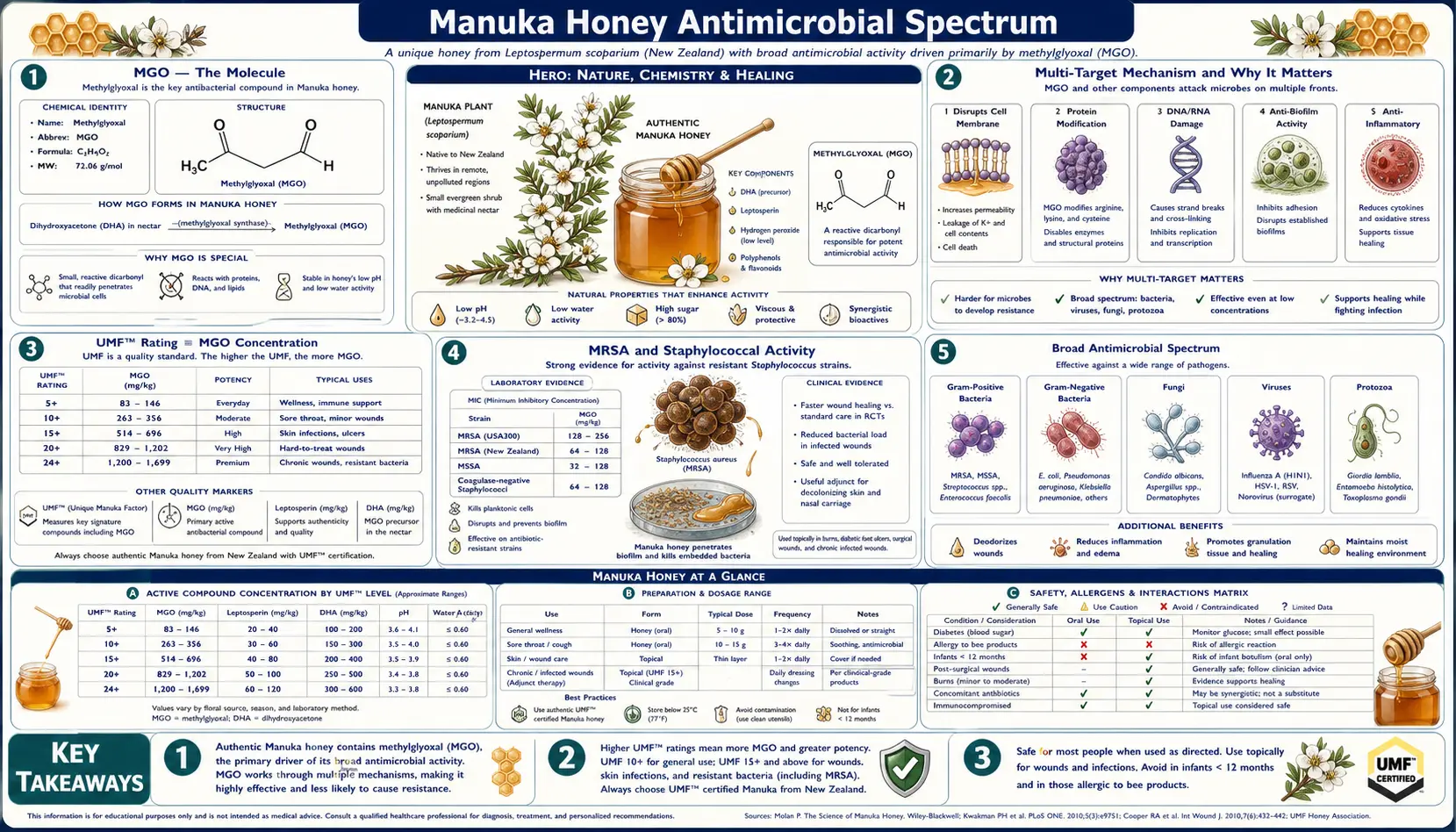
Manuka Honey Antimicrobial Spectrum
Methylglyoxal (MGO) is the single most unusual fact about manuka honey: a small, stable, multi-target antibacterial molecule that has resisted every attempt to find selectable resistance after more than 15 years of clinical wound use. The UMF rating system used commercially is essentially a bioassay readout of MGO concentration. Documented in vitro activity spans MRSA (methicillin-resistant Staphylococcus aureus), VRE (vancomycin-resistant enterococci), Pseudomonas aeruginosa (including biofilm-embedded), Helicobacter pylori, Escherichia coli, Klebsiella pneumoniae, and many anaerobic wound organisms. This deep-dive walks through the MGO mechanism in molecular detail, the spectrum data across organism classes, the biofilm-disruption literature, the remarkable absence of resistance development, and the practical implications for an era of accelerating antimicrobial resistance.
