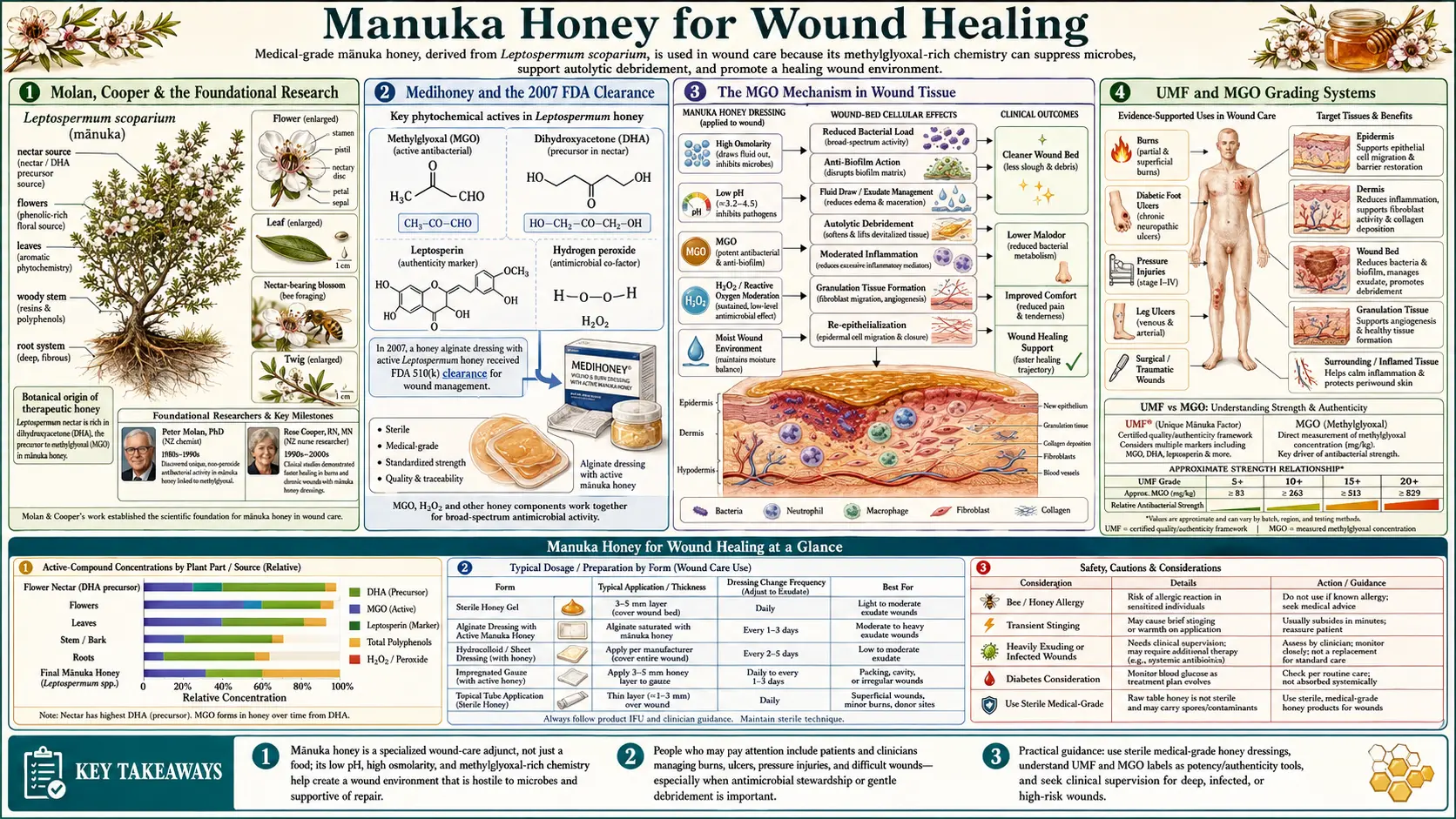
Manuka Honey for Wound Healing
Wound healing is the application that took manuka honey from folk medicine to the FDA Class II medical device register. In 2007, the FDA cleared Medihoney (a gamma-irradiated Leptospermum scoparium honey dressing manufactured by Comvita, distributed by Derma Sciences) for use on diabetic foot ulcers, venous leg ulcers, pressure ulcers, donor sites, and burns — the first traditional wound remedy to clear that regulatory bar in the modern era. The path from Peter Molan's 1980s laboratory work at the University of Waikato in Hamilton, New Zealand, through Rose Cooper's antibacterial characterization at the University of Wales Institute, Cardiff, to randomized clinical trials in venous leg ulcers, diabetic foot ulcers, and partial-thickness burns is one of the few examples in 21st century medicine of a low-tech ancient remedy passing modern evidence-based scrutiny. This deep-dive walks through the mechanism (osmotic + low pH + MGO + residual hydrogen peroxide + bee defensin), the foundational research, the pivotal trials, the UMF and MGO grading systems, and the practical clinical protocols.
