Valerian — Benefits Deep Dive
Valeriana officinalis is the most-popular herbal sleep aid in the Western world, with sales in the hundreds of millions of dollars annually across Europe, North America, and Japan. It is also one of the most polarizing herbal medicines — clinical trials that test it as a fast-acting hypnotic (compared head-to-head with a benzodiazepine on the first night of use) typically find little or no effect, while trials that test it for two to four weeks of continuous use typically find a meaningful improvement in sleep latency and sleep quality. The active chemistry is split between the controversial valepotriates (epoxide-containing compounds that degrade rapidly on storage and may be genotoxic in vitro) and the better-tolerated valerenic acid (a sesquiterpene with documented GABA-A receptor binding). The smell is unmistakable — old valerian root preparations are routinely described as "dirty socks" or "fermented gym shorts," which has limited consumer acceptance. The four benefit pages below explore the conditions where valerian produces measurable clinical effect — the chronic-insomnia application that founded its modern reputation, generalized anxiety, smooth-muscle relaxation including the traditional restless-legs application, and the surprisingly well-documented Iranian and Turkish gynecology literature on primary dysmenorrhea.
Deep-Dive Articles
Sleep Quality
The Bent 2006 meta-analysis (16 trials), the Donath 2000 sleep-latency crossover trial, the Leathwood 1985 paper that is the single most-cited valerian sleep study, the dual valerenic-acid + valepotriate active-compound model, GABA transaminase (GABA-T) inhibition combined with 5-HT5A receptor binding, and the standardized 600-900 mg extract dose range that has emerged as the consensus therapeutic window for chronic insomnia.
Anxiety Relief
The Andreatini 2002 generalized anxiety disorder trial, head-to-head comparisons with diazepam and oxazepam showing slower onset but no dependence, valerenic acid as a positive allosteric modulator at the GABA-A receptor (binding at a site distinct from benzodiazepines), and the 1-2 week onset window that pushes valerian toward chronic-anxiety-management use rather than acute panic.
Muscle Relaxation
Antispasmodic effect on intestinal and uterine smooth muscle, the traditional restless-legs-syndrome application that has been formalized in a small but encouraging clinical literature, comparison with prescription muscle relaxants (cyclobenzaprine, methocarbamol, baclofen), and the emerging fibromyalgia adjunctive role for patients seeking non-pharmacologic options.
Menstrual Cramps
The Mirabi 2011 dysmenorrhea randomized controlled trial, the proposed uterine smooth-muscle calcium-channel-blockade mechanism, head-to-head comparison with mefenamic acid (Ponstel), and the broader Iranian and Turkish gynecology literature in which valerian has been studied alongside chamomile, fennel, and ginger as a tolerable adjunct to NSAID therapy for primary dysmenorrhea.
Table of Contents
- Deep-Dive Articles
