Maca for Libido and Sexual Function
Maca's reputation as a libido tonic predates modern pharmacology by at least eight centuries — Spanish chroniclers described Andean cattlemen feeding Maca to herds at altitude to improve fertility, and the same root has long held a place in Andean kitchens as a sexual tonic for both men and women. The modern controlled trial era began with Gloria Gonzales's 2002 Andrologia paper, which randomized men to 1.5 or 3 g/day of Maca and found a statistically significant increase in self-reported sexual desire at week 8 — while serum testosterone, estradiol, and LH remained unchanged. A subsequent 2010 trial extended the effect to postmenopausal women on SSRIs (the SSRI-induced sexual dysfunction context), and the Shin et al. 2010 BMC Complementary Medicine systematic review pooled four trials and judged the libido signal real but modest. The hypothesized active compounds are the macamides — a class of polar lipid amides unique to Maca that may potentiate endocannabinoid signaling rather than mimicking any sex hormone. This page walks through the trial evidence, the macamides hypothesis, the contrast with conventional hormonal supplements, and the practical 1.5–3 g/day black-Maca dosing.
Table of Contents
- Traditional Andean Use as a Sexual Tonic
- The Gonzales 2002 Men's Libido Trial
- The Gonzales / Dording 2010 Women's Trial
- The Shin 2010 BMC Systematic Review
- Sperm Parameters and Male Fertility
- The Macamides + Macaenes Hypothesis
- Why Maca Is NOT a Hormonal Supplement
- Contrast with Testosterone, DHEA, and Yohimbine
- Practical Dose (1.5–3 g/day) and Black-Phenotype Selection
- What to Expect — Realistic Effect Size and Timeline
- Cautions
- Key Research Papers
- Connections
- Featured Videos
Traditional Andean Use as a Sexual Tonic
Maca cultivation on the high Andean plateau dates back at least two thousand years, with archaeological evidence from the Junin region of Peru placing domesticated Lepidium meyenii in the human food supply by the late Pre-Columbian era. From the earliest documentation by Spanish chroniclers in the sixteenth century, two themes recur in the ethnographic record. The first is altitude tolerance — Maca was the staple food of human populations and the cattle they herded at elevations where ordinary crops failed and Spanish horses lost weight and stopped breeding. The second is sexual function, frequently mentioned in the same breath as fertility: Spanish accounts describe Andean ranchers feeding Maca to cattle to restore breeding capacity, and Maca was incorporated into ritual and ceremonial use as an aphrodisiac in pre-Columbian Andean cosmology.
This tradition persisted unbroken through the colonial and republican periods. By the mid-twentieth century, Maca powder and Maca confections (Maca chicha, a fermented drink; Maca cake; Maca added to porridge) were standard household items across the high Peruvian Andes, used both as a daily nutrient and as a specific sexual and fertility tonic. The contemporary global market — Maca is now exported as a powder and capsule supplement to nearly every developed-world country — began in the mid-1990s when Western interest in herbal sexual tonics elevated demand to the point that the Peruvian government formally protected Maca as a "Genetic Heritage of Peru" in 2003, restricting commercial export of seed and root stock.
The traditional use is therefore not a marketing invention. The clinical-trial evidence summarized below was generated in response to a pre-existing ethnobotanical claim about libido and fertility — not the other way around — which is methodologically important because the trial endpoints were chosen to match the traditional indication rather than data-mining for any incidental signal.
