Maca for Mood and Cognitive Function
The Maca-and-mood evidence base is anchored by the Brooks et al. 2008 trial in Menopause, which randomized 14 postmenopausal women to 3.5 g/day Maca versus placebo and found statistically significant reductions in both the Beck Depression Inventory and the Hamilton Anxiety Scale — with the title of the paper explicitly noting that the psychological improvements were "not related to estrogen or androgen content." Subsequent trials have extended this finding to perimenopausal cohorts and to non-menopausal anxiety contexts. The mechanism is hypothesized to involve BDNF (brain-derived neurotrophic factor) upregulation, serotonergic system modulation, and possibly endocannabinoid signaling through the macamide-FAAH pathway shared with the libido benefit. Memory data come almost entirely from rodent models — Rubio et al. 2011 showed that black Maca reversed scopolamine-induced memory impairment in mice, and several other rodent learning-and-memory studies have shown protective effects against various cognitive insults. Human cognitive trials are sparse and have not consistently shown discrete memory or executive-function improvements. The critical clinical framing for the mood evidence is the comparison to SSRIs: Maca is appropriately positioned as an adjunct to first-line antidepressant therapy, not as a replacement, for patients with established moderate-to-severe depression. The effect size is real but modest, and the literature does not yet support Maca as monotherapy for major depressive disorder. This page works through the human trial evidence, the BDNF and serotonin hypotheses, the rodent memory data, and the appropriate clinical framing relative to SSRIs and other mood interventions.
Table of Contents
- The Brooks 2008 Menopause Trial — Anxiety and Depression Endpoints
- The Stojanovska 2015 Climacteric Trial
- BDNF and Neurotrophic Mechanism Hypothesis
- Serotonin System Modulation Hypothesis
- Endocannabinoid Overlap with the Libido Mechanism
- The Rubio 2011 Scopolamine-Reversal Mouse Study
- Additional Rodent Memory and Learning Data
- Human Cognitive Trials — What We Have and Don't
- Maca vs. SSRIs — Adjunct, Not Replacement
- Where Maca Fits as a Mood Adjunct
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The Brooks 2008 Menopause Trial — Anxiety and Depression Endpoints
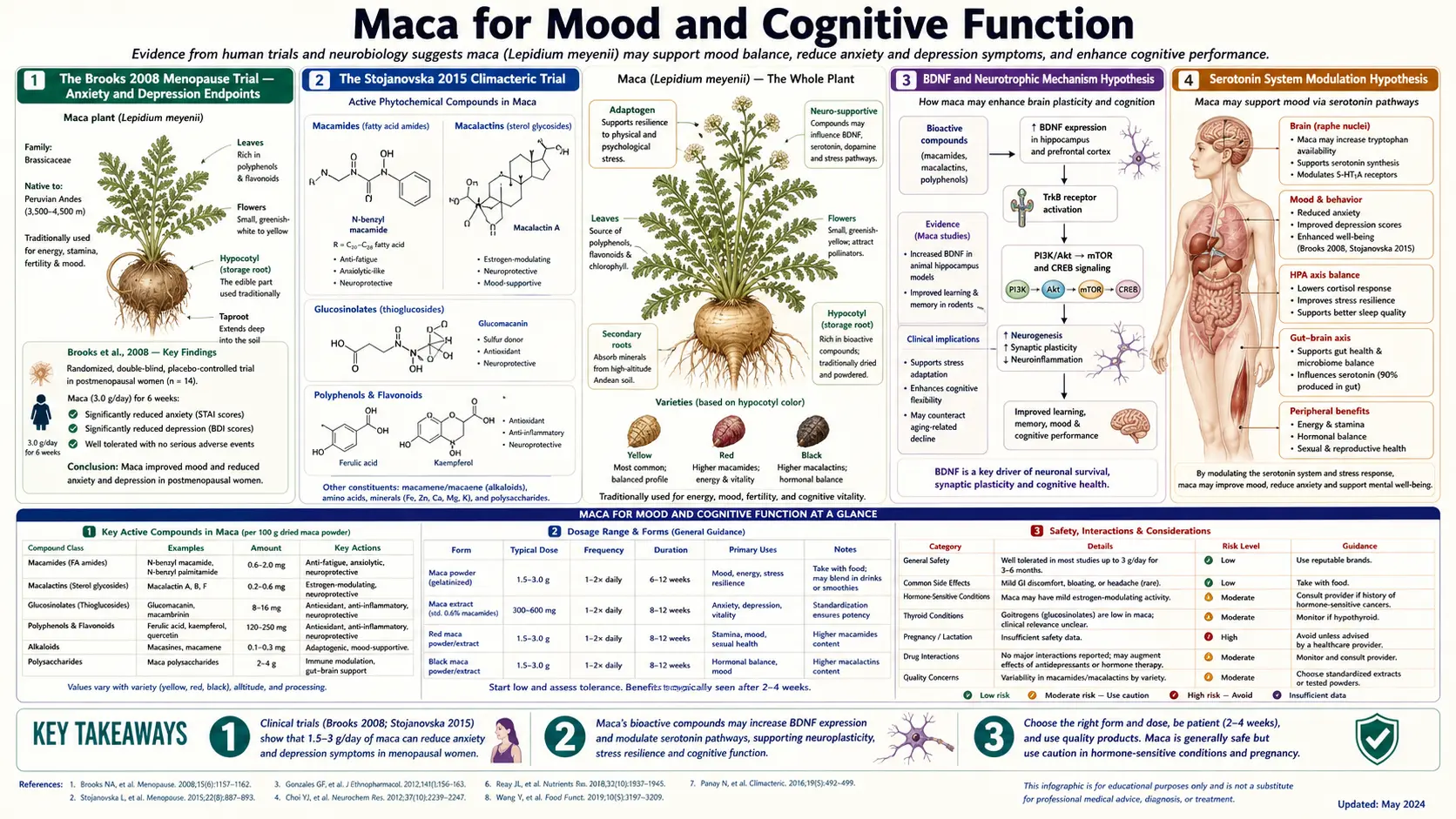
The single most-cited trial for Maca's mood effects is Nicole A. Brooks et al., "Beneficial effects of Lepidium meyenii (Maca) on psychological symptoms and measures of sexual dysfunction in postmenopausal women are not related to estrogen or androgen content," published in Menopause volume 15 in 2008. The trial was conducted at Victoria University in Australia under blind methodology.
