Pau d'Arco for Anti-Inflammatory Effects
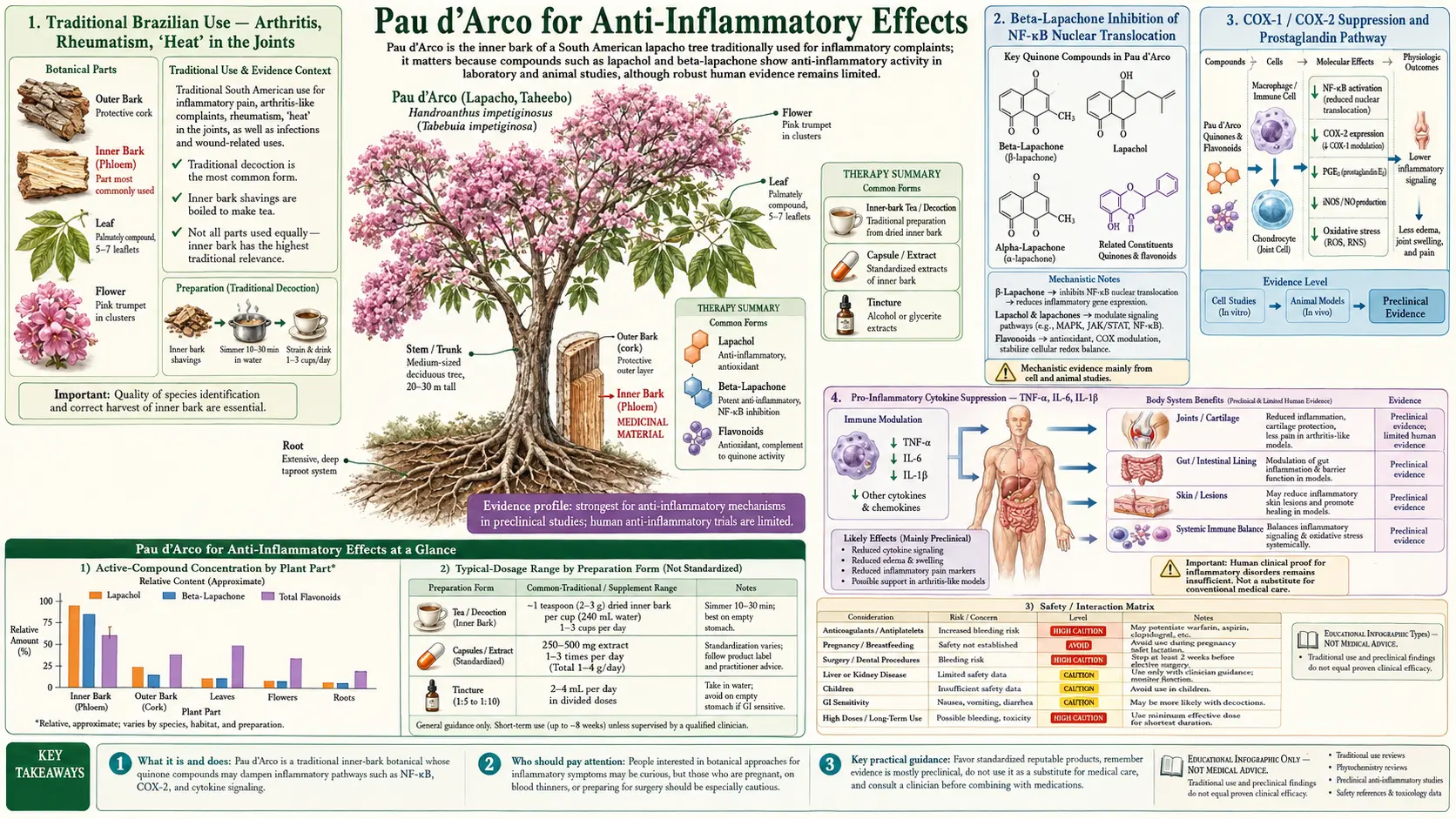
Pau d'Arco has a deep traditional reputation in Brazilian and Argentinian folk medicine for joint pain, arthritis, low-back pain, "rheumatism," chronic boils, and a wide range of inflammatory skin conditions — uses that closely parallel its modern in-vitro and in-vivo profile as an NF-κB inhibitor and cyclooxygenase suppressor. Beta-lapachone, the more potent of the two principal naphthoquinones, blocks the IκB-kinase complex that normally releases NF-κB p65 from cytoplasmic restraint, preventing its translocation to the nucleus and suppressing transcription of TNF-α, IL-6, IL-1β, COX-2, iNOS, and several adhesion molecules. The mechanism overlaps directly with curcumin, boswellic acids, resveratrol, and the parthenolide of feverfew. This deep-dive walks through the molecular pharmacology, the traditional Brazilian arthritis preparations, the realistic dose ranges, and where Pau d'Arco does — and does not — fit alongside the conventional anti-inflammatory drug classes.
