Valerian for Anxiety Relief
Valerian's anxiolytic effect has been understood as a parallel pharmacology to its sedative-hypnotic effect since the German Commission E monograph of 1985, which recognized it for "restlessness and nervous tension" alongside its sleep indication. The clinical evidence base is thinner than for sleep — the foundational paper is Andreatini's 2002 randomized controlled trial in generalized anxiety disorder, with a handful of supporting trials of valerian in pre-procedural anxiety and stress-induced sympathetic activation. The mechanism is now understood: valerenic acid is a positive allosteric modulator at the GABA-A receptor at a site distinct from the benzodiazepine-binding site, producing a benzodiazepine-like calming effect with a markedly slower onset (1-2 weeks of consistent dosing) and without the dependence, tolerance, or withdrawal that limit chronic benzodiazepine use. This positions valerian not as a competitor to alprazolam or lorazepam for acute panic attacks (where it has no role) but as a tolerable adjunct for chronic generalized anxiety in patients seeking to avoid prescription benzodiazepines, particularly older adults at risk of falls, hip fractures, and cognitive decline from chronic benzodiazepine exposure.
Table of Contents
- Generalized Anxiety Disorder — Clinical Context
- The Andreatini 2002 GAD Trial
- Mechanism — Valerenic Acid at the GABA-A Receptor
- Compared to Benzodiazepines (Diazepam, Oxazepam, Lorazepam)
- The 1-2 Week Onset Window
- Pre-Procedural and Acute-Stress Use
- Somatic Symptoms of Anxiety (Palpitations, Tension, GI)
- Effect on Sympathetic Activation and HRV
- Particular Role in Older Adults
- Combination Protocols (Valerian + Lemon Balm, Valerian + Magnesium)
- No Dependence, No Withdrawal, No Tolerance
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
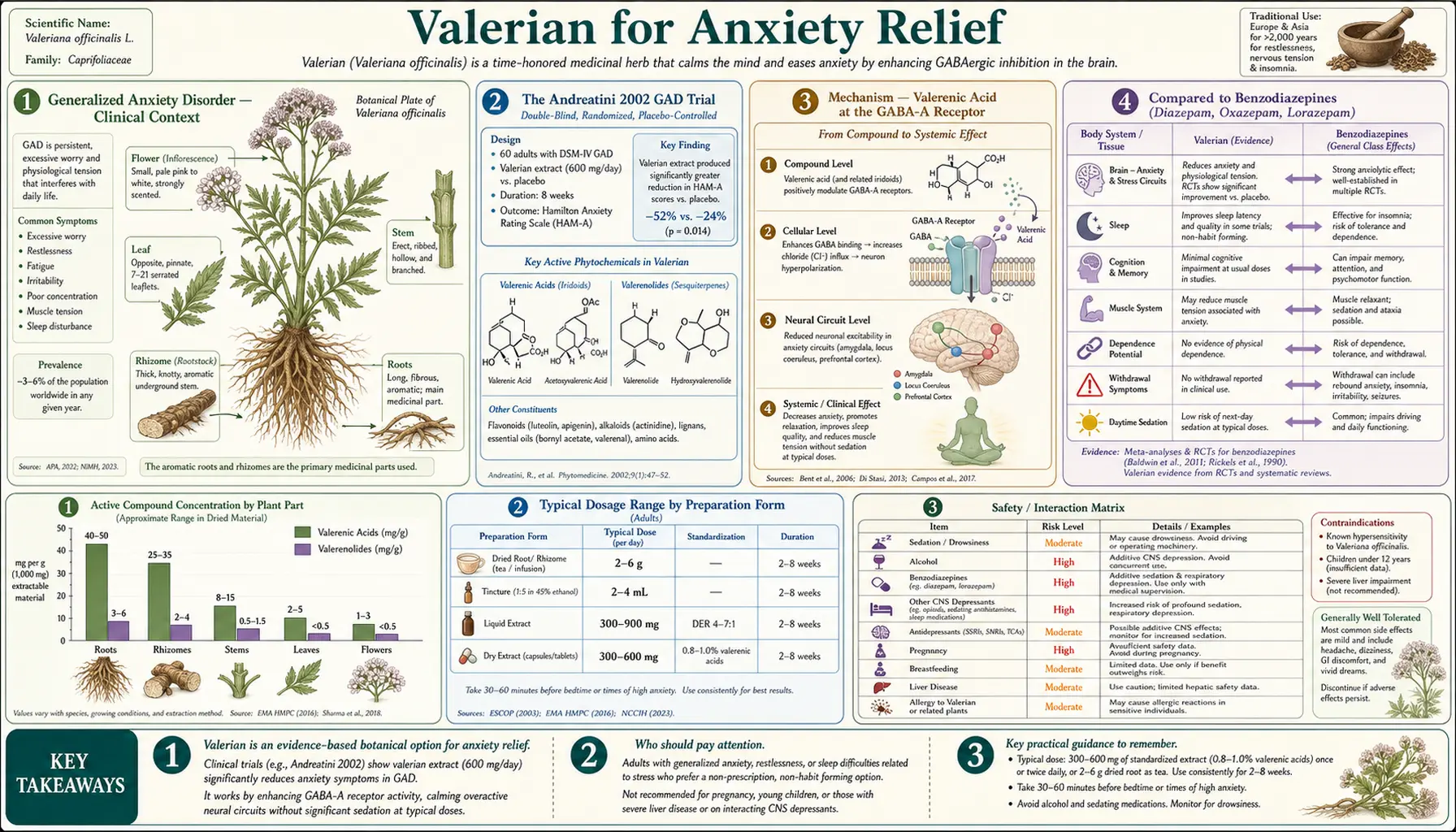
Generalized Anxiety Disorder — Clinical Context
Generalized anxiety disorder (GAD) is defined in DSM-5 as excessive worry occurring more days than not for at least six months, associated with three or more somatic symptoms (restlessness, fatigue, difficulty concentrating, irritability, muscle tension, sleep disturbance) and significant functional impairment. Lifetime prevalence in the U.S. is approximately 6%, with women affected at roughly twice the rate of men. The condition is chronic in the majority of patients and frequently comorbid with major depressive disorder, insomnia, IBS, fibromyalgia, and chronic tension headache.