- Why Valerian Produces Effects (Multi-Mechanism, Each Mild)
- The 1-2 Week Onset Window — Night-of-Only vs Cumulative Use
- Key Research Papers
- External Authoritative Resources
- Connections
- Featured Videos
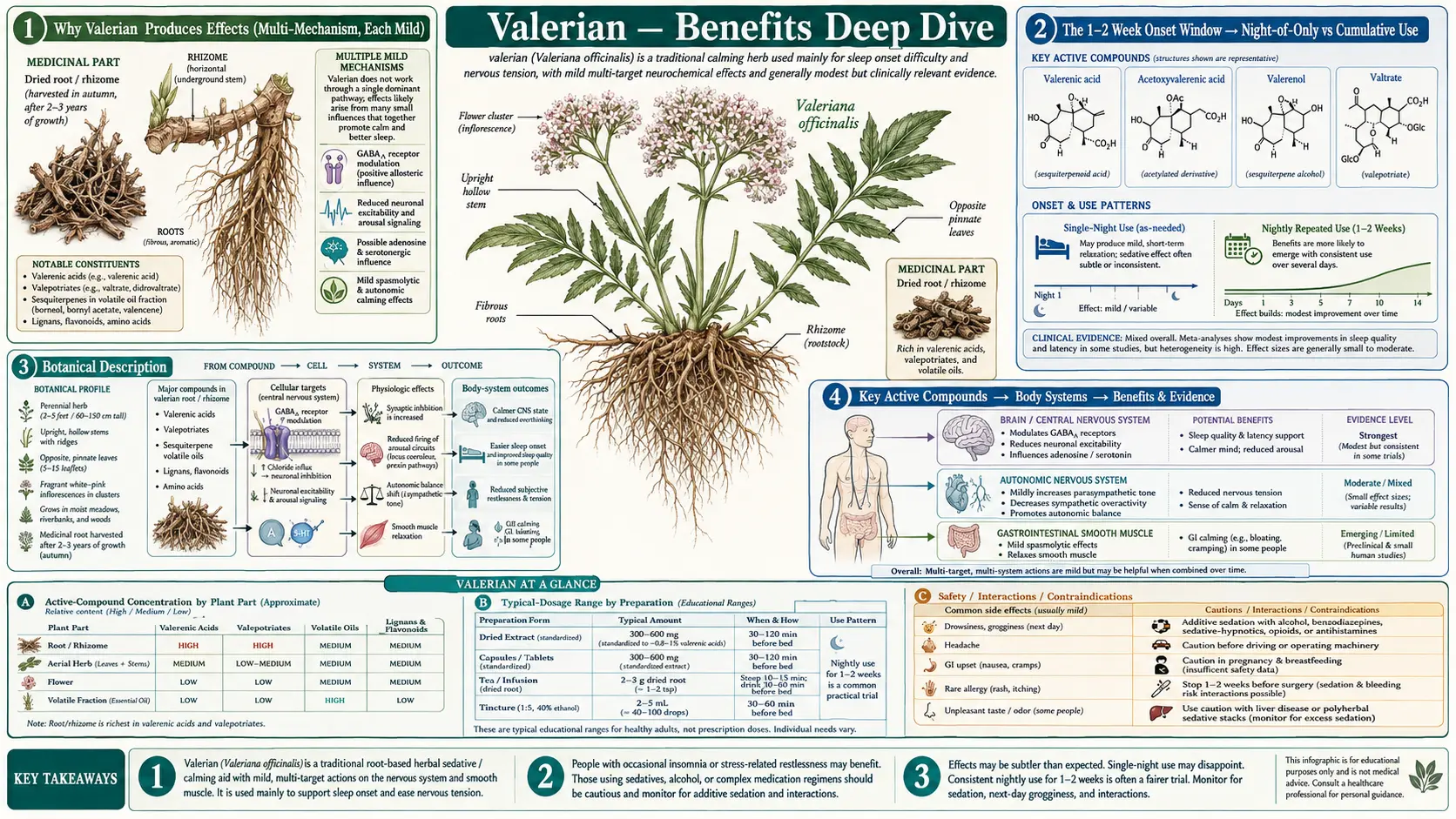
Why Valerian Produces Effects (Multi-Mechanism, Each Mild)
Valerian is unusual among sedative-hypnotic compounds in that it has no single dominant active compound and no single dominant mechanism. The traditional "active ingredient" question — the one that pharmacologists asked from the 1960s through the 1990s about valerian — never resolved cleanly because valerian root is a mixture of dozens of biologically active small molecules, none of which is potent enough alone to fully explain the clinical effect. The modern model is that valerian works through four parallel low-affinity mechanisms that act additively on the same final pathway (CNS depression and smooth-muscle relaxation), and the failure of any single fraction to reproduce whole-root effects in animal studies is itself evidence for the multi-mechanism model.
- GABA transaminase (GABA-T) inhibition — valerenic acid and its derivatives weakly inhibit the enzyme that catabolizes GABA in the synaptic cleft and presynaptic terminal. The net effect is to extend GABA's tonic inhibitory signal, which is the same final pathway as benzodiazepines (which positively modulate GABA-A receptors) and Z-drugs (zolpidem at the alpha-1 subunit), but achieved upstream by raising local GABA concentration rather than amplifying its receptor effect. See Sleep Quality for the clinical translation.
- GABA-A receptor positive allosteric modulation (separate site from benzodiazepines) — valerenic acid binds to the GABA-A receptor at the beta-2 and beta-3 subunits, at a site distinct from the benzodiazepine-binding site at the alpha-gamma interface. This produces a positive allosteric effect on the receptor's response to GABA, similar in mechanism (but much weaker in potency) to benzodiazepines and barbiturates. The clinical anxiolytic effect appears to be driven primarily by this mechanism — see Anxiety Relief.
- 5-HT5A serotonin receptor binding — in vitro radioligand binding studies have identified affinity for the 5-HT5A receptor, a poorly-characterized serotonin receptor subtype expressed in the suprachiasmatic nucleus and dorsal raphe. This may explain why valerian feels "different from a benzodiazepine" in subjective reports — some patients describe more dream-rich sleep and less morning cognitive impairment than with prescription hypnotics.
- Adenosine A1 receptor activity and calcium channel blockade — multiple valerian fractions have weak partial agonist activity at the adenosine A1 receptor (the same receptor caffeine blocks, which is why caffeine is wake-promoting and adenosine accumulation is sleep-promoting), and additional weak blockade of L-type voltage-gated calcium channels in smooth muscle. These together explain the antispasmodic and uterine-relaxant effects discussed in Muscle Relaxation and Menstrual Cramps.