Table of Contents
- Molan, Cooper & the Foundational Research
- Medihoney and the 2007 FDA Clearance
- The MGO Mechanism in Wound Tissue
- UMF and MGO Grading Systems
- Venous Leg Ulcer Trials
- Diabetic Foot Ulcer Trials
- Partial-Thickness Burn Trials
- Autolytic Debridement and Exudate Management
- Clinical Application Protocols
- Cautions and Contraindications
- Key Research Papers
- Connections
- Featured Videos
Molan, Cooper & the Foundational Research
The modern scientific case for manuka honey in wound care begins with Peter Molan, a biochemist at the University of Waikato in Hamilton, New Zealand. Molan began systematic study of honey's antibacterial activity in 1981 after seeing patients with chronic wounds treated with locally produced manuka honey at a New Zealand hospital. Over the next two decades, his lab characterized the dual-mechanism nature of honey antibacterial activity — the well-known hydrogen-peroxide pathway present in all nectar honeys, and a second, stable, non-peroxide activity unique to manuka. Molan's 1992 Bee World review — "The antibacterial activity of honey. 1. The nature of the antibacterial activity" — remains a foundational reference.
The chemical identity of the non-peroxide component was unknown until 2008, when two independent groups (Mavric et al. at the Technical University of Dresden, and Adams et al. at the University of Waikato) simultaneously identified methylglyoxal (MGO) as the dominant antibacterial molecule. Mavric's paper in Molecular Nutrition & Food Research quantified MGO concentrations of up to 761 mg/kg in commercial manuka samples, versus less than 5 mg/kg in conventional honeys — a 100-to-1,000-fold concentration difference that fully accounted for the observed antibacterial activity. The MGO is formed non-enzymatically over weeks to months from dihydroxyacetone (DHA), which is present at unusually high concentration only in Leptospermum scoparium nectar.
The clinical microbiology was characterized in parallel by Rose Cooper's group at the University of Wales Institute, Cardiff. Cooper's 2002 paper "The sensitivity to honey of Gram-positive cocci of clinical significance isolated from wounds" established that manuka honey was active against MRSA, vancomycin-resistant enterococci, and a wide range of clinical wound isolates at concentrations achievable in wound dressings. Cooper's subsequent work documented the absence of selectable bacterial resistance even after sustained exposure — a fundamental advantage over conventional topical antibiotics that has been validated in over 15 years of clinical use without emergence of manuka-resistant strains.
Medihoney and the 2007 FDA Clearance
Medihoney is a sterilized, medical-grade Leptospermum scoparium honey product, manufactured by Comvita New Zealand from selected high-UMF manuka and processed by gamma irradiation to eliminate spore-forming bacteria (including Clostridium botulinum) that could contaminate the raw honey. The gamma irradiation does not destroy MGO, which is heat- and radiation-stable. Medihoney is sold as both a viscous gel applied directly to wound beds and as a pre-loaded calcium-alginate or hydrogel dressing.
