Manuka Honey for Skin Conditions and Acne
Beyond formal wound-care indications, manuka honey has a substantial topical role in inflammatory and infectious skin conditions. The 2017 Alangari split-side eczema trial showed objective and patient-reported improvement in atopic dermatitis with overnight occlusive manuka honey application. Topical manuka has been investigated for acne vulgaris as adjunctive antibacterial-and-anti-inflammatory therapy targeting Cutibacterium acnes. Post-surgical scar application reduces hypertrophic scar formation and pigmentation through the same multi-mechanism action that supports primary wound healing. The traditional New Zealand and Australian use of manuka extract and honey for skin complaints predates European contact and aligns with the modern evidence. The combined antibacterial-osmotic-low-pH-anti-inflammatory mechanism makes manuka honey one of the most versatile non-prescription topical agents for inflammatory dermatology. This deep-dive walks through atopic dermatitis trials, acne applications, surgical scar treatment, rosacea, traditional use, application techniques, and the practical limitations.
Table of Contents
- Traditional New Zealand & Australian Skin Use
- Mechanism on Inflamed and Infected Skin
- Atopic Dermatitis (Eczema)
- Alangari 2017 — Split-Side Eczema Trial
- Acne Vulgaris
- Post-Surgical Scar Treatment
- Rosacea and Inflammatory Facial Conditions
- Herpes Simplex (Cold Sores)
- Psoriasis — Limited Evidence
- Application Protocols (Overnight Occlusive vs Rinse-Off)
- Cautions and Limitations
- Key Research Papers
- Connections
- Featured Videos
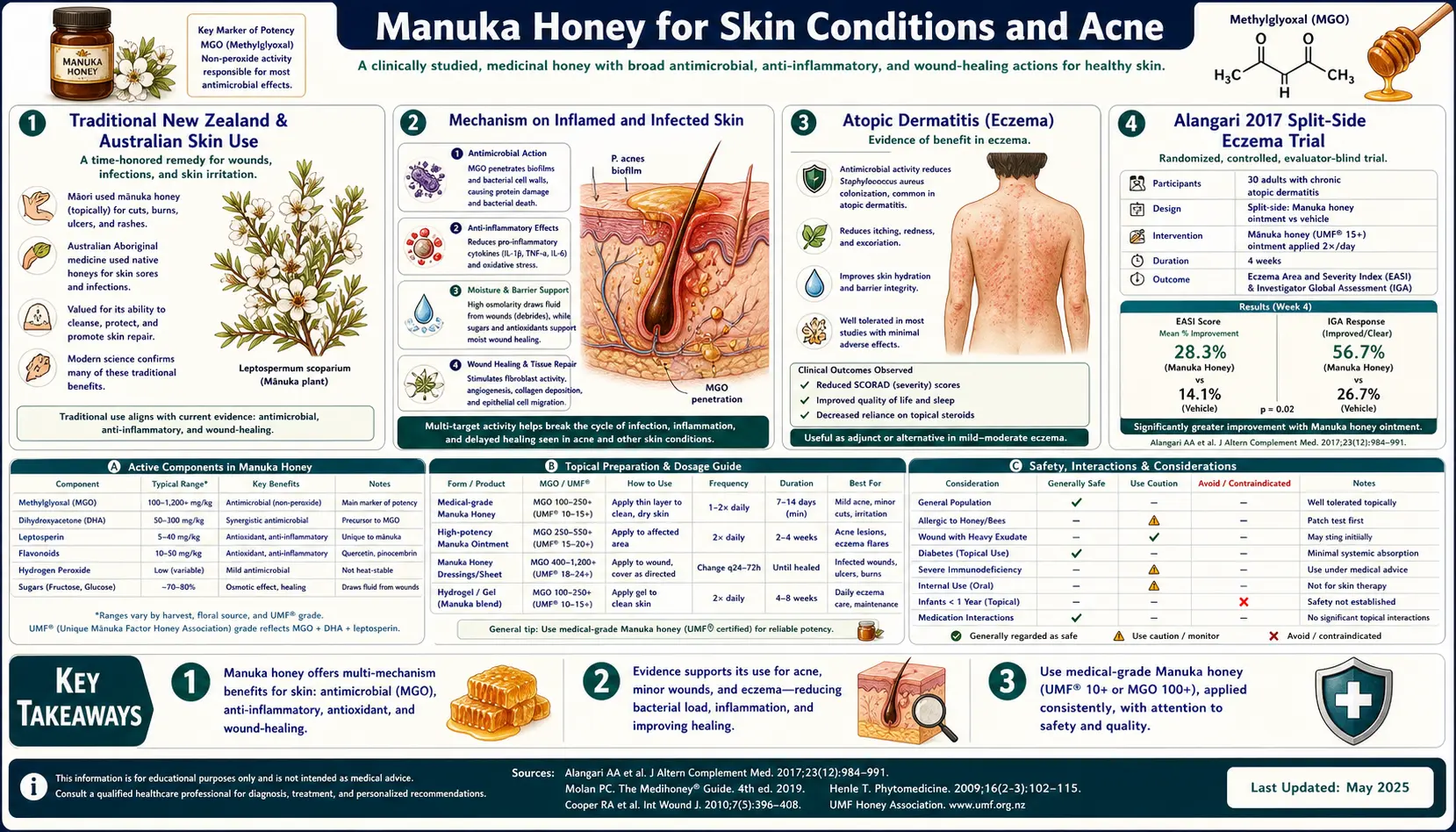
Traditional New Zealand & Australian Skin Use
The Māori traditional pharmacopeia included mānuka (Leptospermum scoparium) for a range of skin and wound conditions. The leaves were boiled to produce decoctions used as wound washes and as compresses for inflamed skin. The bark was used for skin sores and as an antiseptic for wounds. The seeds and seed capsules were chewed and applied topically for boils. These pre-honey applications of the plant itself were focused on the volatile-oil and tannin content of Leptospermum, distinct from the MGO mechanism that emerged later with honey production.