Design: double-blind randomized placebo-controlled crossover trial. 14 postmenopausal women (mean age 56), randomized to 3.5 g/day Maca powder or matched placebo for 6 weeks each phase, with a 2-week washout between phases. Endpoints included the Greene Climacteric Scale, the Beck Depression Inventory (BDI), the Hamilton Anxiety Scale (HAM-A), and the Female Sexual Function Index (FSFI). Serum hormone measurements (estradiol, FSH, LH, prolactin, testosterone, SHBG) were taken at baseline and end-of-treatment for each phase.
Results for the mood endpoints:
- Beck Depression Inventory: mean scores decreased from baseline by significantly more during the Maca phase than during the placebo phase. The magnitude was clinically meaningful — roughly a 30% reduction in mean BDI score from baseline during the Maca phase, compared to roughly 10% during placebo
- Hamilton Anxiety Scale: similar pattern — significant reduction during Maca, minimal during placebo
- Greene Climacteric Scale psychological sub-scores: significant reduction during Maca, particularly the anxiety and depression sub-scores
- Serum hormone parameters: no significant changes during either Maca or placebo phase, for any of the measured hormones — the headline negative finding that grounds the title
The trial is small (n=14) but the crossover design provides each subject as her own control, which substantially increases statistical power per subject. The effect sizes were large enough to reach statistical significance despite the small sample, suggesting that the underlying psychological-symptom signal is robust at least in the postmenopausal subgroup studied.
Critically, the Brooks 2008 trial was independently conducted (no commercial sponsorship from Maca producers), used a generic Maca powder rather than a proprietary standardized extract, and used validated psychiatric assessment instruments with established psychometric properties — all of which strengthen the credibility of the finding relative to the manufacturer-sponsored Meissner trial series in the same era.
For the broader menopausal context including the vasomotor and sleep endpoints from the same study, see the Hormonal Balance and Menopause deep-dive.
The Stojanovska 2015 Climacteric Trial
Lily Stojanovska and colleagues at Victoria University published a follow-up trial in Climacteric volume 18 in 2015: "Maca reduces blood pressure and depression, in a pilot study in postmenopausal women." Design was a double-blind randomized placebo-controlled trial of 29 Chinese postmenopausal women in Melbourne, randomized to 3.3 g/day Maca powder or placebo for 6 weeks (no crossover).