Table of Contents
- Traditional Brazilian Use — Arthritis, Rheumatism, "Heat" in the Joints
- Beta-Lapachone Inhibition of NF-κB Nuclear Translocation
- COX-1 / COX-2 Suppression and Prostaglandin Pathway
- Pro-Inflammatory Cytokine Suppression — TNF-α, IL-6, IL-1β
- iNOS and Nitric Oxide Modulation in Chronic Inflammation
- Practical Applications — Osteoarthritis, Rheumatoid Arthritis, Gout, Bursitis
- Inflammatory Bowel Conditions — Theoretical Application and Realistic Limits
- Inflammatory Skin Conditions — Psoriasis, Eczema, Chronic Dermatitis
- Dosing for Anti-Inflammatory Effect
- Combining with Curcumin, Boswellia, Omega-3, and Other Anti-Inflammatory Agents
- Cautions Specific to Anti-Inflammatory Use
- Key Research Papers
- Connections
- Featured Videos
Traditional Brazilian Use — Arthritis, Rheumatism, "Heat" in the Joints
The traditional Brazilian and Argentinian use of Pau d'Arco for arthritis and rheumatic complaints is one of the most consistent threads in the South American materia medica. The Tupi-Guaraní healers of the lowland forests, the Kallawaya of the high Andes, and the Portuguese-Brazilian rural folk tradition all converge on the same indications: hot, swollen, painful joints; chronic low-back pain that worsens with weather change; "rheumatism" of the hands and shoulders; chronic gout flares; and the diffuse joint pain that often accompanies recurrent fever and infection.
The traditional preparation is generally an oral decoction of cut inner bark — 2 tablespoons of bark per quart of water, simmered 15-20 minutes, drunk as 2-4 cups daily over weeks to months. Topical poultices of warm, moist bark were also applied directly over the painful joint, sometimes wrapped in a wool cloth to retain heat. For gout specifically, the recommendation was often a combination of the oral decoction with dietary modification (reducing organ meats, sardines, beer — the same purine-source modifications a modern gout dietitian would recommend).
The herb was selected for inflammatory joint complaints in part because of its observable effect — pain and swelling visibly improved over 2-4 weeks of continuous use — and in part because of its traditional categorization as a "cooling" herb that reduced "heat" in the affected tissue. The cooling framing maps imperfectly but recognizably onto modern anti-inflammatory pharmacology.
Beta-Lapachone Inhibition of NF-κB Nuclear Translocation
NF-κB (nuclear factor kappa-light-chain-enhancer of activated B cells) is the master transcription factor of inflammation. In resting cells, the active p65/p50 heterodimer is held inactive in the cytoplasm by binding to IκB inhibitor proteins. When the cell receives an inflammatory signal (TNF receptor engagement, Toll-like receptor activation, oxidative stress, certain cytokines), the IκB-kinase (IKK) complex phosphorylates IκB, marking it for proteasomal degradation. Free NF-κB then translocates to the nucleus, where it binds κB response elements in the promoter regions of hundreds of inflammatory target genes: TNF-α, IL-6, IL-1β, COX-2, iNOS, ICAM-1, VCAM-1, E-selectin, and many more.
Beta-lapachone has been shown in multiple cell-line studies (macrophages, hepatocytes, synoviocytes, keratinocytes) to inhibit NF-κB activation at concentrations in the 1-10 μM range. The mechanism involves direct interference with the IκB-kinase complex, with downstream consequences for the entire NF-κB-dependent inflammatory gene set. Importantly, the inhibition is most pronounced at sub-cytotoxic concentrations — making this a genuine pharmacologic effect rather than a non-specific consequence of cell stress.