The U.S. FDA cleared Medihoney as a Class II medical device under 510(k) K062423 in 2007, with subsequent expansions of cleared indications. As of 2026, FDA-cleared uses include:
- Venous leg ulcers (the primary clearance use)
- Diabetic foot ulcers
- Pressure ulcers (decubitus ulcers, all stages)
- Donor sites for skin grafts
- First- and second-degree partial-thickness burns
- Postoperative wounds and traumatic wounds
The clearance was based on the substantial-equivalence pathway (predicate device: hydrogel wound dressings), supported by clinical studies showing non-inferiority for chronic-wound endpoints and superiority for certain antibacterial endpoints. Subsequent NHS approval in the United Kingdom and TGA approval in Australia followed similar pathways. Medihoney is the only honey-based wound product carried on hospital formulary in most U.S. academic medical centers.
Other medical-grade manuka products available globally include Activon (Advancis Medical, UK; used on NHS), L-Mesitran (Theo Manufacturing, Netherlands; a blend of medical-grade honey, vitamins C and E, and zinc oxide for additional antioxidant and re-epithelialization activity), and Surgihoney (Matoke Holdings, UK; an engineered medical honey with controlled hydrogen peroxide release).
The MGO Mechanism in Wound Tissue
Methylglyoxal's antibacterial mechanism is multi-target, which is both why it works against a broad spectrum of organisms and why selectable resistance has not emerged in 15+ years of clinical use. MGO is a small, highly reactive alpha-oxoaldehyde (chemical formula CH3-CO-CHO) that:
- Crosslinks bacterial proteins by reacting with arginine, lysine, and cysteine residues to form irreversible advanced glycation end-products (AGEs). This disables essential enzymes including those required for cell wall biosynthesis, protein synthesis, and DNA replication.
- Modifies bacterial nucleic acids by reacting with guanine and other DNA bases, producing mutagenic and lethal adducts that bacterial DNA repair systems cannot keep up with at high MGO concentrations.
- Disrupts membrane integrity by reacting with phospholipid amine head groups, contributing to membrane leakage and loss of ion gradients.
- Inhibits bacterial cell division by reacting with FtsZ and other cell-division proteins, leading to the formation of elongated non-dividing cells visible by microscopy in MGO-exposed bacterial cultures.
- Disrupts biofilm structure by reacting with extracellular polymeric substance (EPS) components, breaking down established biofilms (a critical clinical advantage because most chronic wound infections are biofilm-based and refractory to systemic antibiotics).
Host tissues are partially protected from MGO toxicity by the glyoxalase system (glyoxalase I and II, requiring glutathione as a cofactor), which converts MGO to D-lactate. Bacteria have less effective glyoxalase systems and are correspondingly more susceptible. This therapeutic-index advantage allows medical-grade manuka honey to kill bacteria at MGO concentrations that human tissue can tolerate.
The osmotic mechanism is additive but distinct. Honey at applied concentration in the wound bed creates a hypertonic environment that draws water out of bacterial cells (loss of turgor, halted growth) and out of edematous host tissue (reduction of wound edema, mechanical debridement of necrotic material). The low pH (3.2-4.5) reduces bacterial growth rates and is hypothesized to improve local tissue oxygenation through the Bohr effect on hemoglobin in the surrounding capillary bed. Residual hydrogen peroxide and bee defensin-1 contribute additional antibacterial activity in the freshly-diluted wound bed.
UMF and MGO Grading Systems
Two parallel grading systems quantify the antibacterial activity of manuka honey. Both must be understood to choose appropriately for clinical or consumer purchase.
UMF (Unique Manuka Factor) is a trademarked grading owned by the UMF Honey Association of New Zealand. The UMF number is determined by an agar-diffusion bioassay against Staphylococcus aureus — a 25% solution of the honey is added to wells in an agar plate, and the diameter of the bacterial growth-inhibition zone is measured and compared to the inhibition zone produced by serial dilutions of phenol. The UMF number is the equivalent concentration of phenol (% w/v) that would produce the same zone. UMF 10+ means the honey has antibacterial activity equivalent to a 10% phenol solution. Only licensed UMF Honey Association members may use the UMF mark on packaging, and audited annually for compliance.
MGO (Methylglyoxal) is a direct chemical assay (by HPLC) of methylglyoxal concentration in mg/kg of honey. It is not trademarked and is used by both UMF licensees and non-licensees. MGO is more reproducible than UMF (chemistry versus bioassay) but loses some information about the contributions of other minor antibacterial compounds and the bioavailability of MGO in different honey matrices.