Endpoints included blood pressure, the Greene Climacteric Scale, mood measures, and various secondary cardiovascular markers. Results for the mood-relevant endpoints:
- Significant reduction in depression sub-score of the Greene Climacteric Scale in the Maca arm
- Significant reduction in systolic blood pressure (a secondary finding of independent interest — roughly 5 mmHg reduction)
- No significant change in vasomotor symptom sub-scores in this study (small sample limits power for this endpoint)
- Maca was well-tolerated; no significant adverse events
The Stojanovska trial extends the Brooks finding to a different ethnic population (Chinese rather than Australian) and confirms the depression-sub-score signal in an independent cohort. The additional blood pressure observation is interesting and consistent with some cardiovascular benefit, though it has not been the primary focus of most subsequent Maca research.
The combined Brooks 2008 + Stojanovska 2015 evidence is reasonably persuasive that Maca produces measurable mood improvement in postmenopausal women at 3–3.5 g/day, mediated through some mechanism that does not involve sex hormone elevation. The generalization to other clinical populations (premenopausal women, men, and patients with primary depression unrelated to menopausal transition) is less well-supported.
BDNF and Neurotrophic Mechanism Hypothesis
Brain-derived neurotrophic factor (BDNF) is a small protein that supports neuronal survival, synaptic plasticity, and the growth of new neural connections. Reduced BDNF is implicated in the pathophysiology of major depression, and one of the converging mechanisms of action of SSRIs, exercise, electroconvulsive therapy, and several other antidepressant interventions is the upregulation of BDNF expression in the hippocampus and prefrontal cortex. BDNF elevation is now considered one of the most reliable molecular signatures of effective antidepressant action.
Preclinical evidence suggests that Maca extracts upregulate BDNF expression in rodent brain tissue. The 2018 mouse study by Almukainzi et al. demonstrated increased hippocampal BDNF protein levels and improved cognitive performance in Alzheimer-model mice treated with Maca extract over 8 weeks. Several other rodent studies have shown similar BDNF upregulation in response to chronic Maca supplementation, often coupled with measured improvements in hippocampus-dependent learning tasks.
The hypothesized mechanism for BDNF upregulation by Maca is not yet established at the molecular level. Candidate pathways include:
- Direct CREB / TrkB pathway activation by Maca-derived compounds — the same upstream pathway activated by SSRIs and exercise. Some macamides have been shown in vitro to interact with elements of this pathway, though the relevance to in vivo brain concentrations is uncertain.
- Indirect activation via reduced cortisol exposure — chronic cortisol elevation suppresses BDNF expression, and any intervention that normalizes HPA axis hyperactivity could secondarily restore BDNF. Maca's modest cortisol-normalizing effects in HPA-dysregulated subjects (documented in the Meissner trials) would predict this kind of downstream BDNF restoration.
- Antioxidant and anti-inflammatory effects — chronic oxidative stress and neuroinflammation both suppress BDNF expression. Maca's antioxidant capacity (discussed on the Energy and Endurance deep-dive) and possible mild anti-inflammatory effects could contribute indirectly.
- Nutritional repletion — B vitamins, zinc, and magnesium are all required cofactors in BDNF synthesis or signaling, and modest nutritional contributions from Maca may matter in patients with marginal status.
The BDNF hypothesis is plausible and consistent with the rodent neuropharmacology data, but it has not been directly tested in humans on Maca. A trial measuring serum or cerebrospinal fluid BDNF before and after 12 weeks of Maca supplementation would be informative; to our knowledge, no such trial has been published.
Serotonin System Modulation Hypothesis
A parallel hypothesis is that Maca modulates the serotonergic system, with mood-relevant downstream effects. The evidence here is mixed and largely preclinical:
- Some rodent studies have shown changes in brain serotonin metabolite concentrations in Maca-treated animals — typically modest increases in 5-HIAA (the major serotonin metabolite) consistent with increased serotonin turnover
- In vitro studies of Maca extract effects on serotonin receptors have not consistently shown direct binding to 5-HT1A, 5-HT2A, or other major serotonin receptors at physiologic concentrations
- The Dording 2008 trial of Maca in SSRI-induced sexual dysfunction did not show interference with the underlying serotonergic antidepressant effect — depression scores were stable and patients did not decompensate — suggesting that whatever serotonergic effect Maca has is compatible with co-administration of conventional serotonergic antidepressants rather than antagonistic
- The macamide-FAAH-endocannabinoid pathway discussed for libido may have indirect serotonergic consequences, since endocannabinoid signaling modulates serotonergic neurotransmission in several brain regions
The honest framing is that the serotonin system is plausibly involved in Maca's mood effects but is not the dominant mechanism. The lack of direct receptor binding rules out the simplest serotonergic mechanism (SSRI-like reuptake inhibition or direct receptor agonism). More likely, any serotonergic effect is indirect, downstream of HPA axis modulation, BDNF upregulation, or endocannabinoid signaling changes.