The Gonzales 2002 Men's Libido Trial
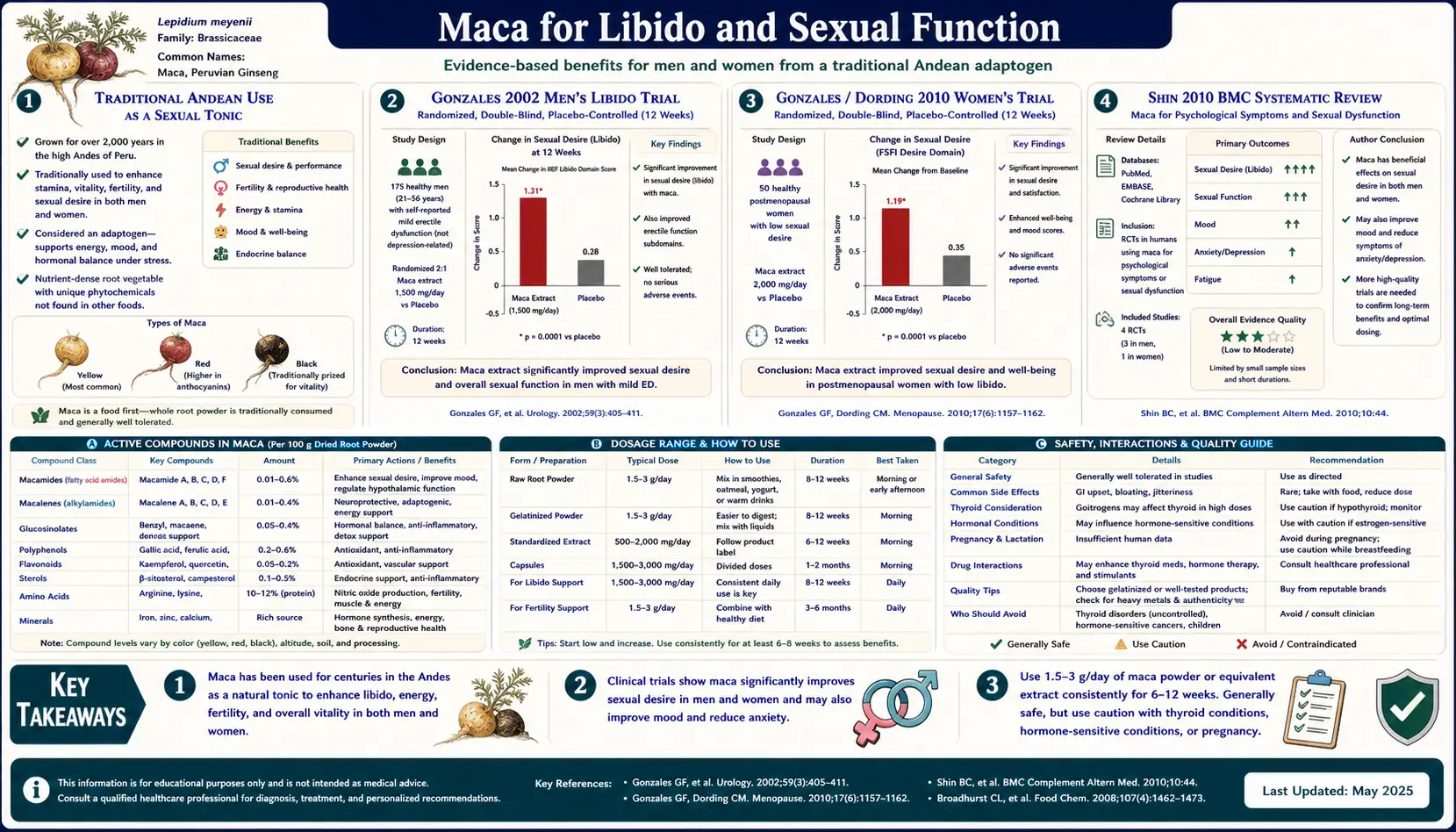
The landmark modern trial is Gloria F. Gonzales et al., "Effect of Lepidium meyenii (MACA) on sexual desire and its absent relationship with serum testosterone levels in adult healthy men," published in Andrologia volume 34 in 2002. The design was a 12-week double-blind randomized placebo-controlled trial in 57 men aged 21 to 56, randomized to placebo, 1.5 g/day Maca, or 3 g/day Maca. The primary endpoint was self-reported sexual desire on a validated questionnaire administered at baseline, 4 weeks, 8 weeks, and 12 weeks. Secondary endpoints included serum testosterone, estradiol, luteinizing hormone (LH), follicle-stimulating hormone (FSH), prolactin, and the Hamilton Anxiety and Depression scales.
The headline result: at week 8 and week 12, both Maca dose groups showed a statistically significant increase in self-reported sexual desire compared to placebo, with no apparent dose-response between 1.5 and 3 g/day (suggesting the effect plateaus at the lower of the two doses tested). The Hamilton anxiety and depression scores did not differ between groups, so the libido effect was not simply a downstream consequence of mood improvement. Critically, serum testosterone, estradiol, LH, FSH, and prolactin showed no significant changes in either Maca group at any timepoint — the libido increase occurred without measurable change in the sex hormone axis.