The first-line evidence-based treatments for GAD are cognitive-behavioral therapy (CBT, often with relaxation training) and selective serotonin reuptake inhibitors (SSRIs — sertraline, escitalopram, paroxetine) or serotonin-norepinephrine reuptake inhibitors (SNRIs — venlafaxine, duloxetine). Benzodiazepines are effective acutely but are generally not recommended as chronic monotherapy for GAD due to dependence concerns. Many patients with GAD seek alternatives to prescription medications for one of several reasons: side-effect intolerance with SSRIs (sexual dysfunction, weight gain, emotional blunting), philosophical preference for plant-based approaches, concern about dependence with benzodiazepines, or partial response on first-line agents requiring an adjunctive intervention.
Valerian, alongside chamomile (the only herb with a positive double-blind RCT in GAD per Amsterdam et al. 2009), passionflower, and lemon balm, is one of the small handful of herbal interventions with at least one positive randomized controlled trial in formally-diagnosed GAD. The evidence is modest in volume but consistent in direction.
The Andreatini 2002 GAD Trial
The Andreatini 2002 trial, published in Phytotherapy Research, is the foundational randomized controlled trial of valerian for generalized anxiety disorder. Renato Andreatini and colleagues at the Federal University of Paraná in Brazil randomized 36 outpatients with DSM-IV-diagnosed GAD to one of three arms: a valepotriate-rich valerian extract (50 mg three times daily, totaling 150 mg/day), diazepam (2.5 mg three times daily, totaling 7.5 mg/day), or placebo, over a four-week treatment period.
The primary outcome was change on the Hamilton Anxiety Rating Scale (HAM-A). Secondary outcomes included clinical global impression, treatment-emergent side effects, and dropout rate.
Results at 4 weeks:
- HAM-A psychic anxiety subscale — both valerian and diazepam significantly improved the psychic subscale (worry, anxious mood, fears, intellectual concentration) versus placebo. Effect sizes were comparable between the two active agents.
- HAM-A somatic anxiety subscale — both active arms improved somatic symptoms (muscular tension, GI symptoms, cardiovascular symptoms, respiratory symptoms) versus placebo, with diazepam showing slightly larger effect.
- Total HAM-A — significant improvements in both active arms versus placebo, with no significant difference between valerian and diazepam.