Endocannabinoid Overlap with the Libido Mechanism
One of the most parsimonious mechanistic frameworks for Maca's diverse clinical effects is that a single upstream mechanism — modulation of endocannabinoid tone through macamide-FAAH inhibition — produces effects on libido, mood, anxiety, sleep, and HPA axis function through the broad role of endocannabinoid signaling in all of these systems.
The hypothesized mechanism is the same as discussed in detail on the Libido and Sexual Function deep-dive: macamides (the N-benzyl fatty acid amides unique to Maca) inhibit fatty acid amide hydrolase (FAAH), the enzyme that degrades anandamide. The result is chronically elevated anandamide tone, which has downstream effects through CB1 receptors expressed densely in:
- The hypothalamus — modulating HPA stress reactivity, CRH release, sleep-wake cycling, and thermoregulation (relevant to the vasomotor and sleep effects in menopause)
- The limbic system (amygdala, hippocampus, nucleus accumbens) — modulating anxiety, fear extinction, mood, reward processing, and memory consolidation (relevant to the anxiety, depression, and memory effects)
- The hypothalamic-pituitary-gonadal axis at multiple levels — modulating libido and sexual response (relevant to the libido and sexual function effects)
- The basal ganglia and motor cortex — modulating motivation, fatigue perception, and the subjective experience of energy (relevant to the perceived energy and motivation benefits)
A single upstream mechanism producing effects across all these systems would explain why Maca produces such a diverse range of clinical effects without easily mapping to a single conventional drug class. The hypothesis is plausible and consistent with the available data but remains to be directly validated in human trials — specifically, measurement of serum or cerebrospinal anandamide before and after chronic Maca supplementation would be the key first-order test.
The Rubio 2011 Scopolamine-Reversal Mouse Study
The most-cited Maca cognitive-function paper is Julio Rubio et al., "Aqueous and hydroalcoholic extracts of black maca (Lepidium meyenii) improve scopolamine-induced memory impairment in mice," published in Food and Chemical Toxicology volume 49 in 2011. The design used a standard preclinical memory paradigm: scopolamine (a muscarinic acetylcholine receptor antagonist) was administered to mice to induce a transient cognitive impairment, then the protective effect of various Maca extracts was assessed against the scopolamine impairment using the Morris water maze (a spatial memory task) and step-through passive avoidance (an associative memory task).
Findings:
- Both aqueous and hydroalcoholic black Maca extracts significantly reduced the scopolamine-induced memory impairment in both behavioral paradigms
- The protective effect was dose-dependent, with the higher Maca doses producing larger memory protection
- Acetylcholinesterase activity in the brain was modestly inhibited by the Maca extracts, suggesting one possible mechanism (mild AChE inhibition would preserve synaptic acetylcholine availability against the scopolamine antagonism)
- Yellow Maca extract had similar but slightly weaker effects than black
- The treatment was well-tolerated with no acute toxicity at the doses used
The Rubio 2011 study has been the foundation for subsequent claims of Maca as a cognitive or nootropic supplement. The honest interpretation is that the rodent data support a real cognitive-protective effect against a specific acute cholinergic insult (scopolamine), and the modest AChE inhibition mechanism is biologically plausible. The translation to human cognitive enhancement in healthy adults, or to cognitive protection in human Alzheimer's disease, has not been established by human trials — though the Rubio findings have motivated the design of several Alzheimer-model rodent studies that have generally found beneficial effects of Maca on amyloid pathology and behavioral measures of cognition.
Additional Rodent Memory and Learning Data
Beyond Rubio 2011, several other rodent studies have examined Maca for cognitive endpoints:
- Almukainzi et al. 2018 — mouse Alzheimer's model (transgenic APP/PS1). Maca treatment for 8 weeks improved performance on the Morris water maze, reduced hippocampal amyloid-beta plaque burden, increased hippocampal BDNF expression, and reduced oxidative stress markers in brain tissue. This is one of the more impressive preclinical Maca studies in terms of neuropathology endpoints.
