Pau d'Arco for Antifungal Effects
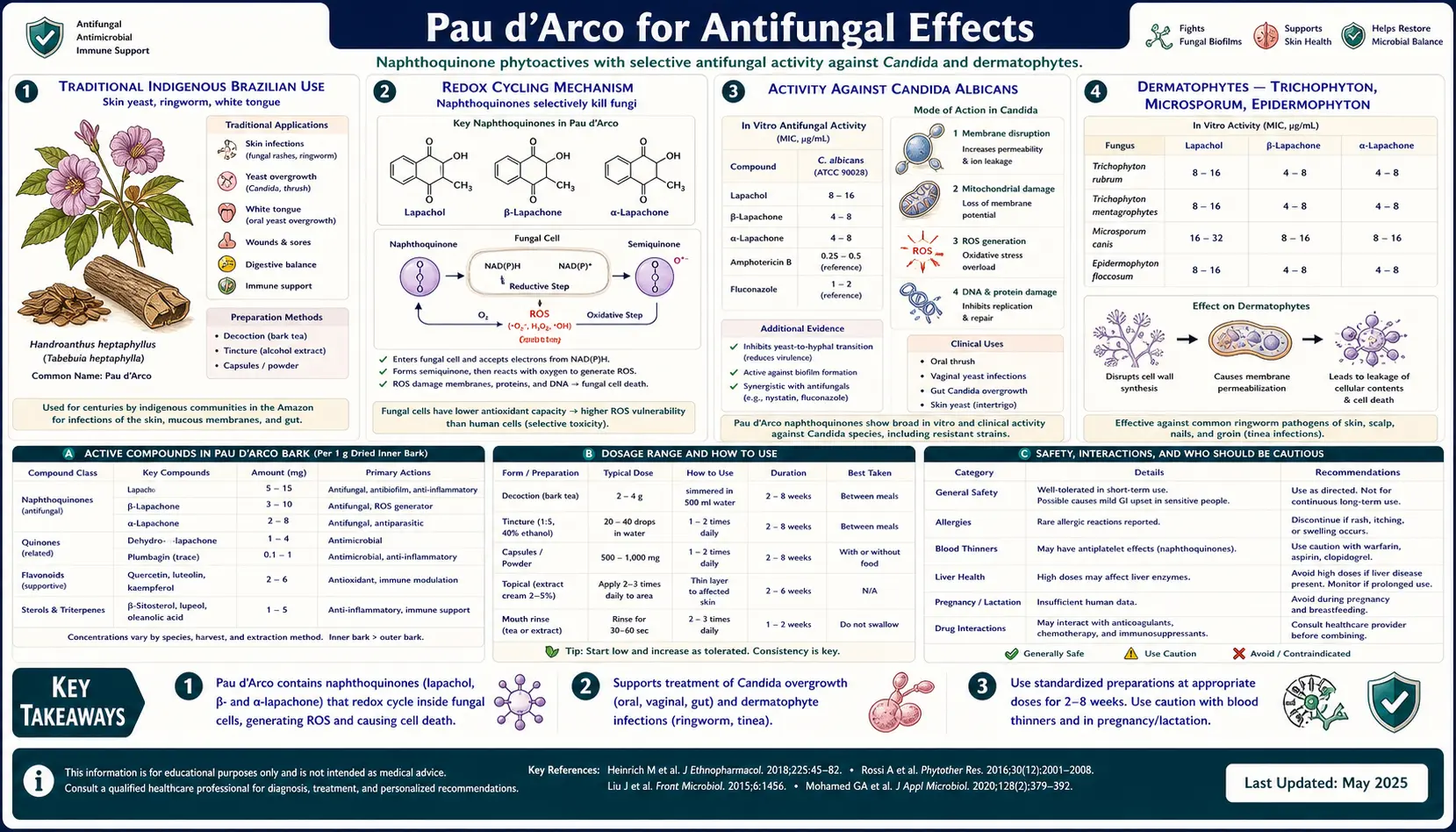
Pau d'Arco's most consistent and best-documented activity is antifungal. The two principal naphthoquinones — lapachol and beta-lapachone — show in-vitro minimum inhibitory concentrations (MICs) against Candida albicans, Candida glabrata, Trichophyton mentagrophytes, Microsporum gypseum, and several Aspergillus species that fall within the same order of magnitude as several pharmaceutical antifungals. Brazilian and Argentinian Indigenous peoples have used inner-bark decoctions topically for ringworm, athlete's foot, jock itch, vaginal yeast, and "white tongue" (oral candidiasis) for centuries, and standardized Pau d'Arco extracts now sit alongside caprylic acid, undecylenic acid, and oregano oil in virtually every modern "candida diet" anti-fungal supplement protocol. This page walks through the mechanism, the in-vitro and in-vivo evidence, the traditional preparations, the modern dosing patterns, and the safety boundaries.