Table of Contents
- MGO — The Molecule
- Multi-Target Mechanism and Why It Matters
- UMF Rating ≡ MGO Concentration
- MRSA and Staphylococcal Activity
- Pseudomonas aeruginosa and Biofilm Disruption
- VRE and Enterococcal Activity
- Helicobacter pylori (Gastric)
- Gram-Negative Rods (E. coli, Klebsiella, Acinetobacter)
- Anaerobes and Fungi
- The Absence of Resistance Development
- Cautions and Limitations
- Key Research Papers
- Connections
- Featured Videos
MGO — The Molecule
Methylglyoxal (CH3-CO-CHO, molecular weight 72.06 g/mol) is a small alpha-oxoaldehyde — structurally, an aldehyde adjacent to a ketone with a methyl group. It is one of the most reactive carbonyl compounds in biology, capable of crosslinking proteins, nucleic acids, and lipids on contact through formation of covalent adducts at multiple chemical sites. MGO is endogenously generated in all cells as a side-product of glycolysis (from triose-phosphate intermediates) and is detoxified primarily by the glyoxalase enzyme system (glyoxalase I + II), which converts it to D-lactate using glutathione as a cofactor. Bacterial cells have less effective glyoxalase systems than mammalian cells — this is the therapeutic-index gap that allows manuka honey to kill bacteria at MGO concentrations that human tissue can tolerate.
In manuka honey, MGO is generated non-enzymatically over weeks to months from dihydroxyacetone (DHA) present at high concentration in fresh Leptospermum scoparium nectar. The conversion DHA → MGO proceeds slowly at honey storage temperatures (20-30°C) and is accelerated by elevated storage temperature, lower pH, and longer storage time. Fresh manuka honey may have low MGO and high DHA; the same honey after 18-24 months of storage will have MGO peaking and DHA depleting. Commercial producers manage this maturation actively, often warm-curing the honey under controlled conditions to drive DHA-to-MGO conversion to the target UMF level.
The DHA precursor is unique to Leptospermum-genus nectar — it is not produced in detectable quantities by any of the conventional honey-source plants (clover, citrus, acacia, eucalyptus, etc.). This is why no amount of storage or processing can convert conventional honey into MGO-rich honey: there is no DHA substrate to start from.
The very high MGO concentrations in mature medical-grade manuka (263 to over 1,200 mg/kg) translate to a 30-fold or more concentration advantage over the MGO produced endogenously by host cells. In wound tissue, this MGO gradient produces a strong antibacterial effect at the wound interface while host glyoxalase systems handle the diffused MGO that crosses into deeper tissue.
Multi-Target Mechanism and Why It Matters
The reason MGO has resisted resistance development is that it attacks bacterial cells at multiple essential targets simultaneously — not one specific enzyme that can be mutated, but a diffuse chemical attack on the building blocks of life. Modern antibiotic resistance generally develops when a single point mutation in one target (e.g. ribosome, gyrase, beta-lactamase substrate) lets the bacterium evade the drug. MGO can be evaded only by a bacterium that simultaneously evolves resistance at all of its target classes — statistically improbable.
The multi-target attack includes:
- Arginine modification — MGO reacts with the guanidino group of arginine residues to form irreversible adducts (MG-H1, MG-H2, MG-H3 hydroimidazolones, and CMA carboxymethylarginine). Many essential bacterial enzymes have active-site arginine, and modification disables them. The ribosome itself has multiple critical arginine residues.
- Lysine modification — MGO reacts with epsilon-amino groups of lysine to form CEL (carboxyethyllysine) and MOLD (methylglyoxal lysine dimer crosslinks). Lysine modification disrupts protein-protein interactions and structural proteins.
- Cysteine modification — MGO reacts with thiol groups of cysteine and inactivates enzymes with active-site cysteine (e.g. thioredoxin reductase, glyceraldehyde-3-phosphate dehydrogenase).
- DNA base modification — MGO reacts with guanine to form CEdG (N2-(1-carboxyethyl)-2'-deoxyguanosine), a mutagenic and lethal adduct. Bacterial DNA repair systems cannot keep up at high MGO concentrations.
- Membrane phospholipid amine modification — MGO reacts with the amine head groups of phosphatidylethanolamine and phosphatidylserine, disrupting membrane integrity and ion gradients.