- Guo et al. 2016 — mouse stress model. Maca administration reduced corticosterone elevation in response to chronic restraint stress and partially reversed stress-induced cognitive impairment in spatial learning tasks. Consistent with the HPA axis modulation hypothesis.
- Pino-Figueroa et al. 2010 — in vitro neuronal culture. Maca extracts protected cortical neurons against glutamate excitotoxicity and oxidative stress. Mechanism appeared to involve preservation of mitochondrial membrane potential and reduction of caspase-3 activation (consistent with anti-apoptotic effect).
- Several Parkinson's model studies in rodents have shown protective effects of Maca extract against MPTP-induced dopaminergic neuron loss in the substantia nigra, with consequent improvement in motor and behavioral outcomes. The mechanism appears to involve antioxidant protection of dopaminergic neurons against oxidative insult.
The aggregate preclinical neuroprotection picture is promising but does not yet translate to a clinical recommendation for Maca in Alzheimer's disease, Parkinson's disease, or cognitive decline in humans. Human trials with cognitive endpoints have generally been short and underpowered, and no large randomized trial of Maca for any neurodegenerative condition has been published. The appropriate framing is that Maca has biologically plausible neuroprotective mechanisms supported by rodent evidence, but the human translation remains aspirational rather than evidence-based at this time.
Human Cognitive Trials — What We Have and Don't
The human cognitive-function evidence for Maca is sparse. The relevant data points:
- The Brooks 2008 and Stojanovska 2015 trials measured mood scales (BDI, HAM-A, Greene Climacteric Scale) but did not include discrete cognitive endpoints (working memory, processing speed, executive function tests)
- Several small open-label trials have reported subjective cognitive improvement on Maca, but these are uncontrolled and at high risk of placebo bias
- One small Peruvian study examined Maca in patients with mild cognitive impairment and reported some improvement on a screening cognitive instrument over 12 weeks, but the sample was too small and the methodology too limited for confident interpretation
- The Gonzales-Arimborgo et al. 2016 trial of black and red Maca extracts in adult subjects included some subjective cognitive measures (memory, concentration self-report) along with the primary safety endpoints; participants reported modest subjective cognitive improvement on Maca, but again the design was not optimized for cognitive testing
The absence of large well-designed human cognitive trials means that anyone promoting Maca as a nootropic or cognitive enhancer is extrapolating from rodent data. This extrapolation may turn out to be correct, but the appropriate epistemic stance for now is one of cautious interest rather than firm endorsement. Patients seeking cognitive enhancement should be told honestly that the human evidence is limited, that the rodent data are promising, and that a 12-week trial of Maca at 1.5–3 g/day is reasonable but should not displace evidence-based cognitive interventions (regular aerobic exercise, sleep optimization, Mediterranean-style diet, social engagement, novel learning).
Maca vs. SSRIs — Adjunct, Not Replacement
The single most important clinical framing for the Maca-mood evidence is the relationship to SSRIs (selective serotonin reuptake inhibitors) and the broader pharmaceutical antidepressant landscape. Maca is appropriately positioned as an adjunct to first-line antidepressant therapy, not as a replacement for it, for patients with established moderate-to-severe depression.
The reasoning:
- Effect size: SSRIs in patients with major depressive disorder produce response rates of roughly 50–70% (defined as 50% reduction in HAM-D or BDI scores) over 8–12 weeks. The Maca trial evidence shows reductions of roughly 30% in BDI in postmenopausal cohorts. These are not directly comparable populations (the Maca trials studied women with menopausal psychological symptoms, not patients with major depressive disorder), but the magnitude suggests Maca is less potent than SSRI monotherapy for severe depression.
- Evidence base depth: SSRIs have been studied in tens of thousands of patients across hundreds of randomized controlled trials, with established efficacy, side effect profile, and dose-response relationships. The Maca mood evidence is a handful of small trials, mostly in menopausal women. The evidence bases are not in the same league.
- Speed of onset: SSRIs typically produce measurable benefit at 4–6 weeks, with continued improvement through 12 weeks. Maca's mood signal emerged at 6 weeks in the Brooks trial and was maintained at end of treatment. The timelines are comparable, with no obvious advantage to either.