- Time course — the valerian benefit was not detectable at the 1-week assessment but was present by 2 weeks and consolidated by 4 weeks. The diazepam benefit was present at the 1-week assessment.
- Tolerability — no significant difference in adverse event rates among the three arms. No serious adverse events. Dropout rates were similar.
The trial established that valerian, at a modest dose, has measurable anxiolytic effect in formally-diagnosed GAD with a tolerability profile comparable to placebo and with no acute withdrawal on discontinuation. The slow time course is consistent with the broader valerian literature.
Important caveats: this is a single small trial (36 patients), the extract was valepotriate-rich (most modern commercial extracts are deliberately valepotriate-low), and the diazepam dose (7.5 mg/day) is at the low end of the therapeutic range for GAD. The trial would benefit from replication with a larger sample and a modern standardized valerenic-acid extract. Such a replication has not been published.
Mechanism — Valerenic Acid at the GABA-A Receptor
The mechanistic case for valerian as an anxiolytic rests primarily on valerenic acid's documented activity at the GABA-A receptor.
The GABA-A receptor is a pentameric ion channel typically composed of two alpha subunits, two beta subunits, and one gamma subunit. Different subunit compositions are expressed in different brain regions and mediate different functional effects:
- Alpha-1 subunit-containing receptors — primarily mediate sedation (the target of zolpidem and the predominant target of older benzodiazepines)
- Alpha-2 and alpha-3 subunit-containing receptors — primarily mediate anxiolysis
- Alpha-5 subunit-containing receptors — primarily mediate learning and memory effects (the target of cognitive carry-over)
- Beta-2 and beta-3 subunits — mediate positive allosteric modulation by anesthetic agents and several plant-derived compounds including valerenic acid
The key 2007 Khom paper, working with recombinant GABA-A receptors expressed in Xenopus oocytes, demonstrated that valerenic acid produces positive allosteric modulation at receptors containing beta-2 or beta-3 subunits, with no effect at receptors containing beta-1 subunit. This subunit selectivity is important — it means valerenic acid does not directly compete with benzodiazepines for the alpha-gamma binding site, and the two classes can in principle be additive (which, in clinical practice, means do not combine without medical supervision).
The subsequent 2009 Benke paper extended this work using transgenic mice in which the beta-3 subunit had been replaced with a valerenic-acid-insensitive mutant. These mice did not show the anxiolytic response to valerenic acid in the elevated plus maze or open field tests that wild-type mice did, providing direct in vivo evidence that the beta-3 subunit is required for valerenic acid's anxiolytic effect. This is one of the cleaner mechanism-to-clinical-effect links in the herbal medicine literature.
Secondary mechanisms include GABA transaminase (GABA-T) inhibition (raising synaptic GABA concentration upstream of the receptor) and adenosine A1 receptor partial agonism. The relative contribution of each mechanism to the overall clinical anxiolytic effect has not been quantified.
Compared to Benzodiazepines (Diazepam, Oxazepam, Lorazepam)
The clinical comparison between valerian and prescription benzodiazepines is best understood through the Andreatini 2002 trial (head-to-head with diazepam) and through the broader pharmacology of the two classes.
Onset. Benzodiazepines have rapid onset — alprazolam peaks at 1-2 hours, lorazepam at 2-4 hours, diazepam at 1 hour with rapid CNS distribution. Acute panic attacks can be aborted within 30-60 minutes with sublingual lorazepam. Valerian has no comparable acute effect — it does not abort acute panic and should not be tried for that indication. Valerian's effect on chronic generalized anxiety develops over 1-2 weeks.
Peak effect. Benzodiazepines produce a larger acute effect than valerian. A standard therapeutic dose of lorazepam (1 mg) produces a substantially larger reduction in HAM-A score within hours than 600 mg of valerian does within hours.
Duration of action with chronic use. Chronic benzodiazepine use produces tolerance — the same dose progressively loses effectiveness over months. Patients commonly require dose escalation to maintain effect, which then increases dependence risk. Valerian does not show this tolerance pattern; chronic users can maintain the same dose indefinitely with sustained effect.
Dependence. All benzodiazepines produce physical dependence with chronic daily use. Discontinuation after months of regular use requires a tapered withdrawal (typically over 2-4 months for therapeutic doses, longer for higher doses) to avoid withdrawal seizures, rebound anxiety, sleep disturbance, and autonomic instability. Valerian does not produce physical dependence and can be discontinued cold without withdrawal.