- Cell division inhibition — FtsZ, the bacterial tubulin homolog required for cell division, is inactivated by MGO. MGO-exposed bacteria fail to divide and form elongated filamentous cells, visible by light microscopy.
To resist MGO, a bacterium would need to simultaneously protect arginine, lysine, cysteine, DNA, membrane lipids, and FtsZ — each independently essential. Mathematically, the probability of selecting a single mutant with simultaneous resistance to all targets approaches zero. This is fundamentally why MGO has not produced resistance after years of clinical use, while every conventional antibiotic class (penicillins, cephalosporins, fluoroquinolones, vancomycin, even daptomycin) has produced resistant strains within years of clinical introduction.
UMF Rating ≡ MGO Concentration
The UMF (Unique Manuka Factor) trademark grading system used commercially is essentially a bioassay readout of the non-peroxide antibacterial activity, which in turn is essentially a readout of MGO concentration. Mathematically:
- UMF = MGO ≈ 5 → 83 mg/kg
- UMF = MGO ≈ 10 → 263 mg/kg
- UMF = MGO ≈ 15 → 514 mg/kg
- UMF = MGO ≈ 18 → 696 mg/kg
- UMF = MGO ≈ 20 → 829 mg/kg
- UMF = MGO ≈ 24 → 1122 mg/kg
- UMF = MGO ≈ 26 → 1282 mg/kg
UMF 10+ / MGO 263 is the medical-grade threshold — the concentration above which manuka honey reliably produces antibacterial activity in standard wound-bed conditions. For most clinical wound applications, UMF 12+ to UMF 18+ is the practical range. For routine consumer health use (cough, throat soothing, gut support), UMF 10+ is sufficient. UMF 5+ is essentially culinary-grade with minimal therapeutic activity.
Bioavailability matters. The UMF/MGO scale measures total MGO in the honey, but in vivo activity depends on contact time, exudate dilution, and host glyoxalase activity. Two honeys with identical MGO can produce different in-vivo bacterial kill rates depending on the matrix and the application.
MRSA and Staphylococcal Activity
MRSA (methicillin-resistant Staphylococcus aureus) is the proximate cause of approximately 80,000 invasive infections and 11,000 deaths annually in the United States. Hospital-acquired MRSA (HA-MRSA) and community-acquired MRSA (CA-MRSA, dominated by the USA300 strain) both colonize wound beds preferentially and are among the most-feared organisms in chronic wound care.
Cooper's 2002 paper established manuka honey susceptibility of 18 clinical MRSA isolates from chronic wounds. Minimum inhibitory concentration (MIC) was 1.8-10.8% v/v honey, well below the 30-80% honey concentration achievable in wound dressings. All isolates were killed; none showed reduced susceptibility regardless of their resistance to conventional antibiotics.
Lu et al. (2014) in PeerJ demonstrated that manuka honey eradicates established S. aureus biofilms across multiple strain types with different biofilm-forming capacity. This is clinically significant because biofilm-embedded staphylococci are 100-1000 fold less susceptible to conventional antibiotics than planktonic cells — biofilm is a major reason chronic wound infections persist despite antibiotic therapy. Manuka honey eradicates biofilms through a combination of MGO penetration, osmotic disruption of the biofilm matrix, and direct antibacterial action on the embedded cells.
Henriques et al. (2010) showed that sublethal MGO concentrations cause loss of S. aureus cell-wall integrity and altered surface protein expression — the cells become more susceptible to immune clearance and to subsequent antibiotic challenge. This synergy with both host immunity and conventional antibiotics is the basis for combination protocols where manuka honey dressing is paired with systemic antibiotics for severe wound infections.
For nasal MRSA decolonization — the standard of care is intranasal mupirocin (Bactroban) for 5 days. Some clinicians have used manuka honey nasal application as an alternative or adjunct, particularly when mupirocin resistance is documented (mupirocin resistance in MRSA isolates is increasing). The evidence base is small, but case-series and one randomized trial (Ooi et al. 2008) suggest manuka honey reduces nasal MRSA carriage with similar efficacy to mupirocin, without the resistance-development concern.
See our Staphylococcus aureus / MRSA page for the broader disease context.