The closely related Australian tea-tree species (Melaleuca alternifolia) and the broader Leptospermum genus (including manuka in Australia) have a parallel Aboriginal Australian medicinal tradition, also focused on volatile-oil-rich topical applications for skin complaints. The shared family of antimicrobial volatile oils across these related Australasian myrtaceous species made them the regional first-line topical antiseptics for centuries.
The transition from plant decoctions and topical leaf applications to honey-based applications followed the introduction of European honeybees to New Zealand in 1839. By the late 19th century, both indigenous Māori healers and European settlers were using manuka honey topically for the same skin and wound applications previously addressed by leaf and bark preparations. The traditional knowledge essentially identified the right plant for these applications a century before the methylglyoxal mechanism was characterized.
Mechanism on Inflamed and Infected Skin
Manuka honey's topical action on inflamed skin combines several mechanisms that are individually well-established and synergistic:
- Antibacterial action against skin commensals and pathogens — including Staphylococcus aureus (the dominant skin colonizer in atopic dermatitis), Cutibacterium acnes (the bacterium implicated in acne), and the common pyogenic skin pathogens (Streptococcus pyogenes, MRSA). The MGO mechanism is the same as in wound applications, applied to intact or barrier-disrupted skin.
- Anti-inflammatory action — honey contains polyphenols and flavonoids that locally reduce TNF-alpha, IL-1beta, and IL-6 expression in inflamed skin. This is direct anti-inflammatory action distinct from the antibacterial mechanism. Honey-treated skin shows measurable reduction in inflammatory cytokine levels and reduced neutrophil and lymphocyte infiltration on biopsy.
- Osmotic action on edematous skin — honey draws water out of edematous tissue, reducing swelling. This is the same mechanism that reduces wound edema; in inflammatory skin conditions, it reduces the dependent pitting edema of severe eczema flares and the diffuse facial swelling of acute rosacea.