Table of Contents
- Traditional Indigenous Brazilian Use — Skin Yeast, Ringworm, and "White Tongue"
- Redox Cycling Mechanism — Why Naphthoquinones Selectively Kill Fungi
- Activity Against Candida albicans
- Dermatophytes — Trichophyton, Microsporum, Epidermophyton
- Activity Against Aspergillus, Cryptococcus, and Other Molds
- Topical Preparations — Decoctions, Sitz Baths, Suppositories, Salves
- Oral "Candida Diet" Protocols — How Pau d'Arco Fits With Caprylic Acid, Undecylenic Acid, and Oregano
- Practical Dosing — Bark Decoction, Tincture, Standardized Capsule
- Quality & Standardization — Why Most Commercial Products Are Underpotent
- Cautions Specific to the Antifungal Use
- Key Research Papers
- Connections
- Featured Videos
Traditional Indigenous Brazilian Use — Skin Yeast, Ringworm, and "White Tongue"
Pau d'Arco's traditional reputation as an antifungal predates any biochemistry by several centuries. The Guaraní people of southern Brazil and Paraguay called the tree tajy (meaning "to have strength" or "vigor") and used the inner bark as a topical wash for ringworm, athlete's foot, jock itch, scabies, and infected wounds. The Kallawaya healers of the Bolivian Andes — one of the few continuously transmitted traditional medicine lineages from the pre-Columbian era — carried Pau d'Arco inner bark on their travels as a remedy for skin infection, fever, and dysentery. In the rainforest highlands of Argentina and Paraguay, lapacho tea (called lapacho colorado or tajy) was given by mouth and applied topically for what we would now recognize as cutaneous candidiasis and oral thrush.
The Portuguese-Brazilian rural folk medicine tradition (medicina popular) inherited and extended these uses. Standard 20th-century Brazilian herbals (Cruz, da Silva, and others) catalog Pau d'Arco for: vaginal candidiasis (douche or sitz bath of decoction), oral thrush (mouthwash), denture stomatitis, intertriginous yeast in skin folds, diaper dermatitis with secondary Candida, athlete's foot, ringworm of the scalp and body, and onychomycosis (fungal nail). The form varied — sometimes the powdered bark was sprinkled directly on weeping fungal skin lesions, sometimes a strong decoction was used as a wash, sometimes a tincture in cane alcohol (cachaça) was painted onto the lesion.
This breadth of traditional fungal indications is unusual. Most plant antifungals in the global ethnobotany have one or two specific indications — Pau d'Arco's pan-fungal reputation parallels its laboratory profile, where the naphthoquinone mechanism is genuinely active against most fungal genera tested.
Redox Cycling Mechanism — Why Naphthoquinones Selectively Kill Fungi
Lapachol and beta-lapachone are 1,4-naphthoquinones — planar bicyclic molecules with two carbonyl groups on the same ring. This structural class is a classic redox cycler: the quinone accepts one electron from cellular NAD(P)H (catalyzed by flavin reductases such as NQO1, cytochrome b5 reductase, and several mitochondrial enzymes) to form an unstable semiquinone radical. The semiquinone in turn transfers its unpaired electron to molecular oxygen, regenerating the parent quinone and releasing a superoxide anion (O&sub2;−). The cycle then repeats — a single naphthoquinone molecule can catalyze the production of many superoxide radicals before being permanently consumed.