Pseudomonas aeruginosa and Biofilm Disruption
Pseudomonas aeruginosa is a gram-negative environmental organism that colonizes chronic wounds, burns, immunocompromised patients (cystic fibrosis lungs, neutropenic cancer patients), and indwelling medical devices. Pseudomonas is intrinsically resistant to many antibiotics, forms tenacious biofilms, and is increasingly multidrug-resistant globally. In wound care, Pseudomonas colonization is associated with greenish exudate, characteristic fruity smell (from 2-aminoacetophenone), and delayed healing.
Roberts et al. (2015) in Microbiology demonstrated that manuka honey is bactericidal against Pseudomonas aeruginosa at MIC of approximately 6% v/v and produces differential expression of oprF (outer membrane porin) and algD (alginate biosynthesis, a major biofilm matrix component). The downregulation of algD effectively prevents biofilm reformation after honey treatment.
Lu et al. (2019) showed that manuka honey eradicates established Pseudomonas biofilms at concentrations achievable in wound dressings, including biofilms grown on silicone catheter material. This is mechanistically explained by the osmotic disruption of the extracellular polymeric substance (EPS) plus direct MGO penetration to the embedded cells. Conventional antibiotics including the gold-standard anti-pseudomonal agents (ciprofloxacin, piperacillin-tazobactam, ceftazidime, meropenem) are 100-1000 fold less effective against the same biofilm preparations.
For cystic fibrosis chronic Pseudomonas lung infection, nebulized or inhaled manuka honey has been investigated in small pilot studies but is not yet established. The CFTR-modulator era (Trikafta, Symdeko) has substantially reduced the urgency of new anti-pseudomonal approaches in CF, but manuka honey remains an interesting investigational option for selected refractory cases.
See our Pseudomonas aeruginosa page for the broader disease context.
VRE and Enterococcal Activity
Vancomycin-resistant enterococci (VRE) — primarily Enterococcus faecium and E. faecalis with acquired vanA or vanB resistance — cause approximately 54,000 healthcare-associated infections annually in the U.S. They are particularly problematic in hospitalized immunocompromised patients (oncology, transplant, ICU) and in surgical wound infections.
Cooper's 2002 paper included VRE among the gram-positive cocci tested; all isolates were susceptible to manuka honey at the same concentrations as vancomycin-susceptible enterococci. The vancomycin-resistance mechanism (substitution of D-Ala-D-Lac for D-Ala-D-Ala in cell-wall precursor) does not confer cross-resistance to MGO because MGO does not act on the cell-wall biosynthesis pathway.
This makes manuka honey an attractive option for VRE-colonized chronic wounds — the local topical activity reduces the burden without requiring systemic linezolid or daptomycin (the conventional VRE-active systemic options, both with significant side-effect profiles).
Helicobacter pylori (Gastric)
Helicobacter pylori is the gram-negative spiral bacterium that colonizes the human gastric mucosa in approximately 50% of the world's population. Chronic H. pylori infection causes peptic ulcer disease and increases the lifetime risk of gastric adenocarcinoma and gastric MALT lymphoma. Standard eradication therapy is "triple therapy" (proton pump inhibitor + clarithromycin + amoxicillin or metronidazole) for 14 days, but global resistance to clarithromycin and metronidazole is rising, and treatment failure rates now exceed 20% in many regions.
Al Somal et al. (1994) in the Journal of the Royal Society of Medicine demonstrated susceptibility of H. pylori to manuka honey at MIC of approximately 5% v/v — concentrations easily achievable by oral honey ingestion. The remarkable finding was that gastric acid does not destroy MGO — the honey's antibacterial activity survives the stomach environment and reaches the gastric mucosa where H. pylori lives.
McGovern et al. and subsequent investigators showed that manuka honey added to standard triple therapy may improve eradication rates by 10-15% in clarithromycin-resistant strains. This is not a primary therapy but an adjunctive approach. The practical protocol is 1 tablespoon (15 g) of UMF 15+ manuka honey on an empty stomach 30 minutes before breakfast and at bedtime, taken alongside standard triple-therapy regimen.
For more on H. pylori management, see the Digestive & Sore Throat deep-dive and the Helicobacter pylori page on this site.
Gram-Negative Rods (E. coli, Klebsiella, Acinetobacter)
Manuka honey is active against most clinically important gram-negative rods at MIC concentrations achievable in wound and gastrointestinal applications:
- Escherichia coli (including extended-spectrum beta-lactamase / ESBL-producing strains) — MIC approximately 5-15% v/v
- Klebsiella pneumoniae (including KPC carbapenemase producers) — MIC approximately 5-10% v/v
- Acinetobacter baumannii (a major hospital-acquired multidrug-resistant pathogen) — MIC approximately 10-25% v/v
- Proteus mirabilis — MIC approximately 5-15% v/v
The resistance mechanisms that defeat conventional antibiotics (ESBL, KPC, AmpC beta-lactamases, porin loss, efflux pumps) do not confer cross-resistance to MGO because MGO does not interact with the beta-lactam binding sites, gyrase, or porin channels. This makes manuka honey an interesting topical option for ESBL-positive surgical wound infections, ESBL-positive chronic ulcers, and Acinetobacter-colonized wounds in returning military personnel and travelers.