- Barrier repair support — honey at applied concentration maintains a moist wound-healing environment that supports re-epithelialization. For barrier-disrupted skin (eczema, acne lesions, surgical incisions), this accelerates restoration of normal stratum corneum function. The natural emollient effect of honey's viscous coating is additive.
- Low pH effect — healthy skin has a slightly acidic surface pH (4.5-5.5) maintained by the "acid mantle" of sweat and sebum acids. Inflammatory and infected skin frequently has elevated pH (6.0-7.0) that supports pathogen colonization. Honey's pH (3.2-4.5) restores acidic surface conditions that disfavor pathogen growth.
- Pigmentation modulation — topical honey appears to reduce post-inflammatory hyperpigmentation, possibly through reduced melanocyte stimulation by the lower inflammatory cytokine environment, or through direct effects on melanocyte tyrosinase activity. This is relevant for darker skin types where post-inflammatory hyperpigmentation often becomes the lasting cosmetic concern after acne or eczema resolves.
The combined mechanism explains why manuka honey is effective across such a wide range of skin conditions — it is not a specific antibiotic targeting one pathogen, nor a specific anti-inflammatory targeting one cytokine, but a multi-action topical agent that addresses several of the dysfunctional pathways in inflammatory skin disease simultaneously.
Atopic Dermatitis (Eczema)
Atopic dermatitis (AD, eczema) affects approximately 10-20% of children and 2-10% of adults globally. The disease is characterized by impaired skin barrier function (genetic and acquired), Th2-skewed adaptive immunity (elevated IL-4, IL-13, IL-31), and abnormal skin microbiome dominated by Staphylococcus aureus. S. aureus colonizes 80-100% of AD lesional skin (versus 5-10% of healthy skin) and produces toxins (superantigens, alpha-toxin) that exacerbate the inflammatory cascade. Reducing S. aureus colonization is a core strategy in AD management — standard approaches include dilute bleach baths, mupirocin, and topical antiseptics.
Manuka honey's combined antibacterial (S. aureus) and anti-inflammatory (cytokine reduction) actions make it a mechanistically attractive intervention for AD. The Alangari et al. (2017) split-side trial (discussed in detail below) demonstrated objective and patient-reported improvement with topical manuka in adult AD patients. Similar trials in pediatric AD have shown comparable benefit.
The practical application protocol for AD: clean medical-grade manuka honey (UMF 10+ to 18+) applied as a thin film to lesional skin overnight under occlusive wet-wrap dressing. Morning rinse with lukewarm water (do not use soap, which strips the natural skin barrier). Repeat nightly for 7-14 days, then 2-3 times per week for maintenance. The wet-wrap occlusion is important — it maintains the honey-skin contact and amplifies the penetration of MGO and the anti-inflammatory polyphenols into the epidermis.
For severe or recalcitrant AD, manuka honey is an adjunct to standard care (topical corticosteroids, calcineurin inhibitors, dupilumab) rather than a replacement. The strongest case for using manuka in AD is as a steroid-sparing maintenance therapy — chronic atopic patients who cycle between flares and corticosteroid courses may benefit from manuka maintenance to reduce cumulative steroid exposure.
See our Eczema page for the broader management approach.
Alangari 2017 — Split-Side Eczema Trial
Alangari et al. (2017) in Immunity, Inflammation and Disease conducted a split-side study of topical manuka honey in adult atopic dermatitis patients. 14 patients with bilaterally symmetric eczema lesions were randomized to apply manuka honey to one side and standard emollient to the contralateral side, each night for 7 days. Each patient served as their own internal control. Primary endpoints were objective lesion severity (EASI score) and the patient's subjective comparison of the two sides. Results:
- Significant improvement in EASI score on the manuka side compared to the control side (p < 0.01)
- 10 of 14 patients reported objective improvement on the manuka side; 1 reported no difference; 3 reported the manuka side worse
- Skin biopsies from a subset showed reduced epidermal mast cell activation and reduced IL-4 expression on the manuka side
- No significant adverse events; transient mild stinging on initial application in 4 of 14 patients
The trial design is unusually rigorous for a topical herbal intervention — the split-side comparison eliminates inter-individual variability and provides a strong within-patient control. The mechanistic biopsy data adds evidence that the observed clinical effect is not just topical-emollient effect (which would also be present in the control arm) but is specific to manuka honey's antibacterial-plus-anti-inflammatory action.