Superoxide and its downstream products (hydrogen peroxide, hydroxyl radical) damage lipids, proteins, and DNA. Mammalian cells maintain elaborate antioxidant defenses (reduced glutathione at ~5 mM in cytoplasm, superoxide dismutase, catalase, glutathione peroxidase, the thioredoxin system, and the Nrf2-regulated phase-2 detoxification gene set). At the doses produced by oral Pau d'Arco intake, normal mammalian cells handle the redox load without measurable damage.
Fungi have antioxidant systems, but they are quantitatively weaker and qualitatively different. Candida albicans, for instance, relies heavily on its catalase (encoded by the CAT1 gene) and on glutathione, but lacks selenium-dependent glutathione peroxidase, lacks the same diversity of glutathione-S-transferase isoforms, and has a smaller cytoplasmic glutathione pool. The fungal cell wall and membrane composition (ergosterol rather than cholesterol; chitin rather than glycocalyx) is also more permeable to lipophilic naphthoquinones than the mammalian plasma membrane. The net result: at the redox-stress concentration that triggers fungal cell death, mammalian cells experience an antioxidant load they can detoxify.
The selectivity index (mammalian-cytotoxic-IC&sub5;&sub0; divided by fungal-MIC) for lapachol against Candida albicans in cultured human keratinocyte / yeast co-culture is typically 10-30 — high enough to support topical therapeutic use and oral use at conservative doses, but not high enough to justify the megadoses required for antitumor effect (see the Cautions & Cancer Research page for the NCI lapachol Phase I termination story).
Activity Against Candida albicans
Candida albicans is the most-studied target of Pau d'Arco. In-vitro MIC values for lapachol and beta-lapachone against laboratory strains of C. albicans typically fall in the 4-32 μg/mL range, comparable to or modestly weaker than fluconazole (MIC typically 0.5-8 μg/mL for susceptible isolates) but with a fundamentally different mechanism — redox stress rather than ergosterol synthesis inhibition — so cross-resistance with the azole drug class is not expected.
Several Brazilian and Korean laboratory groups have shown that beta-lapachone, in particular, is fungicidal (kills the organism) rather than merely fungistatic (inhibits growth) at modestly higher concentrations — an important distinction because fluconazole and the other azoles are fungistatic against Candida, allowing the surviving organism population to develop resistance over the course of repeated treatment. The fungicidal mode of action of beta-lapachone, mediated by overwhelming intracellular oxidative damage, is less likely to select for resistance.
Candida glabrata — the second most common Candida species in human infection and the species most prone to intrinsic fluconazole resistance — also shows in-vitro susceptibility to lapachol and beta-lapachone in the same general MIC range. This is clinically relevant for patients with recurrent vaginal candidiasis or denture stomatitis who have already failed multiple courses of fluconazole.
The non-albicans Candida species — krusei, tropicalis, parapsilosis — have been less systematically tested, but published susceptibility data are consistent with broad activity within the genus.
Dermatophytes — Trichophyton, Microsporum, Epidermophyton
The dermatophyte genera that cause ringworm (tinea corporis), athlete's foot (tinea pedis), jock itch (tinea cruris), scalp ringworm (tinea capitis), and fungal nail infection (onychomycosis) are all keratinophilic fungi that colonize the stratum corneum. They are notoriously difficult to clear with topical therapy because they live inside the keratin layer where azole creams penetrate poorly, and oral terbinafine for nail or scalp infection requires 6-12 weeks of treatment with associated hepatotoxicity risk.