The chemistry is split between two compound classes with very different reputations. Valerenic acid (a sesquiterpene unique to Valeriana officinalis and not found in related Valeriana species) is the most consistently studied and most likely the dominant clinical actor. It is stable on storage, has reasonably well-characterized receptor binding, and is the standardization target for most modern commercial extracts (the 0.8% valerenic acid standardized extract is the de facto industry standard). Valepotriates (epoxide-containing iridoid esters) are the older "controversial" active class — they degrade rapidly on storage (so old preparations contain very little), they have raised genotoxicity flags in some in vitro assays, and modern extracts often deliberately exclude them by using ethanol or aqueous extraction methods that leave the lipophilic valepotriates behind. The clinical effect of standardized modern extracts is largely a valerenic-acid effect with valepotriate exclusion.
The 1-2 Week Onset Window — Night-of-Only vs Cumulative Use
The single most important practical fact about valerian — the one that explains both the disappointing acute trials and the favorable chronic trials — is that it has an onset of action that is not "night of." Patients who take 600 mg of standardized valerian extract for the first time, an hour before bed, on the night of a stressful day, typically report no detectable effect. The same patient who takes 600 mg every night for two weeks typically reports that sleep latency has shortened, that morning awakenings have decreased, and that subjective sleep quality has improved. This pattern is the opposite of the benzodiazepines and Z-drugs, which work on the first night (often dramatically) but lose effect with chronic use due to tolerance.
The mechanism of the cumulative effect is not fully understood. Three hypotheses have been advanced:
- Active metabolite accumulation — valerenic acid has a long elimination half-life and may accumulate with repeated dosing to reach a steady-state plasma concentration that is sub-therapeutic on a single dose
- Adaptive change in GABA-A receptor density or sensitivity — some animal models suggest that chronic GABA-T inhibition leads to upregulation of post-synaptic GABA-A response, analogous (in opposite direction) to the well-documented downregulation seen with chronic benzodiazepine use
- Anxiolytic effect translating to sleep effect — valerian's primary mechanism may actually be reduction of pre-sleep anxiety and hyperarousal, which itself takes 1-2 weeks of consistent use to manifest, and the better sleep is a secondary consequence of less hyperaroused state
The practical implications are substantial. Patients who try valerian "the night before a big presentation" and report it didn't work are correctly describing what valerian does — it doesn't work on the night of, only after sustained use. Patients who try a two-week trial at 600-900 mg of a standardized 0.8% valerenic acid extract one hour before bed typically get a more accurate impression of whether valerian works for them as an individual. This has clinical implications for direct-to-consumer marketing (which tends to imply night-of effect, setting up disappointment) and for clinician guidance (a clinician recommending valerian should explicitly frame it as a two-week trial, not a one-night test). For the contrast with prescription hypnotics that do work on the first night, see our Insomnia page.
Key Research Papers
- Bent S et al. (2006). Valerian for sleep: a systematic review and meta-analysis. American Journal of Medicine. — PubMed
- Donath F et al. (2000). Critical evaluation of the effect of valerian extract on sleep structure and sleep quality. Pharmacopsychiatry. — PubMed
- Leathwood PD et al. (1985). Aqueous extract of valerian root improves sleep quality in man. Pharmacology, Biochemistry, and Behavior. — PubMed
- Andreatini R et al. (2002). Effect of valepotriates (valerian extract) in generalized anxiety disorder. Phytotherapy Research. — PubMed
- Mirabi P et al. (2011). Effects of valerian on the severity and systemic manifestations of dysmenorrhea. International Journal of Gynaecology and Obstetrics. — PubMed
PubMed Topic Searches
- PubMed: Valerian sleep latency / insomnia trials
- PubMed: Valerenic acid GABA receptor
- PubMed: Valepotriate toxicology
- PubMed: Valerian and anxiety
- PubMed: Valerian and dysmenorrhea
External Authoritative Resources
- NIH Office of Dietary Supplements — Valerian Fact Sheet (Health Professionals) — the most authoritative single summary of valerian pharmacology, clinical trials, and safety
- NCCIH (National Center for Complementary and Integrative Health) — Valerian
- European Medicines Agency — Valerianae radix monograph (HMPC traditional-use registration)
- MedlinePlus — Valerian
- PubMed — All research on Valeriana officinalis (~2,000+ papers)
Connections
- Valerian (Main Page)
- Valerian for Sleep Quality
- Valerian for Anxiety Relief
- Valerian for Muscle Relaxation
- Valerian for Menstrual Cramps
- Passionflower
- Lemon Balm
- Chamomile
- Lavender
- Kava
- Ashwagandha
- Rhodiola Rosea
- Magnesium
- Magnesium Glycinate
- Insomnia
- Anxiety
- Depression
- Stress Management
- Sleep Hygiene
- Natural Anxiety Relief
- Cramp Prevention