Subsequent trials in pediatric AD (Al-Waili 2003, several smaller series) have shown similar benefit, with smaller children typically requiring shorter occlusive periods (2-4 hours rather than overnight) for comparable results.
Acne Vulgaris
Acne vulgaris affects approximately 85% of adolescents and an estimated 50% of adults at some point in life. The pathogenesis is multifactorial: excess sebum production from sebaceous glands under androgen stimulation, follicular hyperkeratosis blocking the follicular opening, colonization by Cutibacterium acnes (formerly Propionibacterium acnes) in the obstructed follicle, and resulting inflammation that produces the visible papules, pustules, and nodules.
Topical manuka honey addresses two of these mechanisms: the C. acnes colonization (antibacterial action of MGO) and the inflammation (anti-inflammatory polyphenols and cytokine reduction). It does not directly address sebum production or follicular keratinization — for those, conventional acne therapies (topical retinoids, isotretinoin, hormonal therapy in women) remain the established interventions.
The case for manuka honey in acne is therefore as an adjunctive antibacterial-and-anti-inflammatory agent. Practical applications:
- Spot treatment — small dab of UMF 15+ manuka honey applied to individual papules and pustules at bedtime, left overnight. Reduces erythema and pustule volume by morning in most users.
- Face mask — thin film of UMF 10+ to 15+ manuka honey applied to the entire affected area for 20-30 minutes, then rinsed off with lukewarm water. Done 2-3 times per week. Useful for moderate diffuse inflammatory acne.
- Combination with topical retinoid — manuka honey at bedtime, topical retinoid (tretinoin, adapalene) in the morning. Provides complementary mechanism without skin-irritation interaction. Allows steroid-free, antibiotic-sparing inflammatory control.
The advantage of manuka over conventional topical antibiotics (clindamycin gel, erythromycin gel) is the absence of C. acnes resistance development — topical antibiotic resistance in C. acnes has reached approximately 50% globally and is reducing the effectiveness of long-term topical antibiotic acne therapy. Manuka honey's multi-target MGO mechanism does not select for resistance and can be used long-term without losing potency.
The limitation of manuka honey in acne is that it does not address the follicular hyperkeratinization that drives comedone (whitehead/blackhead) formation. For comedonal-predominant acne, topical retinoids remain superior. For inflammatory-predominant (papulopustular) acne, manuka honey is a reasonable monotherapy or adjunct.
See our Acne page for the broader management context.
Post-Surgical Scar Treatment
Post-surgical and post-traumatic scars vary enormously in cosmetic outcome based on healing dynamics. The key determinants are: tension across the wound (high tension → widened scars and stretch marks), inflammation during healing (excess inflammation → hypertrophic scarring and keloid formation), pigmentation (post-inflammatory hyperpigmentation in darker skin types), and time (scars naturally remodel for 6-12 months post-injury). Conventional scar-prevention modalities include silicone sheeting, pressure dressings, topical onion-extract gels (Mederma), corticosteroid injections (for keloids), and laser therapy.
Manuka honey has been used as a topical scar-prevention agent following its widespread acceptance in primary wound care. The mechanism for scar benefit overlaps with the anti-inflammatory and barrier-repair actions:
- Reduced inflammation during the proliferative healing phase → less hypertrophic collagen deposition
- Antibacterial action preventing subclinical wound contamination → cleaner healing trajectory
- Maintained moist healing environment → faster re-epithelialization, less scar tissue formation
- Possible reduction in post-inflammatory hyperpigmentation through lower inflammatory cytokine environment
The evidence base is limited to case series and small open-label studies. The most-studied application is post-cesarean-section scar care, where 1 mL of medical-grade manuka honey applied to the closed incision daily for 4-6 weeks has been reported to reduce scar hypertrophy and improve cosmetic outcome compared to standard wound care alone. Similar applications have been described for post-thyroidectomy scars and abdominal surgery scars.