Lapachol and beta-lapachone have published in-vitro MIC values against Trichophyton mentagrophytes, Trichophyton rubrum, Microsporum gypseum, and Epidermophyton floccosum that are typically 2-16 μg/mL — in the same general range as terbinafine. Topical Pau d'Arco preparations (bark decoction, tincture in alcohol, or salve in shea butter or coconut oil base) have a long traditional use for these conditions. The lipophilic naphthoquinones penetrate the stratum corneum well, and the redox-stress mechanism is active against dormant arthroconidia (the resistant spore form) as well as actively growing hyphae — in contrast to azoles, which are largely active only against the growing hyphal form.
Practical traditional topical preparation: a strong decoction (2 tablespoons of cut bark per cup of water, simmered 20 minutes, cooled) applied with a cotton ball to affected skin twice daily, allowed to dry without rinsing. For nail infection, the bark powder can be mixed with petroleum jelly or shea butter to a 10% (w/w) suspension and applied nightly under occlusion. Expect 2-6 weeks for skin lesions to clear and 6-12 months for nail.
Activity Against Aspergillus, Cryptococcus, and Other Molds
Aspergillus species — especially A. fumigatus, A. niger, and A. flavus — are filamentous molds that cause allergic bronchopulmonary aspergillosis, sinus aspergilloma, and invasive aspergillosis in immunocompromised patients. Lapachol and beta-lapachone have published in-vitro activity against all three at MICs in the 8-64 μg/mL range — weaker than voriconazole or amphotericin B, but with the same redox-cycling mechanism rather than ergosterol inhibition or pore formation.
The clinical relevance is most concrete for the chronic allergic/colonizing scenarios (e.g., Aspergillus-driven chronic rhinosinusitis, mold colonization in chronic damp-building exposure) where standard antifungals are either not indicated or have failed. In these scenarios, oral Pau d'Arco extract is sometimes part of an integrative protocol alongside mold avoidance, nasal lavage, and binders for mycotoxins (see Mold & Mycotoxins). It is not a substitute for systemic antifungal therapy in invasive aspergillosis — that is a medical emergency requiring voriconazole or echinocandin.
Cryptococcus neoformans (the cause of cryptococcal meningitis in HIV/AIDS) has documented in-vitro susceptibility to beta-lapachone at concentrations comparable to fluconazole, but no clinical data exist and this is also a setting requiring proven systemic therapy.
Topical Preparations — Decoctions, Sitz Baths, Suppositories, Salves
Topical Pau d'Arco preparations are the most traditional use and the most direct application of the antifungal activity. The cell wall and stratum corneum penetration of the lipophilic naphthoquinones is favorable, and topical use avoids the systemic toxicity concerns that arise with higher oral doses.
- Decoction for skin and scalp — 2 tablespoons of cut inner bark per cup of water, simmered 15-20 minutes (not just steeped — naphthoquinones extract better with sustained heat), cooled, applied to affected skin with a cotton ball 2-3× daily. For scalp ringworm, the decoction can be massaged into the scalp after shampooing and left to dry. Refrigerate the unused decoction; discard after 3-4 days.
- Sitz bath for vaginal yeast or perineal candidiasis — 1/2 cup of cut bark simmered 30 minutes in 1 quart of water, strained, added to a shallow bath of warm water in a basin large enough to sit in. Use nightly for 7-14 days. Stop if irritation develops.
- Vaginal suppositories — commercially available from some specialty herb companies; typically 200-400 mg of standardized Pau d'Arco extract in a cocoa butter or coconut oil base. Insert nightly for 7 nights. Less well-studied than oral therapy but with a long Brazilian folk tradition.
- Salve for athlete's foot and ringworm — the powdered bark (10-20% by weight) mixed into a shea butter, coconut oil, or beeswax-and-oil base. Apply nightly. The lipid vehicle improves stratum corneum penetration.
- Mouthwash for oral thrush and denture stomatitis — cooled decoction (same recipe as for skin), swished in the mouth for 60 seconds 3-4× daily, then spat out. Do not swallow large amounts (small accidental ingestion of mouthwash is fine).
- Direct bark powder application — the traditional Brazilian use for weeping fungal skin lesions or diaper-area candidiasis is direct sprinkling of finely powdered bark onto the affected area, kept in place by gauze. The powder draws moisture and delivers the active compounds at high local concentration.