The two systems correlate tightly:
- UMF 5+ ≈ MGO 83 (food grade, minimal therapeutic activity)
- UMF 10+ ≈ MGO 263 (medical-grade threshold)
- UMF 15+ ≈ MGO 514 (active wound dressing range)
- UMF 18+ ≈ MGO 696
- UMF 20+ ≈ MGO 829
- UMF 24+ ≈ MGO 1122
- UMF 26+ ≈ MGO 1282+ (rare premium product)
For chronic wound clinical use, UMF 12+ to UMF 18+ (MGO 350 to 700) is the typical practical range. Higher MGO does not necessarily produce proportionally better clinical outcomes because the limiting factor is often bioavailability and wound contact time rather than peak MGO concentration. Below UMF 10+ / MGO 263, antibacterial activity is too low for reliable clinical effect against established wound infection. Above UMF 25+ / MGO 1200+, cost rises sharply without proportional clinical benefit for routine wound care, though some practitioners reserve UMF 25+ for refractory chronic wounds.
For consumer purchase: avoid manuka honey sold without either UMF or MGO certification — the global market is plagued by counterfeit and adulterated product (estimated to be more manuka honey sold worldwide annually than is physically produced in New Zealand). Legitimate certified product carries a batch number traceable to the producer.
Venous Leg Ulcer Trials
Venous leg ulcers (VLUs) are chronic wounds caused by venous insufficiency of the lower extremity. They affect approximately 1% of adults over age 65 and are notoriously slow to heal — mean time to closure with standard compression therapy alone is approximately 24 weeks, with 30% recurrence within one year. The chronic, infected, slough-laden character of VLUs makes them a natural test case for an antibacterial, debridement-supporting topical agent.
The pivotal trial was Gethin and Cowman's 2008 multicentre randomized controlled trial published in Journal of Clinical Nursing: 108 patients with sloughy venous or mixed leg ulcers, randomized to manuka honey dressing (Woundcare 18+) versus hydrogel dressing (IntraSite Gel) under standard compression bandaging. Primary outcome was percentage reduction in slough after 4 weeks; secondary outcomes included infection clearance and time to complete closure. Results:
- Median slough reduction: 67% manuka vs 53% hydrogel at 4 weeks (p = 0.054, trend toward manuka superiority)
- Wounds with greater than 50% slough at baseline: significantly faster slough clearance with manuka (p = 0.027)
- Bacterial culture conversion (positive to negative) at 4 weeks: 70% manuka vs 16% hydrogel (p = 0.002, strongly favoring manuka)
- Healing at 12 weeks: 44% manuka vs 33% hydrogel (trend favoring manuka, not significant)
- Patient-reported comfort: equivalent
The Robson et al. 2009 RCT in Journal of Tissue Viability evaluated standardized antibacterial honey (Medihoney) versus standard therapy in a mixed wound population including VLUs and reported 90% bacterial eradication at 4 weeks vs 56% in the standard-care arm.
The 2015 Cochrane systematic review by Jull et al. of 26 RCTs (3,011 patients) of honey for wounds concluded that honey heals partial-thickness burns more quickly than conventional treatment but evidence for VLUs and other chronic wounds was rated low to moderate certainty — the data trend favors honey but most trials were small and methodologically heterogeneous. The clinical practice consensus, despite the Cochrane caution, is that manuka honey is a reasonable choice for sloughy or infected VLUs that have failed to progress on standard moisture-retentive dressings, particularly when MRSA or Pseudomonas colonization is documented.
For more on the broader venous insufficiency picture, see our Venous Insufficiency page and the Cellulitis page for the infection-secondary complication.
Diabetic Foot Ulcer Trials
Diabetic foot ulcers (DFUs) are the leading cause of non-traumatic lower-extremity amputation worldwide. The combination of peripheral neuropathy (loss of protective sensation), peripheral vascular disease (impaired tissue perfusion and oxygen delivery), and immune dysfunction (impaired neutrophil function in chronic hyperglycemia) makes DFUs uniquely refractory to conventional wound care. Approximately 20-25% of all DFUs progress to amputation within 5 years, and 5-year mortality after a major DFU-related amputation is approximately 50% — worse than most cancers.