This was the result that put Maca on the global research map. Most putative aphrodisiac herbs that pass placebo-controlled testing show either a clear hormonal change (testosterone elevation, as with some Tribulus terrestris formulations) or a vascular mechanism (PDE5 inhibition, as with pomegranate and certain icariin preparations). Maca produced a libido signal with neither — pointing toward a different mechanism class entirely.
The trial used a non-specified-color Maca powder (predominantly yellow given the source). Subsequent work has suggested that the libido effect may be stronger with the black phenotype, but Gonzales 2002 itself did not test color-specific preparations.
The Gonzales / Dording 2010 Women's Trial
The Maca-and-women evidence base lagged behind the men's by nearly a decade. The 2010 work most often cited is the Dording et al. randomized double-blind crossover trial in CNS Neuroscience and Therapeutics, which examined 3 g/day Maca versus 1.5 g/day Maca versus placebo over 12 weeks in 45 women with SSRI-induced sexual dysfunction. This is a clinically important population because SSRI-induced sexual dysfunction (anorgasmia, low desire, vaginal dryness) is one of the most common reasons women discontinue otherwise-effective antidepressant therapy — and Maca offered the prospect of an intervention without serotonin- or hormone-axis confounding.
Results: the 3 g/day group showed a significant improvement in the Arizona Sexual Experience Scale (ASEX) and the Massachusetts General Hospital Sexual Function Questionnaire (MGH-SFQ) by week 12, compared to placebo. The 1.5 g/day group showed a smaller, non-significant improvement — suggesting that for the SSRI-dysfunction indication specifically, the higher dose may be more reliable. Hormone parameters again did not change.
A parallel earlier trial by Brooks et al. (2008) in Menopause examined 3.5 g/day Maca in postmenopausal women not on SSRIs and reported improvement in sexual dysfunction scores along with anxiety and depression. The Brooks paper specifically titled its conclusion to highlight that the improvements "are not related to estrogen or androgen content" — reinforcing the non-hormonal mechanism. We treat the Brooks 2008 paper in more depth on the Mood and Cognitive Function deep-dive page.
The take-home for the women's sexual function evidence: smaller than the men's literature, but converging on the same conclusion — modest libido benefit at 3 g/day, no detectable hormonal change, and a particular niche in the SSRI-induced dysfunction population where conventional alternatives (bupropion augmentation, drug holidays) carry their own drawbacks.
The Shin 2010 BMC Systematic Review
Byung-Cheul Shin, Myeong Soo Lee, Eun Jin Yang, Hyun-Suk Lim, and Edzard Ernst published "Maca (L. meyenii) for improving sexual function: a systematic review" in BMC Complementary and Alternative Medicine volume 10 in 2010. The reviewers searched 17 databases for any randomized controlled trial of Maca with a sexual function endpoint, identified four trials meeting inclusion criteria (Gonzales 2002, Zenico 2009, Brooks 2008, Stone 2009 — with the Stone trial actually examining cycling time-trial performance rather than libido directly, but including a libido secondary endpoint), and assessed methodological quality using the Jadad score.
The reviewers' conclusion was carefully hedged: the four trials provided "some" evidence that Maca improves sexual function, but the body of evidence was limited and the trials were small and heterogeneous in design. They specifically noted that the Edzard Ernst group — well known for skeptical scrutiny of complementary medicine claims — was treating the libido signal as plausible but not yet definitively established. The recommendation was for larger and methodologically tighter trials.
Subsequent meta-analyses have generally reproduced the Shin conclusion: a real but modest libido effect, with effect sizes in the small-to-moderate range on validated sexual function scales, replicated across multiple independent trial sites in Peru, the UK, the US, and Italy. No meta-analysis has identified a serious safety signal or any indication of harm.
For comparison, the effect size of Maca on libido scales is approximately one-third to one-half of the effect size of phosphodiesterase-5 inhibitors (sildenafil, tadalafil) on erectile function in men with mild-to-moderate erectile dysfunction. Maca is not a substitute for PDE5 inhibitors when erectile function is the issue — the mechanism is unrelated. Maca is more appropriately positioned as a libido and sexual-desire tonic, where the conventional pharmaceutical alternatives are limited (testosterone supplementation in low-testosterone men; flibanserin and bremelanotide in women, both with mixed evidence and significant side-effect profiles).