None of these topical preparations have been formally evaluated in modern randomized trials — the evidence base is centuries of Brazilian and Andean folk use, in-vitro MIC data, and clinical experience reports from herbalists and integrative practitioners.
Oral "Candida Diet" Protocols — How Pau d'Arco Fits With Caprylic Acid, Undecylenic Acid, and Oregano
The modern "candida diet" anti-fungal protocol — popularized in the 1980s by William Crook (The Yeast Connection) and the integrative medicine community — targets suspected intestinal candidal overgrowth with simultaneous dietary sugar restriction, probiotic repopulation, and a rotation of plant-derived antifungals. Pau d'Arco is one of the canonical members of this antifungal rotation, typically alongside:
- Caprylic acid — an 8-carbon medium-chain fatty acid from coconut oil that disrupts the Candida cell membrane. Typically 500-1,000 mg with meals.
- Undecylenic acid — an 11-carbon fatty acid from castor oil with documented anti-yeast activity. Typically 100-300 mg with meals.
- Oregano oil — standardized to carvacrol, a phenolic monoterpene with broad-spectrum antifungal activity. Typically 100-200 mg of extract or a few drops of oil emulsified in carrier oil.
- Garlic (allicin-standardized) — allicin and ajoene have anti-Candida activity. See Garlic.
- Berberine — alkaloid from goldenseal, Oregon grape, and barberry with multi-target antifungal action. See Goldenseal.
The rationale for rotation rather than monotherapy is the same as for antibiotic rotation: reduce the selection pressure for resistance. Most integrative protocols cycle these agents on 1-2 week rotations across a 4-12 week total course. Pau d'Arco is typically dosed at 500-1,500 mg of dried-bark equivalent (or 3-9 mL of 1:5 tincture) twice daily, with meals to reduce GI upset and to provide a fat vehicle for the lipophilic naphthoquinones.
This protocol is most appropriate for patients with confirmed intestinal candidal overgrowth (organic acids urine test showing elevated arabinose, stool culture, or comprehensive stool analysis) and for those with recurrent mucocutaneous candidiasis. It is not appropriate as a generic "detox" or "energy boost" intervention — the redox-cycling pharmacology does carry real toxicity at sustained high doses (see the Cautions & Cancer Research page).
Parallel dietary measures — eliminating refined sugar, reducing refined carbohydrate, restoring stomach acid, repopulating with diverse Probiotics, repairing intestinal barrier function with Gut Healing nutrients (zinc-carnosine, L-glutamine, slippery elm) — are essential for durable resolution. Antifungals alone tend to give symptomatic improvement that relapses when the underlying ecological imbalance is not addressed.
Practical Dosing — Bark Decoction, Tincture, Standardized Capsule
Pau d'Arco is available commercially in three principal oral forms, each with its own dosing range and bioavailability profile:
- Loose cut inner bark for decoction — the traditional preparation. Adult dose: 1-2 tablespoons of bark per quart of water, simmered (not just steeped) 15-20 minutes, drunk as 2-4 cups per day. Naphthoquinones extract incompletely in water (they are lipophilic), so this is the lowest-potency form. Best for general tonic use and for those starting Pau d'Arco for the first time. Has a pleasant slightly earthy-bitter flavor.
- Alcohol tincture (1:5 in 40-50% ethanol) — the lipophilic naphthoquinones extract well in alcohol. Adult dose: 3-9 mL twice daily (often expressed as 60-180 drops or 1-3 dropperfuls), diluted in water or juice. Taste is bitter; many people prefer to dilute it in a strong-flavored juice (cranberry, pomegranate) or to add it to a cup of warm decoction.
- Standardized capsule extract — the dose-controllable form. Look for products standardized to a specified naphthoquinone content (typically 3-10% lapachol + beta-lapachone combined, expressed as "naphthoquinones"). Adult dose: 500-1,500 mg of dried-bark equivalent twice daily, with meals. The dose-equivalent calculation requires knowing the standardization — a 500 mg capsule at 3% naphthoquinone delivers ~15 mg of active compound, while a 500 mg capsule at 8% delivers ~40 mg. Reputable products list the percentage.