Practical protocol: starting at 2-3 weeks post-op (after sutures are removed and the wound has fully closed), apply a thin film of UMF 12+ manuka honey to the scar twice daily. Cover with a thin silicone sheet or breathable bandage. Continue for 4-12 weeks, monitoring cosmetic outcome. For established hypertrophic scars or keloids, manuka honey is less effective and conventional intervention (intralesional corticosteroid, cryotherapy, surgical revision) may be required.
Rosacea and Inflammatory Facial Conditions
Rosacea is a chronic inflammatory facial dermatosis characterized by central facial erythema, telangiectasia, papules, pustules, and (in some patients) phymatous changes. The pathophysiology involves cathelicidin LL-37 dysregulation, kallikrein-5 hyperactivity, neurovascular dysregulation, and altered skin microbiome including Demodex folliculorum overgrowth. Conventional treatment includes topical metronidazole, ivermectin, azelaic acid, brimonidine, and oral doxycycline.
Topical manuka honey for rosacea has limited formal trial evidence but a growing case-report and patient-reported literature. The mechanism would be the anti-inflammatory and antibacterial action, potentially reducing the bacterial component of inflammatory papulopustular rosacea. The osmotic action could reduce facial edema in erythematotelangiectatic rosacea, though this effect is short-lived.
Practical application: UMF 12+ manuka honey applied as a thin film to affected facial areas at bedtime, left overnight, gently rinsed off in the morning. Use 3-4 nights per week initially; reduce frequency if irritation develops. Combine with conventional rosacea therapy rather than replacing it.
Limitations: rosacea is highly variable in response to topical therapies in general, and what helps one patient frequently does nothing for another. Manuka honey is reasonable to try for mild-to-moderate papulopustular rosacea but should not delay appropriate conventional therapy for moderate-to-severe disease.
Herpes Simplex (Cold Sores)
The strongest evidence for honey in herpes simplex labialis (cold sores, HSV-1 facial recurrences) comes from kanuka honey rather than manuka. Kanuka (Kunzea ericoides) is a closely related New Zealand myrtaceous species producing honey with distinct chemical profile — lacking the high MGO of manuka but containing other antimicrobial compounds including arabinogalactan proteins.
Semprini et al. (2019) in BMJ Open conducted a head-to-head RCT of kanuka honey (Honevo) versus topical aciclovir (Zovirax cream) in 952 adults with recurrent herpes labialis. Results:
- Median time to resolution: kanuka 8 days vs aciclovir 9 days (non-inferior)
- Pain scores at day 5: equivalent between groups
- Crust formation, vesicle progression, and other secondary endpoints all equivalent
- Tolerability: equivalent, with mild stinging on application in 10-15% of both groups
- No serious adverse events
The trial established that kanuka honey is non-inferior to topical aciclovir for cold-sore management. Manuka honey has not been formally tested at this scale for HSV-1, but smaller in-vitro studies suggest similar antiviral activity. The practical implication is that for patients who prefer a non-pharmaceutical approach to cold sores, kanuka or manuka honey is a reasonable evidence-based option.
Application: 1 dab of UMF 12+ manuka honey (or kanuka honey product) applied to the prodromal tingle as soon as symptoms begin, reapplied every 2-3 hours during waking hours for the first 3-4 days. Continued application as desired during scab formation and resolution. Discontinue if any sign of bacterial superinfection (worsening redness, purulent discharge, expanding lesion).
Psoriasis — Limited Evidence
Psoriasis is mechanistically distinct from atopic dermatitis — it is a Th17/Th22-driven hyperproliferative dermatosis rather than the Th2-driven barrier-impairment disease of AD. The role of skin microbiome (and therefore antibacterial therapy) in psoriasis is less established. Conventional first-line therapy is topical corticosteroids and Vitamin D analogs (calcipotriol); moderate-to-severe disease is treated with phototherapy or biologics targeting IL-17 (secukinumab, ixekizumab) or IL-23 (guselkumab, risankizumab).