Moghazy et al. (2010) in Diabetes Research and Clinical Practice conducted a 30-patient prospective study of bee honey dressing in DFUs not responsive to conventional therapy. Outcomes:
- Healing rate: 43% complete closure within 3 months
- Significant improvement in 43% additional patients
- Wound culture clearance in 80% of initially-infected wounds
- Cost per healed wound approximately 25% of historical conventional-care comparator
The Eddy et al. (2008) Wisconsin Medical Journal paper "Practical considerations of using topical honey for neuropathic diabetic foot ulcers" reports successful application of unprocessed honey on otherwise-recalcitrant neuropathic DFUs, with healing of ulcers that had failed multiple advanced wound modalities over years.
The Imran et al. 2015 RCT in Journal of College of Physicians and Surgeons Pakistan randomized 348 DFU patients to manuka honey dressing versus standard saline gauze dressing. Results favored manuka: median healing time 18 weeks vs 29 weeks (p < 0.001), and bacterial culture clearance at 4 weeks 78% vs 35% (p < 0.001).
For DFUs specifically, the practical advantages of manuka honey are:
- Activity against polymicrobial flora including MRSA, Pseudomonas, and anaerobes — the typical DFU microbiome
- Autolytic debridement of slough and necrotic tissue without surgical sharps
- Maintenance of moist wound environment that supports granulation tissue formation
- Compatibility with offloading devices (total contact casts, removable boots) because the dressing can be left in place for several days
- Cost: medical-grade manuka dressings are expensive per gram but inexpensive per healed wound when they accelerate closure
See our Diabetes page for the broader management of the underlying disease and our Diabetic Foot Ulcers page (if available) for additional wound-specific management.
Partial-Thickness Burn Trials
The strongest evidence base for honey in wound care is in partial-thickness burns. Multiple randomized trials and the 2015 Cochrane systematic review concluded that honey accelerates healing of partial-thickness burns compared to conventional dressings (silver sulfadiazine cream, polyurethane film, paraffin gauze).
Subrahmanyam (1998) in Burns randomized 50 patients with superficial burns to honey dressing versus 1% silver sulfadiazine. Mean healing time was 9.4 days for the honey arm versus 15.6 days for silver sulfadiazine (p < 0.001). Bacterial colonization rates were also lower with honey.
Multiple subsequent Subrahmanyam trials (in Burns, Annals of Burns and Fire Disasters, and British Journal of Surgery) replicated this finding across several hundred additional patients in different burn etiologies (thermal, chemical, electrical) and depths. The Cochrane review's burn-specific meta-analysis concluded with moderate-quality evidence that honey is more effective than conventional dressings for partial-thickness burns — median 4-5 day reduction in time to healing.
The mechanism for burn benefit overlaps but extends beyond the antibacterial activity: the osmotic effect of honey reduces wound edema (a major contributor to depth-progression of burn injury in the first 48 hours), the low pH may improve tissue oxygenation, and the maintained moist wound environment optimizes re-epithelialization rate. For deeper burns (full-thickness, third-degree), honey is not a primary therapy — these require surgical debridement and grafting — but Medihoney can be used as a donor-site dressing for skin-graft harvest sites.
For thermal burn first-aid before professional medical care, honey is not recommended over the established cool-water cooling protocol (20 minutes of cool but not cold running water) — cooling is the priority. Manuka honey enters the algorithm at the dressing stage, after cooling and initial wound assessment.
Autolytic Debridement and Exudate Management
One of the practical clinical advantages of manuka honey in chronic wound care is its dual action as both an antibacterial agent and an autolytic debridement agent. Slough and fibrinous exudate are barriers to healing — chronic wounds with persistent slough rarely re-epithelialize, regardless of how clean the bacterial culture is. Conventional approaches to debridement include sharp (scalpel), mechanical (wet-to-dry dressings, ultrasonic), enzymatic (collagenase), and autolytic (occlusive dressings that allow endogenous proteases to dissolve necrotic tissue). Each has limitations — sharp debridement is painful and requires skilled practitioners; mechanical debridement can damage healthy tissue; enzymatic debridement is expensive and slow; autolytic debridement requires intact host wound fluid chemistry that is often impaired in chronic wounds.