The mechanistic overlap with other natural NF-κB inhibitors is striking:
- Curcumin (from turmeric) inhibits IKK and p65 nuclear translocation through similar but not identical mechanisms
- Resveratrol (from grapes, polygonum cuspidatum) inhibits NF-κB through SIRT1-dependent and -independent pathways
- Parthenolide (from feverfew) covalently modifies cysteine residues in IKKβ
- EGCG (from green tea) inhibits p65 nuclear translocation
- Boswellic acids (from Boswellia serrata) inhibit 5-lipoxygenase and also have NF-κB effects
This shared mechanism explains why these herbs are often combined in clinical practice — their effects on the NF-κB node are at least partly additive, and the redundancy reduces the chance that an individual patient's pharmacogenomic variation will prevent benefit.
COX-1 / COX-2 Suppression and Prostaglandin Pathway
Cyclooxygenase (COX) is the enzyme that converts arachidonic acid to prostaglandin H2, the precursor of all downstream prostaglandins and thromboxane. COX-1 is constitutively expressed in most tissues and produces the prostaglandins responsible for gastric mucus protection, renal blood flow autoregulation, and platelet aggregation. COX-2 is the inducible form upregulated in inflammation and is the target of selective NSAIDs like celecoxib (Celebrex).
Beta-lapachone has documented suppression of COX-2 expression at the transcriptional level (through NF-κB inhibition, since the COX-2 gene is NF-κB-regulated) and to a lesser extent direct enzymatic inhibition. The net effect is reduced prostaglandin E2 production in inflamed tissue, which is the primary driver of the swelling, redness, warmth, and pain of inflammation.
The COX-2-preferential profile is clinically attractive because it suggests potential anti-inflammatory benefit without the gastric and platelet effects of COX-1 inhibition (which is why most patients on chronic ibuprofen develop gastric irritation or risk GI bleeding). However, this comparison should not be overstated — the absolute potency of Pau d'Arco's COX-2 effect at oral doses achievable in humans is far below that of celecoxib or ibuprofen. Pau d'Arco is best thought of as a mild, broad-spectrum anti-inflammatory adjunct, not a replacement for NSAID therapy in significant inflammatory disease.
Pro-Inflammatory Cytokine Suppression — TNF-α, IL-6, IL-1β
The pro-inflammatory cytokines TNF-α, IL-6, and IL-1β are the central mediators of the systemic inflammatory response. They are produced primarily by activated macrophages and monocytes in response to infection or tissue damage, and they orchestrate fever, acute-phase protein production by the liver, neutrophil recruitment, and the malaise of acute and chronic inflammation. They are also the molecular drivers of several major chronic inflammatory diseases — TNF-α is the target of adalimumab (Humira), infliximab (Remicade), and etanercept (Enbrel); IL-6 is the target of tocilizumab (Actemra); IL-1β is the target of canakinumab (Ilaris).
Beta-lapachone reduces the production of all three cytokines in stimulated macrophage cell lines and in murine inflammation models, again at sub-cytotoxic concentrations and through the NF-κB mechanism. The magnitude of the effect in vitro is comparable to other plant NF-κB inhibitors but, again, far below that of monoclonal antibody biologics. The clinical implication is that Pau d'Arco can modestly damp the chronic low-grade inflammation of conditions like osteoarthritis, mild rheumatoid arthritis, and chronic skin inflammation — but it is not a substitute for biologic DMARD therapy in moderate-to-severe rheumatoid arthritis, severe psoriasis, or active inflammatory bowel disease.
For patients on biologic therapy who want to add a mild plant adjunct, Pau d'Arco is generally well tolerated — but the addition should be discussed with the treating rheumatologist or gastroenterologist, particularly because of the anticoagulation interaction and the immune-modulating effects (see the Cautions & Cancer Research page).
iNOS and Nitric Oxide Modulation in Chronic Inflammation
Inducible nitric oxide synthase (iNOS, encoded by the NOS2 gene) is the enzyme that produces large amounts of nitric oxide (NO) in activated macrophages and other inflammatory cells. iNOS is NF-κB-regulated and is upregulated in chronic inflammatory tissue. While NO has many physiologic roles (the constitutive eNOS produces small amounts of NO for vascular smooth muscle relaxation), the large amounts produced by iNOS in chronic inflammation contribute to tissue damage and the perpetuation of the inflammatory state.
Beta-lapachone's NF-κB inhibition translates to reduced iNOS expression and reduced NO production in inflammatory cells. This effect has been documented in macrophage cell lines, in murine arthritis models, and in cell-line models of inflammatory bowel disease. The reduction is modest but consistent.