For acute oral candidiasis or vaginal candidiasis, typical integrative-medicine dosing is at the upper end of these ranges for 2-3 weeks, then tapered to a lower maintenance dose for 4-8 additional weeks. For dermatophyte skin infection, the topical preparations are usually the primary therapy and oral dosing is supportive.
For nail infection (onychomycosis), 6-12 months of combined oral and topical therapy is typical — the nail grows slowly and the entire infected nail plate must grow out before clinical clearance. This is a long commitment; many patients prefer oral terbinafine despite its hepatotoxicity profile because the duration is shorter (12 weeks).
Quality & Standardization — Why Most Commercial Products Are Underpotent
Pau d'Arco is one of the most adulterated herbs on the U.S. market. The botanical taxonomy is confusing: the genus historically called Tabebuia was split in 2007 such that the medicinally important species is now Handroanthus impetiginosus (the "purple lapacho"), while several other Tabebuia and Tecoma species — with little or no naphthoquinone content — are still sold as "pau d'arco" or "lapacho" in commercial trade. Outer-bark material (which contains little naphthoquinone), wood chips, and sapwood substitution are also common.
Quality markers for a serious antifungal product:
- Species specified on the label — "Tabebuia impetiginosa" or "Handroanthus impetiginosus" (the same plant under its old and new names). Avoid products listing only "Pau d'Arco" or "Tabebuia" without species.
- Part specified as "inner bark" — not "bark" alone, not "wood," not "stem." The lapachol and beta-lapachone are concentrated in the inner bark layer (phloem).
- Naphthoquinone percentage stated — reputable products show 3-10% lapachol + beta-lapachone combined. Without a stated percentage, you cannot know the active dose.
- Origin — sustainable harvest from wild South American sources (Argentina, Paraguay, Bolivia) tends to have higher naphthoquinone content than younger cultivated material.
- Third-party testing certificate — ideally USP or NSF certification, or at least a published Certificate of Analysis.
Generic supermarket-grade Pau d'Arco capsules without these markers may contain very little active naphthoquinone — explaining the wide variability of patient reports of efficacy.
Cautions Specific to the Antifungal Use
The cautions specific to antifungal-dose Pau d'Arco are largely the same as the general cautions covered in detail on the Cautions & Cancer Research page, but with a few use-specific points worth emphasizing here:
- "Die-off" reaction (Jarisch-Herxheimer-like syndrome) — the rapid kill of large fungal populations can release endotoxin-like cell-wall fragments that produce a flu-like reaction: malaise, low-grade fever, headache, body ache, brain fog, and worsened original symptoms for 24-72 hours. Mitigate with a lower starting dose, slow uptitration, generous water intake, binders (activated charcoal 500 mg between meals, bentonite clay 1 tsp in water at bedtime), and slow elimination support (milk thistle, dandelion root tea).
- Anticoagulant interaction — beta-lapachone and lapachol are functional vitamin K antagonists. Do not combine with warfarin, heparin, apixaban, rivaroxaban, dabigatran, clopidogrel, ticagrelor, or aspirin without explicit monitoring. Discontinue Pau d'Arco at least 14 days before any planned surgery.
- Pregnancy and breastfeeding — absolute contraindication. Lapachol crosses the placenta and has demonstrated teratogenic and reproductive-toxic effects in rodent studies. Do not use, even topically over large body-surface areas, in pregnancy. Also avoid during breastfeeding — the molecule passes into breast milk.
- G6PD deficiency — the redox-cycling mechanism produces oxidative stress on red blood cells. Patients with glucose-6-phosphate dehydrogenase deficiency are at risk for hemolytic anemia and should not use high oral doses. Common in Mediterranean, African, and Southeast Asian populations.