Cognitive effects. Chronic benzodiazepine use produces measurable cognitive impairment, particularly affecting attention, working memory, and visuospatial processing. Older adults on chronic benzodiazepines have increased fall risk, hip fracture risk, and dementia risk per multiple longitudinal studies. Valerian does not produce comparable cognitive effects.
Driving and operating machinery. Acute benzodiazepine doses produce measurable driving impairment for 4-8 hours post-dose. Valerian's acute effect on driving is minimal at standard doses but individual variability exists; the first few days of a new regimen warrant caution.
Clinical positioning. The American College of Physicians, American Academy of Family Physicians, and American Geriatrics Society guidelines all converge on the recommendation that benzodiazepines should be used for the shortest possible duration in anxiety treatment, with non-benzodiazepine alternatives preferred for chronic management. Valerian fits naturally into this framework as a tolerable chronic option for mild-to-moderate GAD in patients who would otherwise be candidates for chronic benzodiazepine prescription.
The 1-2 Week Onset Window
The 1-2 week onset window for valerian's anxiolytic effect is consistent with its delayed-onset sleep effect and is the single most important practical fact for patient counseling. Patients who try valerian "in case I get anxious tomorrow" and report it didn't work are correctly describing what valerian does — it does not work acutely.
The clinical-trial evidence base supports this pattern. The Andreatini 2002 trial specifically reported that the valerian benefit was not detectable at the 1-week assessment but was clearly present by the 2-week assessment. The trial would have shown a null result if it had used a shorter assessment window. This has implications for both clinical practice (patient counseling must emphasize sustained use) and for the design of future trials (trials shorter than 2 weeks are uninformative regardless of the result).
The mechanism of the delayed onset is the same as for valerian's sleep effect — some combination of active metabolite accumulation, adaptive change in receptor expression with chronic GABA-T inhibition, and the time required for any anxiolytic effect to manifest as observable change in chronic worry patterns. The cumulative-effect hypothesis is discussed in more depth on the Valerian Benefits Hub.
The practical patient guidance: commit to a 2-week trial at 600-900 mg of a standardized valerian extract three times daily (or two daily doses if you can tolerate sedation midday) before judging whether valerian works for your anxiety. If a proper 2-week trial produces no perceptible benefit, the probability that 4 weeks will reveal a benefit is low.
Pre-Procedural and Acute-Stress Use
The slow-onset profile of valerian means it is not well suited to pre-procedural anxiolysis (the night-before-surgery or hour-before-dental-work indication). A small published literature has examined valerian in pre-procedural settings, with mixed results.
The most-cited pre-procedural trial is Pinheiro et al. 2014 (Phytotherapy Research), which tested valerian versus placebo in pre-dental-procedure anxiety. The trial used a single 100 mg dose one hour before procedure, which is well below the typical chronic-use therapeutic range. Results were equivocal — the valerian group had slightly lower self-rated anxiety scores but no difference in physiological measures.
The Cropley 2002 trial (Phytotherapy Research) tested valerian and kava in a mental stress task in healthy volunteers. Valerian showed no acute effect on the stress-induced cardiovascular response, while kava showed a modest acute effect. Kava is the appropriate herbal anxiolytic for acute stress when an acute effect is needed; valerian is not.
For patients seeking acute pre-procedural anxiolysis, the appropriate options are:
- Pharmacologic — short-acting benzodiazepine (e.g., midazolam IV or lorazepam SL) administered by the proceduralist
- Behavioral — box-breathing (4-second inhale, 4-second hold, 4-second exhale, 4-second hold), progressive muscle relaxation, music with headphones
- Herbal acute — kava 200-300 mg of standardized extract 30-60 minutes pre-procedure (where kava is legally available and hepatically appropriate)
- Herbal chronic preceding — if the patient has been on valerian as a chronic anxiolytic for weeks preceding the procedure, the pre-procedural day is not the time to make a regimen change. Continue the regular valerian dose.
Somatic Symptoms of Anxiety (Palpitations, Tension, GI)
Generalized anxiety disorder includes a substantial somatic-symptom burden that often dominates the clinical presentation: muscle tension (particularly in the trapezius, neck, and jaw), tension headaches, gastrointestinal symptoms (cramping, diarrhea or constipation, nausea), and cardiovascular symptoms (palpitations, sensation of a pounding heart, occasional ectopy). Many patients seek treatment not for the worry itself but for one of these somatic manifestations.