This is part of a broader pattern in the integrative-medicine literature in which several plant-derived NF-κB inhibitors (Pau d'Arco, curcumin, boswellic acids, EGCG, resveratrol) collectively produce a "broadly anti-inflammatory" effect through coordinated suppression of cytokines, COX-2, iNOS, and adhesion molecules. The strategy of using multiple complementary plant agents at modest doses rather than a single agent at high dose is one of the operating principles of much of clinical herbalism, and it is largely supported by the molecular pharmacology.
Practical Applications — Osteoarthritis, Rheumatoid Arthritis, Gout, Bursitis
For the practical patient with inflammatory joint disease, where does Pau d'Arco actually fit?
- Mild-to-moderate osteoarthritis — reasonable adjunct alongside the standard triad of exercise, weight management, and topical or oral NSAID as needed. Typical dose: 500-1,000 mg standardized extract twice daily for 12 weeks, then reassess. Often combined with curcumin 500 mg twice daily, omega-3 fish oil 2-3 g daily, and glucosamine + chondroitin. Expect modest pain reduction and possibly modest reduction in NSAID requirement.
- Rheumatoid arthritis — complementary to (NOT a substitute for) DMARD therapy. Discuss with the treating rheumatologist. Particularly worth considering for patients with milder seropositive RA on methotrexate alone, where adding low-grade anti-inflammatory adjuncts can help with breakthrough symptoms without escalating immunosuppression. NOT appropriate as monotherapy for active RA.
- Gout — the traditional indication has a basis — modest anti-inflammatory effect — but does NOT replace allopurinol or febuxostat for uric acid lowering, and does not replace colchicine or NSAID for acute flare management. Worth considering as an adjunct for chronic interval management alongside dietary purine restriction. See Gout.
- Bursitis and tendinitis — mild adjunct, more useful for chronic recurrent forms than for acute flares. Topical bark decoction warm compresses can be added to oral therapy. Generally takes 3-6 weeks of consistent use for measurable effect.
- Polymyalgia rheumatica — the standard therapy is low-dose prednisone, and Pau d'Arco is not a substitute. May have modest adjunctive value for patients trying to minimize the prednisone dose, but not a primary intervention.
- Lyme arthritis — the antimicrobial and immune-modulating mechanisms make Pau d'Arco one of several plant adjuncts that integrative Lyme practitioners use alongside antibiotics. See Lyme Disease.
Inflammatory Bowel Conditions — Theoretical Application and Realistic Limits
The NF-κB and cytokine suppression mechanisms of Pau d'Arco are mechanistically attractive for inflammatory bowel disease (IBD), but the practical application is more nuanced than for joint disease. Active ulcerative colitis and active Crohn's disease require evidence-based induction therapy (5-aminosalicylates, corticosteroids, immunomodulators, biologics) and are not appropriate settings for plant-based monotherapy.
Pau d'Arco may have a role in:
- Mild interval management of IBD in remission, alongside maintenance 5-ASA therapy, gut-healing nutrients, and dietary modification
- Microscopic colitis (lymphocytic, collagenous) as part of an integrative protocol after gastroenterology evaluation
- Post-infectious irritable bowel syndrome with low-grade inflammatory component
- Functional bowel patterns with concurrent suspected fungal overgrowth — here the dual antifungal + anti-inflammatory profile is potentially additive
The cautions for IBD use are real: paradoxically, the same naphthoquinone redox-cycling that delivers therapeutic benefit can also irritate inflamed gut mucosa at higher doses, producing diarrhea or worsening symptoms. Start at the low end of the dose range (500 mg standardized extract once daily with food), titrate slowly, and discontinue immediately for any worsening. Patients with active flares of IBD should defer plant-medicine experimentation until remission is achieved.
For more on gut-related interventions, see Gut Healing and Crohn's Disease.
Inflammatory Skin Conditions — Psoriasis, Eczema, Chronic Dermatitis
The dual antifungal and anti-inflammatory profile of Pau d'Arco translates well to several inflammatory skin conditions where chronic low-grade fungal contribution is part of the picture:
- Seborrheic dermatitis — the chronic flaky red rash of the scalp, eyebrows, and nasolabial folds is driven by Malassezia yeast colonization plus an inflammatory response to it. Topical Pau d'Arco decoction or salve combines antifungal (against Malassezia) and anti-inflammatory effects directly at the site. Often combined with topical zinc pyrithione or ketoconazole shampoo.