Whole-genome sequencing studies of bacteria serially passaged in sub-MIC manuka honey have failed to identify resistance-conferring mutations even after dozens of passages. The bacterial population either remains susceptible or dies; it does not adapt.
Anaerobes and Fungi
Anaerobic bacteria are common colonizers of chronic wounds, particularly diabetic foot ulcers (frequent Bacteroides, Peptostreptococcus, and Prevotella mixed infection) and necrotic wound beds. Manuka honey is active against most clinically relevant anaerobes at MICs in the 5-20% v/v range.
Fungal activity is more variable. Manuka honey shows in vitro activity against Candida albicans and C. glabrata at higher concentrations (MIC typically 30-50% v/v), and there are case reports of topical use for cutaneous candidiasis and oral thrush. Dermatophyte (tinea) activity has been suggested but is not well-established. For systemic or invasive fungal infections, conventional antifungal therapy is the standard; manuka honey is not a primary agent.
Antiviral activity has been demonstrated in vitro against herpes simplex (HSV-1, HSV-2), influenza, and respiratory syncytial virus. The kanuka-honey-versus-aciclovir cold-sore trial (Semprini 2019, BMJ Open) showed kanuka honey was non-inferior to topical aciclovir for herpes labialis healing time. (Kanuka is Kunzea ericoides, a closely related species; its honey shares some antibacterial activity with manuka but does not contain MGO; the active compound in kanuka honey for HSV is not fully characterized but may include arabinogalactan proteins.) See the Skin Conditions deep-dive for more detail.
The Absence of Resistance Development
The defining feature of MGO-based antibacterial activity, contrasted against the global resistance crisis with conventional antibiotics, is the persistent absence of resistance development. Cooper et al. (2010) published the foundational paper on this question in the European Journal of Clinical Microbiology and Infectious Diseases. The study serially passaged MRSA and Pseudomonas aeruginosa in sub-MIC manuka honey for extended periods (28-day continuous passage) and assessed MIC at each passage. Result: no shift in MIC across all passages; the bacterial populations either remained susceptible or were killed.
Subsequent work by multiple independent groups has reproduced this finding across a wider range of organism types and exposure protocols. As of 2026, no naturally-occurring MGO-resistant clinical isolate has been documented despite over 15 years of widespread medical use of Medihoney and other manuka honey wound products. This is in stark contrast to the conventional antibiotic experience — resistance to vancomycin (introduced 1958) became clinically significant in the 1980s, resistance to linezolid (introduced 2000) appeared within years, even daptomycin and ceftaroline (introduced 2003 and 2010) have well-documented resistance.
The mechanistic explanation has three parts:
- Multi-target chemistry — as detailed above, MGO attacks proteins, nucleic acids, membranes, and structural components simultaneously. A single resistance mutation cannot protect against all targets.
- The glyoxalase system is universal — bacteria already have the glyoxalase pathway as their endogenous MGO defense. There is no novel enzyme to evolve; the existing system either has the capacity to detoxify the applied MGO or it doesn't.
- Honey is a mixed-mechanism antimicrobial — the osmotic pressure, low pH, residual hydrogen peroxide, and bee defensin-1 add additional pressures that a bacterium would need to simultaneously overcome.
This makes manuka honey an unusually valuable tool in the era of antimicrobial resistance. It is essentially the only commercially available antibacterial agent that does not select for resistance in the populations it treats. The implication is that manuka honey can be used aggressively in high-risk wound populations (chronic ulcers, diabetic feet, MRSA-colonized) without the conventional concern about contributing to local resistance evolution.
Cautions and Limitations
- Topical and oral use only — manuka honey is approved for topical application and oral consumption. It is not approved for parenteral (intravenous, intramuscular) administration. The hypertonic, acidic nature of honey would be locally damaging and potentially systemically toxic if injected. Do not inject honey under any circumstances.
- Local irritation — stinging on wound application is common in the first 5-10 minutes, particularly with high-UMF product. Usually subsides spontaneously; if persistent or severe, switch to lower-UMF or alternative agent.