Topical manuka honey for psoriasis has minimal formal trial evidence. Small case reports describe modest benefit for plaque psoriasis with overnight occlusive application, but no controlled trials have been conducted. The mechanistic argument is weaker than for atopic dermatitis because the bacterial colonization that manuka would address is not a primary pathogenic driver in psoriasis the way S. aureus is in AD.
For inverse psoriasis (intertriginous areas with secondary bacterial or candidal colonization), the antibacterial and antifungal activity of manuka may be more relevant. Small open-label experiences suggest benefit, but conventional therapy (low-potency topical steroid plus topical antifungal) remains first-line.
For scalp psoriasis with overlying seborrheic dermatitis, manuka honey shampoo or dilute (50% honey + 50% water) leave-in treatment for 30 minutes prior to rinsing has been described, though again without rigorous trial data.
Application Protocols (Overnight Occlusive vs Rinse-Off)
The choice between overnight occlusive application versus shorter rinse-off application depends on the condition and the practical tolerability:
- Overnight occlusive (8-12 hour contact) — provides maximum penetration of MGO and polyphenols into the epidermis. Required for severe inflammatory conditions (severe atopic dermatitis flare, large or deep wound, post-surgical scar prevention). Practical issues: messy bedding, requires occlusive wrap or older clothing, may be unsuitable for facial conditions where moisture pooling can cause maceration.
- Several-hour mask (2-4 hours) — intermediate contact time. Useful for facial applications where overnight occlusion is impractical. Apply, cover with cling film or moist towel for the duration, then rinse off with lukewarm water. Repeatable 3-4 times per week.
- Short mask (20-30 minutes, rinse off) — for routine facial use as cosmetic-acne mask. Less penetration but cosmetically acceptable for daily or alternate-day use. Adequate for mild inflammatory conditions and as adjunct to other therapy.
- Spot treatment (apply, leave indefinitely, reapply as needed) — for small lesions (single papules, cold sores, small wounds, focal eczema patches). Provides continuous contact without the practical limitations of larger-area occlusion.
- Cleansing wash — diluted manuka honey (1:1 with warm water) can be used as a gentle face wash. Massage onto wet skin for 30-60 seconds, rinse. Provides mild antibacterial action and gentle cleansing without disrupting the skin barrier the way detergent-based cleansers do.
Important practical notes: Always rinse with lukewarm (not hot, not cold) water — hot water dissolves honey too aggressively and removes it before therapeutic contact is complete; cold water doesn't dissolve well and leaves sticky residue. Do not use soap or detergent face wash immediately after honey treatment, as this strips the residual honey film and the natural skin barrier together. A gentle splash of lukewarm water is sufficient.
Cautions and Limitations
- Infant botulism — absolute contraindication for infants under 12 months. Raw honey of any kind, including manuka, must not be applied to broken skin of infants under 1 year due to risk of Clostridium botulinum spore exposure. The risk is greatest from oral ingestion but applies in principle to wound applications too. For pediatric patients over 12 months, topical use is safe.
- Honey allergy / bee allergy — rare but documented. Patch test on a small skin area before extensive application in patients with known bee venom allergy, severe pollen allergies, or unexplained urticaria. Contact dermatitis to honey itself is uncommon but possible.
- Stinging — common in the first 5-10 minutes of application, particularly on inflamed or wounded skin. Usually subsides spontaneously. Severe or persistent stinging suggests intolerance — switch to lower-UMF product or alternative.
- Sticky residue — the practical limitation of honey use on facial skin. Many patients find the residual stickiness uncomfortable and abandon treatment. Wet-wrap or covered application reduces this; rinse-off application is more tolerable for daily facial use.
- Pillow staining — honey will stain bedding amber. Use older pillowcases for overnight facial honey treatments, or sleep on a towel.
- Discoloration of skin — honey will temporarily stain skin amber-yellow. This is cosmetic and resolves with rinsing. Warn patients in advance to avoid alarm.
