation, fibrosis, and pelvic anatomic distortion — not primarily by uterine smooth-muscle contraction in normal endometrium. Valerian's uterine smooth-muscle calcium-channel mechanism is less relevant when the pain generator is extra-uterine.
That said, valerian remains useful in endometriosis as an adjunct for:
- Sleep disturbance from chronic pelvic pain
- Anxiety and depression related to chronic disease management
- Modest reduction of associated functional GI symptoms (bowel endometriosis or coincident IBS)
- Reduction of central pain sensitization through GABA mechanisms
Patients with endometriosis should be under the care of a gynecologist with expertise in the condition. Valerian is an appropriate gentle adjunct but should not be substituted for definitive endometriosis-specific care.
Cautions and Drug Interactions
- Pregnancy. Valerian should not be used in pregnancy. Uterine smooth-muscle relaxant activity, while desirable in the non-pregnant patient with dysmenorrhea, is theoretically concerning in pregnancy. The WHO and EMA both recommend avoidance. Stop valerian if pregnancy is possible.
- Lactation. Limited data; the WHO and EMA recommend avoidance. Resume after weaning if desired.
- Secondary dysmenorrhea. The diagnosis of "primary dysmenorrhea" should be confirmed before assuming valerian is appropriate. New-onset severe dysmenorrhea in adulthood, dysmenorrhea that has changed character, or dysmenorrhea associated with other symptoms (heavy bleeding, dyspareunia, infertility) warrants gynecologic evaluation to rule out endometriosis, adenomyosis, fibroids, or other pathology.
- Concurrent NSAIDs. Valerian and NSAIDs can be combined safely. The combination is in fact the most common clinical use pattern. There is no significant pharmacokinetic interaction.
- Concurrent hormonal contraception. Valerian and oral contraceptives can be combined safely. No significant pharmacokinetic interaction has been documented.
- CNS depressant interactions. Additive sedative effect with alcohol, benzodiazepines, opioids. Caution with combinations.
- Driving and operating machinery. The 3x daily dosing for dysmenorrhea includes daytime doses that may produce mild sedation. Adjust dose if driving is affected.
- Anesthesia. Discontinue at least 1 week before elective surgery.
- Inadequate response. If valerian after 2-3 cycles produces no perceptible benefit, escalation is unlikely to help. Reassess the regimen; consider hormonal options if not previously tried; consider gynecologic evaluation for secondary dysmenorrhea if symptoms warrant.
Key Research Papers
- Mirabi P, Dolatian M, Mojab F, Majd HA (2011). Effects of valerian on the severity and systemic manifestations of dysmenorrhea. International Journal of Gynaecology and Obstetrics. — PubMed
- Mirabi P, Mojab F (2013). The effects of valerian root on hot flashes in menopausal women. Iranian Journal of Pharmaceutical Research. — PubMed
- Modaress Nejad V, Asadipour M (2006). Comparison of the effectiveness of fennel and mefenamic acid on pain intensity in dysmenorrhoea. Eastern Mediterranean Health Journal. — PubMed
- Ozgoli G, Goli M, Moattar F (2009). Comparison of effects of ginger, mefenamic acid, and ibuprofen on pain in women with primary dysmenorrhea. Journal of Alternative and Complementary Medicine. — PubMed
- Rahnama P, Montazeri A, Huseini HF, Kianbakht S, Naseri M (2012). Effect of Zingiber officinale R. rhizomes (ginger) on pain relief in primary dysmenorrhea: a placebo randomized trial. BMC Complementary and Alternative Medicine. — PubMed
- Quaranta S, Buscaglia MA, Meroni MG, Colombo E, Cella S (2007). Pilot study of the efficacy and safety of a modified-release magnesium 250 mg tablet (Sincromag) for the treatment of premenstrual syndrome. Clinical Drug Investigation. — PubMed
- Marjoribanks J, Ayeleke RO, Farquhar C, Proctor M (2015). Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database of Systematic Reviews. — PubMed
- Pattanittum P, Kunyanone N, Brown J, et al. (2016). Dietary supplements for dysmenorrhoea. Cochrane Database of Systematic Reviews. — PubMed
- Iorno V, Burani R, Bianchini B, Minelli E, Martinelli F, Ciatto S (2008). Acupuncture treatment of dysmenorrhea resistant to conventional medical treatment. Evidence-Based Complementary and Alternative Medicine. — PubMed
- Jenabi E, Fereidoony B (2015). Effect of Achillea millefolium on relief of primary dysmenorrhea: a double-blind randomized clinical trial. Journal of Pediatric and Adolescent Gynecology. — PubMed
- Dawood MY (2006). Primary dysmenorrhea: advances in pathogenesis and management. Obstetrics and Gynecology. — PubMed
- Proctor M, Farquhar C (2006). Diagnosis and management of dysmenorrhoea. BMJ. — PubMed
PubMed Topic Searches
- PubMed: Valerian and dysmenorrhea
- PubMed: Iranian herbal dysmenorrhea research
- PubMed: Mefenamic acid for dysmenorrhea
- PubMed: Uterine calcium channels in dysmenorrhea
- PubMed: Herbal combinations for dysmenorrhea
Connections
- Valerian Overview
- Valerian Benefits Hub
- Valerian for Sleep
- Valerian for Anxiety
- Valerian for Muscle Relaxation
- Chamomile
- Passionflower
- Lemon Balm
- Lavender
- Magnesium
- Magnesium Glycinate
- Anxiety
- Insomnia
- Heart Palpitations
- Migraine
- Cramp Prevention
- Sleep Hygiene
- Stress Management
- Natural Anxiety Relief
- Endometriosis — a leading cause of secondary dysmenorrhea, where valerian is only an adjunct.