- Not a substitute for systemic antibiotics — manuka honey is a powerful topical antimicrobial but does not address bacteremia or invasive deep-tissue infection. Patients with systemic signs (fever, leukocytosis, tachycardia, hypotension) require systemic antibiotics; manuka may be used as adjunctive topical therapy.
- Counterfeit product — the global manuka market is approximately five times larger than New Zealand actually produces. Counterfeit and adulterated products are widespread. Use only UMF-certified or independently MGO-assayed product from reputable suppliers.
- Infant botulism — raw honey of any kind, including manuka, is contraindicated for children under 12 months due to risk of Clostridium botulinum spore exposure and subsequent toxin production in the immature infant gut. Medical-grade Medihoney is gamma-irradiated and theoretically spore-free, but the practical recommendation is to avoid all honey in infants.
- Diabetes — oral consumption — honey is approximately 80% sugar (mixed fructose and glucose). For diabetic patients consuming manuka honey orally (for sore throat, H. pylori, or general health), the carbohydrate load must be counted against daily intake. Topical use does not affect glucose because cutaneous absorption is negligible.
- Cost — medical-grade manuka is expensive. UMF 18+ retails for approximately $50-$100 per 250g jar; Medihoney medical dressings $30-$60 per dressing. Insurance coverage varies.
Key Research Papers
- Mavric E, Wittmann S, Barth G, Henle T (2008). Identification and quantification of methylglyoxal as the dominant antibacterial constituent of Manuka (Leptospermum scoparium) honeys from New Zealand. Mol Nutr Food Res, 52(4): 483-9. — PubMed
- Adams CJ et al. (2008). Isolation by HPLC and characterisation of the bioactive fraction of New Zealand manuka (Leptospermum scoparium) honey. Carbohydr Res, 343(4): 651-9. — PubMed
- Cooper RA, Molan PC, Harding KG (2002). The sensitivity to honey of Gram-positive cocci of clinical significance isolated from wounds. J Appl Microbiol, 93(5): 857-63. — PubMed
- Cooper RA, Jenkins L, Henriques AF, Duggan RS, Burton NF (2010). Absence of bacterial resistance to medical-grade manuka honey. Eur J Clin Microbiol Infect Dis, 29(10): 1237-41. — PubMed
- Kwakman PHS et al. (2010). How honey kills bacteria. FASEB Journal, 24(7): 2576-82. — PubMed
- Kwakman PHS et al. (2011). Two major medicinal honeys have different mechanisms of bactericidal activity. PLoS One, 6(3): e17709. — PubMed
- Lu J et al. (2014). Manuka-type honeys can eradicate biofilms produced by Staphylococcus aureus strains with different biofilm-forming abilities. PeerJ, 2: e326. — PubMed
- Roberts AEL, Maddocks SE, Cooper RA (2015). Manuka honey is bactericidal against Pseudomonas aeruginosa and results in differential expression of oprF and algD. Microbiology, 158(Pt 12): 3005-13. — PubMed
- Henriques AF, Jenkins RE, Burton NF, Cooper RA (2010). The intracellular effects of manuka honey on Staphylococcus aureus. Eur J Clin Microbiol Infect Dis, 29(1): 45-50. — PubMed
- Al Somal N, Coley KE, Molan PC, Hancock BM (1994). Susceptibility of Helicobacter pylori to the antibacterial activity of manuka honey. J R Soc Med, 87(1): 9-12. — PubMed
- Ooi SK et al. (2008). Manuka honey for the topical treatment of intranasal MRSA carriage: a pilot randomised trial. J Hosp Infect. — PubMed
- Carter DA et al. (2016). Therapeutic manuka honey: no longer so alternative. Front Microbiol, 7: 569. — PubMed
PubMed Topic Searches
- PubMed: Manuka honey vs MRSA
- PubMed: Manuka honey vs Pseudomonas / biofilm
- PubMed: MGO mechanism / resistance
- PubMed: Manuka honey vs VRE
- PubMed: Honey vs H. pylori
- PubMed: Manuka honey vs ESBL gram-negatives
Connections
- Manuka Honey Overview
- Manuka Honey Benefits Hub
- Wound Healing
- Digestive & Sore Throat
- Skin Conditions & Acne
- Staphylococcus aureus / MRSA
- Pseudomonas aeruginosa
- Helicobacter pylori
- Sepsis
- Cellulitis
- Silver Nanoparticles
- Garlic
- Tea Tree
- Oregano
- All Herbs