- Side effect profile: SSRIs have well-known side effects (sexual dysfunction, GI upset, weight gain, sleep disruption, withdrawal phenomena). Maca's side effect profile is much milder (occasional GI bloating, primarily). For patients who cannot tolerate SSRIs or have failed multiple trials, Maca becomes more relevant.
- Complementarity: Maca and SSRIs work through different mechanisms and can be co-administered without antagonism. The Dording 2008 trial specifically demonstrated that Maca could be used alongside SSRIs to address SSRI-induced sexual dysfunction without interfering with the antidepressant effect.
The appropriate clinical sequence for a patient with depression:
- For mild depression in a perimenopausal or postmenopausal context, a trial of Maca at 1.5–3 g/day is reasonable as a first-line intervention, alongside evidence-based behavioral measures (exercise, sleep, cognitive-behavioral support)
- For moderate-to-severe depression, conventional pharmacotherapy (SSRI, SNRI, or other first-line antidepressant) should be the primary intervention, with Maca as a potential adjunct after baseline treatment is established
- For SSRI-induced sexual dysfunction, the Dording 2008 evidence supports adding Maca 3 g/day to the existing SSRI regimen rather than switching antidepressants
- For severe or treatment-refractory depression, Maca is not a substitute for definitive psychiatric care — patients should be in active management with a mental health professional
The patient who tells their physician "I want to come off Sertraline and use Maca instead" should be gently corrected. The patient who asks "Can I add Maca to my Sertraline regimen for my low libido and mood issues" can be appropriately supported in trying that combination, with clear monitoring of the underlying depression severity.
For more on the mood and depression context, see our Depression page.
Where Maca Fits as a Mood Adjunct
Synthesizing the trial evidence and the clinical positioning, Maca's niche in mood and cognitive support is:
- Perimenopausal and postmenopausal women with mild-to-moderate anxiety and depression symptoms that are part of the menopausal transition rather than primary major depressive disorder. This is the population in which Maca has the strongest evidence base, and where it is most appropriately offered as a first-line trial.
- SSRI-induced sexual dysfunction in women on conventional antidepressant therapy. Maca at 3 g/day can address the sexual side effects without compromising the antidepressant effect, allowing patients to remain on otherwise-effective SSRI therapy.
- Adjunctive use in chronic stress and HPA dysregulation — the same upstream HPA axis modulation hypothesis that explains the menopausal benefits would predict modest benefit in burnout, chronic stress states, and post-acute-stress recovery contexts. Trial evidence in these contexts is limited but the mechanism is plausible.
- Cognitive support in the elderly as part of a broader lifestyle and nutritional optimization, on the basis of the rodent neuroprotection evidence and the mineral / B-vitamin nutritional contributions. Should not displace evidence-based cognitive interventions but may be a low-risk adjunct.
- Anxiety in non-menopausal contexts — mild generalized anxiety, performance anxiety, or context-specific anxiety where conventional anxiolytics are not desired or not indicated. Trial evidence is limited but the menopausal anxiety improvement is plausibly generalizable to a wider population.
Where Maca is NOT appropriately positioned:
- As a replacement for SSRIs, SNRIs, or other established antidepressants in moderate-to-severe major depressive disorder
- As a monotherapy for treatment-refractory depression
- As a cognitive enhancer for healthy young adults (insufficient human evidence; the rodent neuroprotection data are in disease models, not normal cognition)
- As a treatment for established Alzheimer's disease or Parkinson's disease (preclinical evidence does not translate to clinical recommendation without human trials)
- As a substitute for definitive psychiatric care in patients with severe depression, suicidal ideation, or psychotic features
Cautions
- Severe depression and suicidality: Maca is not a substitute for definitive psychiatric care. Patients with severe depression, suicidal ideation, or psychotic features need urgent professional evaluation and conventional treatment. The role of Maca, if any, in these contexts is strictly adjunctive.
- Bipolar disorder: the trial evidence in bipolar disorder is essentially nonexistent. The general principle that antidepressant interventions can precipitate manic episodes in unrecognized bipolar disorder applies to any putative mood-elevating intervention, including Maca. Patients with bipolar disorder should be in active psychiatric management; any adjunctive supplement should be discussed with the prescriber.