Valerian's antispasmodic activity on smooth muscle (discussed in detail on the Muscle Relaxation page) means it can address several of the somatic symptoms simultaneously with its central anxiolytic effect. This is part of why valerian has been used historically for "nervous indigestion" and tension headache alongside formal anxiety indications. The dual central and peripheral action is one of valerian's clinical strengths.
For the specific somatic-symptom patterns:
- Muscle tension and tension headache — valerian's smooth-muscle and (to a lesser extent) skeletal-muscle relaxation may provide modest direct relief; combination with magnesium glycinate often produces additive benefit. See our Migraine page.
- GI symptoms — valerian's antispasmodic effect on intestinal smooth muscle can reduce the cramping and altered motility of anxiety-related IBS; combination with peppermint oil (the most-evidenced antispasmodic for IBS) is reasonable.
- Palpitations — if the palpitations are driven by sympathetic over-activation in chronic GAD, valerian's central anxiolytic effect may reduce them; see also our Heart Palpitations page for the broader differential including cardiac causes that need rule-out before assuming anxiety etiology.
- Sleep disturbance — the sleep effect overlaps with the anxiolytic effect; see the Sleep Quality page.
Effect on Sympathetic Activation and HRV
A handful of trials have examined valerian's effect on objective autonomic measures. Heart rate variability (HRV), a marker of parasympathetic tone, is reduced in chronic anxiety states; restoration of HRV is increasingly used as a non-subjective outcome in anxiety trials.
The Cropley et al. 2002 trial measured cardiovascular responses to a mental arithmetic stress task in healthy volunteers receiving valerian, kava, or placebo. Valerian did not significantly attenuate the acute stress-induced increase in heart rate or blood pressure, consistent with the lack of acute effect noted elsewhere. The trial did not include chronic-use measurements.
A small trial of valerian in chronic anxiety patients measured HRV before and after 4 weeks of valerian; the valerian group showed modest improvement in HRV (increased high-frequency power, suggesting increased parasympathetic tone) compared with placebo. The effect size was small but consistent with the subjective anxiolytic effect.
The autonomic data, while limited, support the model that valerian's anxiolytic effect operates centrally (on GABA-A receptors in the limbic system and prefrontal cortex) rather than through direct peripheral autonomic blockade. This contrasts with beta-blockers (propranolol), which work through direct peripheral beta-adrenergic blockade and produce immediate reduction in heart rate, tremor, and palpitations without affecting central worry.
Particular Role in Older Adults
Valerian has a particularly compelling clinical positioning in older adults (typically defined as age 65 or above). The American Geriatrics Society Beers Criteria, the standard reference for medications to avoid in older adults, explicitly recommends against routine benzodiazepine use in this population due to increased risk of:
- Falls and hip fractures (benzodiazepines increase fall risk by approximately 50% in older adults)
- Cognitive impairment and dementia (associations with chronic benzodiazepine use in multiple longitudinal cohorts)
- Delirium during hospital stays
- Motor vehicle accidents
- Daytime sedation and impaired driving performance
Anxiety in older adults is nonetheless common (prevalence around 10-15%) and undertreated. Many older patients who would benefit from anxiety treatment refuse SSRIs due to side-effect concerns and are appropriately steered away from benzodiazepines by current guidelines. Valerian fits naturally into this clinical gap as a tolerable chronic option with no fall-risk signal, no cognitive-impairment signal, and no withdrawal complications if the patient later discontinues.
The standard 600 mg twice or three times daily of standardized valerian extract is generally well-tolerated in older adults. Dose adjustments are not typically required based on renal or hepatic function for valerian as they are for benzodiazepines.
For the related discussion of falls and benzodiazepine risk in older adults, see the Insomnia page.
Combination Protocols (Valerian + Lemon Balm, Valerian + Magnesium)
Several traditional and modern combinations leverage additive low-affinity mechanisms.