- GI tolerance — nausea, soft stool, and epigastric burning are the most common side effects. Take with meals. If GI symptoms persist beyond a few days, reduce the dose or switch from capsules to a more dilute tea preparation.
- Hepatic monitoring with sustained high dose — for courses longer than 8 weeks at the upper dose range, periodic liver function testing (ALT, AST, total bilirubin) is reasonable. Stop immediately for any unexplained jaundice, dark urine, or persistent right-upper-quadrant discomfort.
- Drug interaction with chemotherapeutic agents — concurrent use with topoisomerase inhibitor chemotherapy (irinotecan, topotecan, etoposide, doxorubicin) is theoretically problematic because of mechanistic overlap. Patients receiving cancer chemotherapy should discuss any Pau d'Arco use with their oncology team.
Key Research Papers
- Guiraud P, Steiman R, Campos-Takaki GM, Seigle-Murandi F, Simeon de Buochberg M (1994). Comparison of antibacterial and antifungal activities of lapachol and beta-lapachone. Planta Medica. — PubMed
- Portillo A, Vila R, Freixa B, Ferro E, Parella T, Casanova J, Canigueral S (2005). Antifungal activity of Paraguayan plants used in traditional medicine. Journal of Ethnopharmacology. — PubMed
- Macedo L, Fernandes T, Silveira L, Mesquita A, Franchitti AA, Ximenes EA (2013). beta-Lapachone activity in synergy with conventional antimicrobials against methicillin-resistant Staphylococcus aureus and antifungal activity. Phytomedicine. — PubMed
- Pinto AV, de Castro SL (2009). The trypanocidal activity of naphthoquinones: a review. Molecules. — PubMed
- Hussain H, Krohn K, Ahmad VU, Miana GA, Green IR (2007). Lapachol: an overview. ARKIVOC. — PubMed
- Castellanos JR, Prieto JM, Heinrich M (2009). Red Lapacho (Tabebuia impetiginosa) — a global ethnopharmacological commodity? Journal of Ethnopharmacology. — PubMed
- Park BS, Lee HK, Lee SE, Piao XL, Takeoka GR, Wong RY, Ahn YJ, Kim JH (2006). Antibacterial activity of Tabebuia impetiginosa Martius ex DC (Taheebo) against Helicobacter pylori. Journal of Ethnopharmacology. — PubMed
- Salas C, Tapia RA, Ciudad K, Armstrong V, Orellana M, Kemmerling U, Ferreira J, Maya JD, Morello A (2008). Trypanosoma cruzi: activities of lapachol and alpha- and beta-lapachone derivatives. Bioorganic & Medicinal Chemistry. — PubMed
- Steinert J, Khalaf H, Rimpler M (1996). HPLC determination of naphthoquinone derivatives from Tabebuia avellanedae. Journal of Chromatography. — PubMed
- Mantovani MS et al. (2008). beta-Lapachone induced DNA damage in normal and tumor cells. Mutation Research. — PubMed
- Fonseca SG et al. (2003). Studies on Pau d'Arco aqueous extract activity. Brazilian Journal of Medical and Biological Research. — PubMed
- Crook WG (1986). The Yeast Connection and subsequent integrative-medicine Candida diet protocols citing Pau d'Arco. — PubMed
PubMed Topic Searches
- PubMed: Tabebuia impetiginosa Candida antifungal
- PubMed: Lapachol / beta-lapachone vs Candida MIC
- PubMed: Naphthoquinone vs dermatophytes
- PubMed: Handroanthus impetiginosus antimicrobial
- PubMed: Pau d'Arco / lapacho traditional antifungal
Connections
- Pau d'Arco Overview
- Pau d'Arco Benefits Hub
- Pau d'Arco — Immune Modulation
- Pau d'Arco — Anti-Inflammatory
- Pau d'Arco — Cautions & Cancer Research
- Fungal Infections
- Mold & Mycotoxins
- Oregano (Carvacrol)
- Goldenseal (Berberine)
- Neem
- Garlic (Allicin)
- Probiotics
- Gut Healing
- Elimination Diet
- Olive Leaf