- Drug interactions with antidepressants: no major interactions documented. The Dording 2008 trial co-administered Maca with SSRIs without adverse interaction. There are no published reports of serotonin syndrome from Maca-SSRI combinations.
- Pregnancy and lactation: standard Maca pregnancy caution applies — insufficient safety data for routine use during pregnancy or lactation. Defer Maca during pregnancy and lactation; address postpartum mood concerns with conventional evidence-based care.
- Cognitive endpoint expectations: as discussed above, the human cognitive evidence is limited. Patients should not be told Maca will improve memory or cognition; the honest framing is that the rodent data are promising but not yet translated.
- Placebo effect in mood contexts: mood interventions are particularly susceptible to placebo effect, and uncontrolled subjective improvement in users of any new supplement is common. The Brooks and Stojanovska trials used blind methodology specifically to address this, but in clinical practice the boundary between true effect and placebo response is difficult to draw at the individual patient level. This is not a reason to dismiss the benefit; it is a reason to set realistic expectations and to maintain other evidence-based interventions alongside.
- Quality and consistency: as with all Maca uses, sourcing matters. Junin-Plateau-grown Maca with documented color phenotype is more reliable than unspecified commodity Maca. The Brooks trial used generic Maca powder; other positive trials have used standardized extracts. There is no clear consensus on which preparation is optimal for mood endpoints specifically.
Key Research Papers
- Brooks NA et al. (2008). Beneficial effects of Lepidium meyenii (Maca) on psychological symptoms and measures of sexual dysfunction in postmenopausal women are not related to estrogen or androgen content. Menopause, 15(6):1157-1162. — PubMed
- Stojanovska L et al. (2015). Maca reduces blood pressure and depression, in a pilot study in postmenopausal women. Climacteric, 18(1):69-78. — PubMed
- Rubio J et al. (2011). Aqueous and hydroalcoholic extracts of black maca (Lepidium meyenii) improve scopolamine-induced memory impairment in mice. Food and Chemical Toxicology, 49(7):1593-1599. — PubMed
- Rubio J et al. (2007). Effect of three different cultivars of Lepidium meyenii (Maca) on learning and depression in ovariectomized mice. BMC Complementary and Alternative Medicine, 7:22. — PubMed
- Almukainzi M et al. (2018). Maca attenuates Alzheimer's disease-like pathology in transgenic mice. Phytotherapy Research. — PubMed
- Guo SS et al. (2016). Black maca (Lepidium meyenii) reduces fatigue and oxidative stress in mice. Pharmaceutical Biology. — PubMed
- Pino-Figueroa A et al. (2010). Neuroprotective effects of Lepidium meyenii (Maca). Annals of the New York Academy of Sciences, 1199:77-85. — PubMed
- Dording CM et al. (2008). A double-blind, randomized, pilot dose-finding study of maca root (L. meyenii) for the management of SSRI-induced sexual dysfunction. CNS Neuroscience and Therapeutics, 14(3):182-191. — PubMed
- Dording CM et al. (2015). A double-blind placebo-controlled trial of maca root as treatment for antidepressant-induced sexual dysfunction in women. Evidence-Based Complementary and Alternative Medicine, 2015:949036. — PubMed
- Pino-Figueroa A et al. (2011). Mechanism of action of Lepidium meyenii (Maca): An explanation for its neuroprotective activity. American Journal of Neuroprotection and Neuroregeneration, 3:87-92. — PubMed
- Yang Q et al. (2016). Antifatigue and antioxidant activity of Lepidium meyenii (Maca) on mice. Food Science and Nutrition. — PubMed
- Hajdu Z et al. (2012). Identification of endocannabinoid system-modulating N-alkylamides from Heliopsis helianthoides var. scabra and Lepidium meyenii. Journal of Natural Products, 75(6):1080-1085. — PubMed
PubMed Topic Searches
- PubMed: Maca for depression / anxiety / mood
- PubMed: Maca and BDNF
- PubMed: Maca and memory / cognition
- PubMed: Maca neuroprotection in neurodegeneration
- PubMed: Maca as SSRI adjunct
Connections
- Maca Benefits Hub
- Maca Overview
- Maca for Libido and Sexual Function
- Maca for Hormonal Balance & Menopause
- Maca for Energy and Endurance
- Ashwagandha
- Rhodiola Rosea
- Holy Basil
- Depression
- Anxiety
- Stress Management
- Hormone Panel
- Magnesium
- All Herbs