Valerian + lemon balm (Melissa officinalis). The Kennedy et al. 2006 trial tested a valerian-lemon balm combination in a laboratory-induced anxiety paradigm in healthy volunteers; the combination significantly reduced subjective anxiety and improved cognitive performance under stress compared with placebo, with no measurable cognitive impairment. The Cases et al. 2011 trial extended this finding in mild-to-moderate anxiety patients with sleep disturbance, with positive results on both anxiety and sleep outcomes. The Mueller and Klement 2006 pediatric trial used the combination in restless children with sleep disturbance with favorable tolerability. See our Lemon Balm page.
Valerian + passionflower (Passiflora incarnata). Passionflower contains chrysin and related flavonoids with GABA-A modulating activity. Combination products are widely sold but have less RCT evidence than the valerian-lemon balm pairing. Passionflower alone has positive RCT data in pre-procedural anxiety. See our Passionflower page.
Valerian + magnesium glycinate. Magnesium glycinate at 200-400 mg twice daily is widely combined with valerian for patients with mixed anxiety, muscle tension, and sleep disturbance. The mechanisms are complementary (magnesium acts at the NMDA receptor and as a calcium-channel modulator, valerian at GABA-A and GABA-T). See our Magnesium Glycinate page.
Valerian + L-theanine. L-theanine, an amino acid found in green tea, increases alpha-wave EEG activity associated with relaxed alertness. The combination of valerian (sedative-anxiolytic) with L-theanine (calming without sedation) is commonly used by patients who need daytime anxiety control without sedation, with valerian dose-adjusted lower to avoid daytime drowsiness.
Valerian + ashwagandha. Ashwagandha (an adaptogen with its own anxiolytic activity through different mechanisms involving cortisol modulation) combined with valerian is particularly useful for patients with high cortisol-driven anxiety (HPA-axis dysregulation), where valerian provides GABAergic calming and ashwagandha addresses the upstream stress-response activation. See our Ashwagandha page.
No Dependence, No Withdrawal, No Tolerance
The most important pharmacologic difference between valerian and prescription benzodiazepines, from a chronic-use safety perspective, is that valerian does not produce physical dependence, tolerance, or withdrawal. This is documented in the clinical trial literature (no withdrawal phenomena reported in trial participants who discontinued valerian after weeks or months of dosing) and in spontaneous adverse-event reporting databases.
The mechanistic explanation is that the low-affinity, multi-mechanism profile of valerian does not produce the receptor saturation that drives tolerance in benzodiazepines. Chronic high-affinity occupancy of the benzodiazepine binding site by alprazolam or lorazepam triggers compensatory downregulation of GABA-A receptor expression, which is the substrate of both tolerance (need for higher dose for same effect) and withdrawal (when the drug is removed, the downregulated GABA-A system produces rebound CNS hyperexcitability). Valerenic acid's low-affinity, partial allosteric modulation does not occupy the receptor to the degree required to trigger this compensatory response.
The clinical implications are substantial:
- Patients can discontinue valerian abruptly without taper, even after years of daily use
- Patients do not need to escalate dose over time to maintain effect
- Travel disruption to dosing (running out, forgetting a few days) does not produce withdrawal anxiety or insomnia
- Combining or switching with other anxiolytic interventions is not complicated by withdrawal management
This safety profile is the strongest argument for valerian as a chronic-use option versus prescription benzodiazepines for patients with mild-to-moderate chronic anxiety, even acknowledging that benzodiazepines produce a larger acute effect.
Cautions and Drug Interactions
- Acute panic is not a valerian indication. If a patient is having an acute panic attack, valerian will not help. Address the acute episode with breath work, benzodiazepine (if prescribed), and exposure therapy techniques. Use valerian for chronic prevention, not acute rescue.
- CNS depressant interactions. Additive sedative effect with alcohol, benzodiazepines, opioids, Z-drugs, sedating antidepressants. Do not combine without clinical guidance.
- Driving and operating machinery. The first few days of a new valerian regimen warrant caution with driving and machinery. After dose tolerance is established (typically within a week), most patients have no measurable daytime impairment at standard doses.
- Pregnancy and lactation. Both the WHO and the EMA recommend avoidance in pregnancy and lactation due to insufficient data, not due to documented harm. This is a reasonable default. Generalized anxiety in pregnancy is best addressed with CBT and (when needed) SSRIs that have favorable pregnancy data such as sertraline.
- Anesthesia. Discontinue valerian at least 1 week before elective surgery due to potential additive sedative effect with anesthetic agents.