Manuka honey's osmotic action provides a fifth debridement modality. The hypertonic honey draws water out of necrotic tissue, softening and loosening slough so that it can be wiped away at dressing changes. Combined with the antibacterial activity that reduces the bacterial bioburden in the slough, this produces measurable slough reduction within days. The Gethin trial above (67% slough reduction at 4 weeks with manuka) is representative of clinical experience.
Exudate management is the other practical consideration. Heavily exudating wounds will dilute applied honey and reduce both its antibacterial concentration and its osmotic effect. Two approaches manage this:
- Calcium-alginate-impregnated honey dressings — the alginate fiber absorbs exudate and gels in place, maintaining honey contact with the wound bed
- Frequent dressing changes — for heavily exudating wounds, daily dressing changes maintain a therapeutic honey concentration in the wound bed
For low-exudate wounds, dressings can typically be left in place for 3-7 days, balancing antibacterial activity (peak in the first 24-48 hours after application as MGO concentration is highest in undiluted honey) with practical convenience.
Clinical Application Protocols
Practical protocols for medical-grade manuka honey in outpatient or wound-clinic settings:
- Wound assessment — document wound dimensions (length, width, depth), tissue type (granulation, slough, eschar percentages), exudate volume and character, surrounding skin condition, signs of infection. Culture if cellulitis, systemic signs, or no progress after 2 weeks.
- Wound cleansing — gentle saline or commercial wound cleanser to remove loose debris and surface bacteria. Do not aggressively scrub healthy granulation tissue.
- Honey application — apply medical-grade manuka honey (UMF 12+ to 18+, or equivalent MGO 350-700) generously to the entire wound bed. For cavity wounds, fill the cavity. Aim for a layer at least 5 mm thick to maintain therapeutic concentration as exudate dilutes it.
- Secondary dressing — non-adherent contact layer or absorbent secondary dressing to manage exudate and contain honey at the wound site. For dependent body sites (e.g. lower leg), film or foam secondary dressings prevent honey from migrating.
- Outer dressing — compression bandage for venous leg ulcers (this is the primary therapy for VLU; manuka is the adjunct). Offloading device for diabetic foot ulcers. Standard absorbent dressing for non-pressure-dependent wounds.
- Dressing change frequency — daily for heavily exudating wounds, every 2-3 days for moderate exudate, up to weekly for low-exudate clean wounds. Adjust based on wound response.
- Progress monitoring — weekly wound measurement and photographic documentation. Expect bacterial culture clearance within 2-4 weeks and visible slough reduction within 1-2 weeks. Lack of progress at 4 weeks should prompt reassessment of the underlying diagnosis (vascular insufficiency, osteomyelitis, malignancy, atypical infection).
- Duration — manuka honey can be used throughout the healing process from inflammation through proliferation. Discontinue when the wound is fully re-epithelialized.
Cautions and Contraindications
- Infants under 12 months — absolute contraindication. Raw honey of any kind, including unirradiated manuka, can contain Clostridium botulinum spores. The immature infant gut cannot prevent germination and toxin production, and infant botulism is a life-threatening condition. Medical-grade gamma-irradiated Medihoney is theoretically safer in this regard, but the practical recommendation remains: no honey of any type, by any route, for any infant under 1 year of age. This applies even to the smallest taste.
- Honey allergy / bee allergy — rare but documented. Test on a small area before extensive application in patients with known bee or pollen allergies. Systemic reactions are extremely rare with topical use but theoretically possible.
- Diabetes (systemic) — topical honey application has negligible systemic glucose effect because absorption from intact or wound tissue is minimal. Oral consumption is a different matter and should be counted against carbohydrate budget.
- Stinging sensation — common in the first 5-10 minutes after application, particularly in wounds with substantial inflammation. Generally subsides spontaneously. If severe or persistent, manuka honey may not be the right choice for that patient.