- Psoriasis — the chronic NF-κB-driven plaque-forming inflammatory skin disease. Pau d'Arco at oral doses contributes mild systemic NF-κB suppression. Topical preparations can be applied directly to plaques. NOT a substitute for biologic therapy in moderate-severe psoriasis but worth considering as an adjunct in mild disease or for patients trying to delay biologic initiation.
- Atopic dermatitis (eczema) — particularly for patients with eczema and concurrent gut candidiasis or recurrent skin yeast infection, the dual mechanism is useful. The Th2-dominant pattern of allergic eczema may also benefit from the Th1-shifting effect (see Immune Modulation page).
- Acne (inflammatory rather than comedonal) — the anti-inflammatory and modest antimicrobial effects against Cutibacterium acnes make Pau d'Arco a reasonable adjunct for inflammatory acne. NOT a substitute for tretinoin, benzoyl peroxide, or oral antibiotic / isotretinoin therapy for moderate-severe disease. See Acne.
- Chronic urticaria — the chronic histamine-driven hive condition with some inflammatory component. Mild adjunct, results variable.
Dosing for Anti-Inflammatory Effect
The anti-inflammatory dose range for Pau d'Arco is generally at the lower end of the overall dose range:
- Standardized extract capsule: 500-1,500 mg of dried-bark equivalent twice daily, with meals. Aim for products standardized to 3-10% combined naphthoquinones. The lower end of this range (500 mg twice daily of an 8% standardized product) is often sufficient for anti-inflammatory effect; the higher end is more appropriate when there is concurrent antifungal target.
- Alcohol tincture (1:5 in 40-50% ethanol): 3-6 mL twice daily, diluted in water or juice.
- Decoction: 2-3 cups daily of the standard preparation (2 tbsp bark per quart of water, simmered 15-20 minutes). The lowest-potency form — useful for general tonic anti-inflammatory effect, less useful for active inflammatory flare.
Expect 2-6 weeks for measurable effect on chronic inflammatory conditions. Pau d'Arco is not appropriate as an acute flare intervention — it has no rapid pharmacologic effect comparable to ibuprofen or prednisone. Use it as steady-state tonic management, with conventional anti-inflammatory drugs available for acute flares as needed.
Continuous use beyond 12 weeks is generally not recommended without breaks — take 1-2 weeks off every 8-12 weeks to prevent tachyphylaxis and to allow assessment of whether continued use is still providing benefit. Many patients find that intermittent 8-12 week courses with 2-4 week breaks provide better long-term efficacy than continuous indefinite dosing.
Combining with Curcumin, Boswellia, Omega-3, and Other Anti-Inflammatory Agents
The most pragmatic clinical strategy for chronic inflammatory disease is combination of multiple complementary mechanisms at modest doses, rather than mono-therapy at high dose. Pau d'Arco fits well into combination protocols:
- Curcumin — the most-studied plant NF-κB inhibitor. 500-1,000 mg twice daily of a bioavailability-enhanced formulation (Meriva, Theracurmin, or with piperine). Mechanistically additive with Pau d'Arco.
- Boswellia serrata (boswellic acids) — selective 5-lipoxygenase inhibition reduces leukotrienes (the inflammatory mediators not addressed by NSAIDs). 300-500 mg of standardized extract (typically AKBA-enriched) twice daily.
- Omega-3 fish oil (EPA + DHA) — substrate competition with arachidonic acid for COX and LOX enzymes; resolvins and protectins as actively pro-resolving mediators. 2-3 g combined EPA+DHA daily. See Omega-3 Fatty Acids.
- Bromelain — pineapple stem proteolytic enzyme with bradykinin and complement modulation. Useful for acute inflammation and post-surgical recovery. 500 mg twice daily between meals.
- Quercetin — flavonoid with mast cell stabilization and modest NF-κB effect. Particularly useful for allergic-inflammatory patterns. 500-1,000 mg twice daily.
- SAMe (S-adenosylmethionine) — methyl donor with documented anti-inflammatory effect in osteoarthritis. 400-1,200 mg daily.
- Magnesium glycinate — magnesium deficiency exacerbates many inflammatory conditions; the glycinate form is well tolerated. 200-400 mg elemental magnesium at bedtime.
A typical "chronic OA / mild RA / chronic inflammatory pain" stacking protocol might include Pau d'Arco 500 mg twice daily + curcumin 500 mg twice daily + boswellia 300 mg twice daily + omega-3 2 g daily, alongside conventional NSAID or DMARD as needed. The expectation is modest steady-state improvement and possibly reduced NSAID dose requirement, not pharmaceutical-grade rapid pain relief.