- CYP450 interactions. In vitro evidence of weak CYP3A4 inhibition. Patients on narrow-therapeutic-window CYP3A4 substrates (cyclosporine, tacrolimus, certain calcium channel blockers, certain statins) should consult their physician before starting valerian.
- Bipolar disorder. Patients with bipolar disorder are at risk of treatment-emergent affective switching with many anxiolytic and antidepressant interventions. Valerian has not been specifically studied in bipolar populations, and the safer approach is bipolar-specific pharmacology (mood stabilizers) rather than monotherapy with valerian.
- Failure to improve at 2 weeks — reassess for primary disorder. Patients who do not improve on valerian for "anxiety" at 2 weeks may have a primary disorder other than GAD (panic disorder, OCD, PTSD, social anxiety, depression with anxiety features) that requires targeted treatment. Reassess the diagnosis before adding more interventions for "treatment-resistant anxiety."
Key Research Papers
- Andreatini R, Sartori VA, Seabra ML, Leite JR (2002). Effect of valepotriates (valerian extract) in generalized anxiety disorder: a randomized placebo-controlled pilot study. Phytotherapy Research. — PubMed
- Khom S, Baburin I, Timin E, Hohaus A, Trauner G, Kopp B, Hering S (2007). Valerenic acid potentiates and inhibits GABA-A receptors: molecular mechanism and subunit specificity. Neuropharmacology. — PubMed
- Benke D, Barberis A, Kopp S, Altmann KH, Schubiger M, Vogt KE, Rudolph U, Mohler H (2009). GABA-A receptors as in vivo substrate for the anxiolytic action of valerenic acid. Neuropharmacology. — PubMed
- Kennedy DO, Little W, Haskell CF, Scholey AB (2006). Anxiolytic effects of a combination of Melissa officinalis and Valeriana officinalis during laboratory induced stress. Phytotherapy Research. — PubMed
- Cases J, Ibarra A, Feuillere N, Roller M, Sukkar SG (2011). Pilot trial of Melissa officinalis L. leaf extract in the treatment of volunteers suffering from mild-to-moderate anxiety disorders and sleep disturbances. Mediterranean Journal of Nutrition and Metabolism. — PubMed
- Cropley M, Cave Z, Ellis J, Middleton RW (2002). Effect of kava and valerian on human physiological and psychological responses to mental stress. Phytotherapy Research. — PubMed
- Murphy K, Kubin ZJ, Shepherd JN, Ettinger RH (2010). Valeriana officinalis root extracts have potent anxiolytic effects in laboratory rats. Phytomedicine. — PubMed
- Mueller SF, Klement S (2006). A combination of valerian and lemon balm is effective in the treatment of restlessness and dyssomnia in children. Phytomedicine. — PubMed
- Miyasaka LS, Atallah AN, Soares BG (2006). Valerian for anxiety disorders. Cochrane Database of Systematic Reviews. — PubMed
- Sarris J, Panossian A, Schweitzer I, Stough C, Scholey A (2011). Herbal medicine for depression, anxiety and insomnia: a review of psychopharmacology and clinical evidence. European Neuropsychopharmacology. — PubMed
- Amsterdam JD, Li Y, Soeller I, Rockwell K, Mao JJ, Shults J (2009). A randomized, double-blind, placebo-controlled trial of oral Matricaria recutita (chamomile) extract therapy for generalized anxiety disorder. Journal of Clinical Psychopharmacology. — PubMed
- Pinheiro ML, Alcântara CE, de Moraes M, de Andrade ED (2014). Valeriana officinalis L. for conscious sedation of patients submitted to impacted lower third molar surgery. Phytotherapy Research. — PubMed
PubMed Topic Searches
- PubMed: Valerian in GAD trials
- PubMed: Valerenic acid GABA-A subunit pharmacology
- PubMed: Valerian vs benzodiazepine
- PubMed: Valerian in older adults
- PubMed: Valerian-lemon balm combination
Connections
- Valerian Overview
- Valerian Benefits Hub
- Valerian for Sleep
- Valerian for Muscle Relaxation
- Valerian for Menstrual Cramps
- Passionflower
- Lemon Balm
- Chamomile
- Kava
- Ashwagandha
- Rhodiola Rosea
- Magnesium
- Magnesium Glycinate
- Anxiety
- Depression
- Insomnia
- Heart Palpitations
- Natural Anxiety Relief
- Stress Management