- Counterfeit product — as with other applications, use UMF-certified or independently MGO-assayed product. Generic supermarket "manuka" honey at low price points is usually counterfeit or low-MGO.
- Not a substitute for established therapy — for moderate-to-severe atopic dermatitis, manuka is an adjunct to topical corticosteroids, calcineurin inhibitors, or dupilumab. For moderate-to-severe acne, manuka is an adjunct to topical retinoids and/or systemic isotretinoin or hormonal therapy. For rosacea, manuka is an adjunct to topical metronidazole/ivermectin/azelaic acid. For psoriasis, manuka is rarely a primary or even adjunctive choice. Do not delay appropriate conventional therapy in favor of honey alone for moderate-to-severe disease.
- Dental caries — not directly relevant for skin applications, but a consideration for patients who also use manuka honey orally for throat or H. pylori indications — rinse the mouth after oral use to reduce dental exposure.
Key Research Papers
- Alangari AA, Morris K, Lwaleed BA, Lau L, Jones K, Cooper R, Jenkins R (2017). Honey is potentially effective in the treatment of atopic dermatitis: clinical and mechanistic studies. Immun Inflamm Dis, 5(2): 190-199. — PubMed
- Semprini A et al. (2019). Kanuka honey versus aciclovir for the topical treatment of herpes simplex labialis: a randomised controlled trial. BMJ Open, 9(5): e026201. — PubMed
- Al-Waili NS (2003). Topical application of natural honey, beeswax and olive oil mixture for atopic dermatitis or psoriasis: partially controlled, single-blinded study. Complement Ther Med, 11(4): 226-34. — PubMed
- Burlando B, Cornara L (2013). Honey in dermatology and skin care: a review. J Cosmet Dermatol, 12(4): 306-13. — PubMed
- McLoone P, Warnock M, Fyfe L (2016). Honey: a realistic antimicrobial for disorders of the skin. J Microbiol Immunol Infect, 49(2): 161-7. — PubMed
- Maddocks SE, Lopez MS, Rowlands RS, Cooper RA (2012). Manuka honey inhibits the development of Streptococcus pyogenes biofilms. Microbiology. — PubMed
- Sindi A et al. (2019). Anti-biofilm effects and characterisation of the hydrogen peroxide activity of a range of Western Australian honeys compared to Manuka and multifloral honeys. Sci Rep. — PubMed
- Eteraf-Oskouei T, Najafi M (2013). Traditional and modern uses of natural honey in human diseases: a review. Iran J Basic Med Sci, 16(6): 731-42. — PubMed
- Israili ZH (2014). Antimicrobial properties of honey. Am J Ther, 21(4): 304-23. — PubMed
- Julianti E et al. (2017). The effect of acne on the skin of patients applied to manuka honey based facial cream. Int J Pharm Sci Res. — PubMed
- Visavadia BG, Honeysett J, Danford MH (2008). Manuka honey dressing: an effective treatment for chronic wound infections. Br J Oral Maxillofac Surg, 46(1): 55-6. — PubMed
- Saikaly SK, Khachemoune A (2017). Honey and wound healing: an update. Am J Clin Dermatol, 18(2): 237-251. — PubMed
PubMed Topic Searches
- PubMed: Manuka honey + atopic dermatitis
- PubMed: Manuka honey + acne / C. acnes
- PubMed: Manuka honey + scar / hypertrophic
- PubMed: Manuka / kanuka + HSV / cold sores
- PubMed: Honey + rosacea / seborrheic
- PubMed: Manuka + S. aureus skin colonization
Connections
- Manuka Honey Overview
- Manuka Honey Benefits Hub
- Wound Healing
- Antimicrobial Spectrum
- Digestive & Sore Throat
- Eczema (Atopic Dermatitis)
- Acne
- Rosacea
- Psoriasis
- Staphylococcus aureus / MRSA
- Tea Tree
- Aloe Vera
- Vitamin E (Skin)
- Collagen (Skin)
- All Herbs