Cautions Specific to Anti-Inflammatory Use
Most cautions are covered in detail on the Cautions & Cancer Research page. Anti-inflammatory use brings a few specific concerns:
- Concurrent NSAID use — Pau d'Arco does not reduce the gastric or renal toxicity of NSAIDs. Patients taking chronic ibuprofen or naproxen still need gastroprotection (proton pump inhibitor or H2 blocker) and renal monitoring as appropriate.
- Concurrent anticoagulant use — this is the most consequential interaction. NSAIDs already increase bleeding risk; adding beta-lapachone, which has its own vitamin-K-antagonist functional similarity to warfarin, compounds the risk substantially. Discontinue Pau d'Arco at least 2 weeks before any planned surgical procedure.
- Concurrent corticosteroid use — no direct interaction documented, but corticosteroids already provide substantial NF-κB inhibition through their genomic mechanism. Adding Pau d'Arco may provide modest additive effect.
- Concurrent biologic DMARD use — discuss with treating rheumatologist or gastroenterologist before adding Pau d'Arco. The immune-modulating effects could theoretically interact with biologic mechanism, though no specific interactions have been clinically documented.
- Pregnancy — absolute contraindication for any indication, including arthritis. Pregnant patients with arthritis should work with maternal-fetal medicine and rheumatology on pregnancy-compatible alternatives.
- Liver function — both Pau d'Arco and many anti-inflammatory drugs (methotrexate, leflunomide, sulfasalazine, chronic NSAIDs) can affect liver function. Periodic liver function testing is appropriate when combining.
Key Research Papers
- Lee JI, Choi DY, Chung HS, Seo HG, Woo HJ, Choi BT, Choi YH (2006). beta-Lapachone induces growth inhibition and apoptosis in human cancer cells (NF-κB context). Phytotherapy Research. — PubMed
- Moon DO et al. (2007). beta-Lapachone inhibits TNF-induced NF-kappaB activation. Free Radical Biology and Medicine. — PubMed
- de Almeida ER, da Silva Filho AA, dos Santos ER, Lopes CA (1990). Anti-inflammatory action of lapachol. Journal of Ethnopharmacology. — PubMed
- Choi YH et al. (2003). beta-Lapachone induces apoptosis in human prostate cancer cells through NF-kappaB pathway modulation. Cancer Letters. — PubMed
- Aggarwal BB, Sung B (2009). Pharmacological basis for the role of curcumin in chronic diseases: an age-old spice with modern targets (NF-κB mechanism background applicable to Pau d'Arco). Trends in Pharmacological Sciences. — PubMed
- Kung HN et al. (2014). beta-Lapachone modulates inflammation. Toxicology and Applied Pharmacology. — PubMed
- Bonifazi EL et al. (2010). Naphthoquinones and inflammation review. Mini-Reviews in Medicinal Chemistry. — PubMed
- Hu R et al. (2011). Nrf2 induction by beta-lapachone (phase-2 antioxidant gene induction context). Cancer Research. — PubMed
- Kim SO et al. (2007). beta-Lapachone suppresses COX-2 expression. Biochemical and Biophysical Research Communications. — PubMed
- Hwang JH et al. (2008). Tabebuia avellanedae and inflammatory cytokine suppression. Phytotherapy Research. — PubMed
- Goel A et al. (2008). Curcumin as "Curecumin": from kitchen to clinic. Biochemical Pharmacology. — PubMed
- Sethi G, Sung B, Aggarwal BB (2008). TNF: a master switch for inflammation to cancer (background on the TNF-α-driven inflammation that Pau d'Arco modulates). Frontiers in Bioscience. — PubMed
PubMed Topic Searches
- PubMed: beta-Lapachone NF-kB / inflammation
- PubMed: Lapachol COX / prostaglandin
- PubMed: Tabebuia for arthritis
- PubMed: Naphthoquinone cytokine suppression
- PubMed: Pau d'Arco traditional arthritis use
Connections
- Pau d'Arco Overview
- Pau d'Arco Benefits Hub
- Pau d'Arco — Antifungal
- Pau d'Arco — Immune Modulation
- Pau d'Arco — Cautions & Cancer Research
- Turmeric (Curcumin)
- Boswellia
- Omega-3 Fatty Acids
- Rheumatoid Arthritis
- Osteoarthritis
- Gout
- Psoriasis
- Eczema
- Gut Healing
- Oxidative Stress