- Wound color change — honey will temporarily stain wound tissue yellow-amber. This is cosmetic and does not indicate infection. Patients should be warned in advance to prevent alarm.
- Drug interactions — no clinically significant drug interactions with topical use. Oral ingestion of large amounts (rare) could theoretically affect medications metabolized by the same hepatic pathways, but in practice this is not a concern.
- Counterfeit product — the global manuka market includes substantial counterfeit and adulterated product. Use only UMF-certified or MGO-certified product from reputable suppliers. Comvita, Manuka Doctor, Wedderspoon, and Watson & Son are commonly recommended brands; Medihoney is the FDA-cleared medical product.
- Cost — medical-grade manuka dressings are expensive ($30-$60 per dressing depending on size). Insurance coverage varies by jurisdiction and indication; most U.S. Medicare carriers cover Medihoney for documented chronic wounds meeting specific criteria.
Key Research Papers
- Molan PC (1992). The antibacterial activity of honey. 1. The nature of the antibacterial activity. Bee World, 73(1): 5-28. — PubMed
- Mavric E, Wittmann S, Barth G, Henle T (2008). Identification and quantification of methylglyoxal as the dominant antibacterial constituent of Manuka (Leptospermum scoparium) honeys from New Zealand. Mol Nutr Food Res, 52(4): 483-9. — PubMed
- Adams CJ et al. (2008). Isolation by HPLC and characterisation of the bioactive fraction of New Zealand manuka (Leptospermum scoparium) honey. Carbohydr Res, 343(4): 651-9. — PubMed
- Cooper RA, Molan PC, Harding KG (2002). The sensitivity to honey of Gram-positive cocci of clinical significance isolated from wounds. J Appl Microbiol, 93(5): 857-63. — PubMed
- Cooper RA et al. (2010). Absence of bacterial resistance to medical-grade manuka honey. Eur J Clin Microbiol Infect Dis, 29(10): 1237-41. — PubMed
- Gethin G, Cowman S (2008). Manuka honey vs. hydrogel: a prospective, open label, multicentre, randomised controlled trial to compare desloughing efficacy and healing outcomes in venous ulcers. J Clin Nurs, 18(3): 466-74. — PubMed
- Robson V, Dodd S, Thomas S (2009). Standardized antibacterial honey (Medihoney) with standard therapy in wound care: randomized clinical trial. J Adv Nurs, 65(3): 565-75. — PubMed
- Subrahmanyam M (1998). A prospective randomised clinical and histological study of superficial burn wound healing with honey and silver sulfadiazine. Burns, 24(2): 157-61. — PubMed
- Jull AB et al. (2015). Honey as a topical treatment for wounds. Cochrane Database Syst Rev, CD005083. — PubMed
- Eddy JJ, Gideonsen MD, Mack GP (2008). Practical considerations of using topical honey for neuropathic diabetic foot ulcers. WMJ, 107(4): 187-90. — PubMed
- Moghazy AM et al. (2010). The clinical and cost effectiveness of bee honey dressing in the treatment of diabetic foot ulcers. Diabetes Res Clin Pract, 89(3): 276-81. — PubMed
- Imran M, Hussain MB, Baig M (2015). A randomized, controlled clinical trial of honey-impregnated dressing for treating diabetic foot ulcer. J Coll Physicians Surg Pak, 25(10): 721-5. — PubMed
PubMed Topic Searches
- PubMed: Manuka honey wound healing RCTs
- PubMed: Medihoney / leptospermum wound dressing
- PubMed: Methylglyoxal antibacterial mechanism
- PubMed: Manuka honey venous leg ulcer
- PubMed: Manuka honey diabetic foot ulcer
- PubMed: Honey vs silver sulfadiazine for burns
Connections
- Manuka Honey Overview
- Manuka Honey Benefits Hub
- Antimicrobial Spectrum
- Digestive & Sore Throat
- Skin Conditions & Acne
- Diabetes
- Staphylococcus aureus / MRSA
- Pseudomonas aeruginosa
- Cellulitis
- Collagen (Wound Healing)
- Silver Nanoparticles
- Tea Tree
- Honey (Conventional)
- All Herbs