Sperm Parameters and Male Fertility
A separate line of Maca evidence concerns sperm parameters in men, distinct from the libido endpoint. The lead reference is Gonzales et al. 2001 in Asian Journal of Andrology, which examined 1.5 or 3 g/day Maca for 4 months in nine men and reported increased sperm count, sperm motility, and seminal volume. The 2006 follow-up Gonzales paper in Andrologia extended the finding in a larger cohort and specifically used black Maca, which produced larger effects than yellow on sperm parameters.
Mechanistically, the proposed pathway is not via the HPG axis (testosterone, LH, FSH unchanged in all sperm-parameter trials) but via direct effects on spermatogenesis in the seminiferous tubules — possibly through antioxidant protection of the spermatogenic epithelium, possibly through direct effects of macamides or glucosinolates on Sertoli cell function. This is plausible but not definitively mechanistically established.
The clinical relevance for male fertility: Maca has a place in the evaluation of oligospermia and asthenospermia of unclear etiology, particularly in men who have already addressed the obvious factors (heat exposure to the testes, varicocele, hormonal abnormalities, recent infection) and who are exploring adjunctive interventions before in vitro fertilization or intracytoplasmic sperm injection. A three-to-six-month trial of 3 g/day black Maca, with semen analysis before and after, is a low-risk option in this context. It should not delay diagnostic workup or definitive fertility treatment when those are indicated.
For more on male fertility evaluation and supportive nutrition, see our Testosterone Test page and the related lab work needed to characterize subfertility before adding adjuncts.
The Macamides + Macaenes Hypothesis
The leading mechanistic hypothesis for Maca's sexual-function effect involves two related chemical classes that are unique to Lepidium meyenii: macamides and macaenes. The macamides are N-benzyl fatty acid amides — structurally, a benzylamine head group attached via an amide bond to a fatty acid tail (palmitic, oleic, linoleic, linolenic, and several others have been identified). The macaenes are unsaturated fatty acids with a related structural motif, generally co-occurring with the macamides in Maca root.
The crucial structural observation is that macamides are close cousins of anandamide (N-arachidonoylethanolamine), the principal endogenous endocannabinoid that activates the cannabinoid CB1 receptor in the central and peripheral nervous system. Endocannabinoid signaling is known to play a role in sexual desire and arousal (one of the few well-replicated effects of acute cannabis use is increased subjective sexual desire, mediated through CB1).
The macamide-endocannabinoid hypothesis has two specific molecular legs:
- Several macamides have been shown in vitro to inhibit fatty acid amide hydrolase (FAAH), the enzyme that degrades anandamide. FAAH inhibition is a well-established pharmaceutical strategy for augmenting endogenous endocannabinoid tone — several FAAH-inhibitor drugs have reached clinical trials for chronic pain, anxiety, and mood disorders. If Maca-derived macamides act as weak natural FAAH inhibitors, they would chronically elevate anandamide tone, with downstream effects on sexual desire, mood, and HPA stress response.
- Independent in vitro studies have suggested direct partial agonism at the CB1 receptor by certain macamides, though the binding affinities are modest and the pharmacologic significance at typical Maca consumption is debated.
Both legs of this hypothesis remain to be validated in vivo in humans. No published study has, for instance, measured serum anandamide before and after Maca supplementation, or used a CB1 antagonist to test whether the libido effect is endocannabinoid-mediated. The hypothesis is biologically plausible and structurally consistent but not yet directly tested.
The practical consequence: the macamide concentration of any commercial Maca preparation matters more than the total Maca powder weight. High-end suppliers now standardize on macamide content (typically expressed as mg per gram of dried Maca), and the black phenotype consistently shows the highest macamide concentration of the four colors. This is the empirical basis for preferring black Maca specifically for the libido indication.
Why Maca Is NOT a Hormonal Supplement
A persistent confusion in the popular Maca literature is the suggestion that Maca "balances hormones" by acting like estrogen or testosterone. The clinical and in vitro evidence is unambiguous that Maca does not bind sex hormone receptors at any physiologically relevant concentration. The specific evidence:
- Every adequately-powered trial measuring serum testosterone, estradiol, progesterone, LH, FSH, or prolactin before and after Maca supplementation has reported no significant change. This is true in men (Gonzales 2002), in postmenopausal women (Brooks 2008, Meissner 2006), and in women with SSRI-induced sexual dysfunction (Dording 2010).
- In vitro receptor binding studies have tested Maca extracts at supraphysiologic concentrations against the androgen receptor, the estrogen receptor (both alpha and beta isoforms), and the progesterone receptor, and have not detected meaningful binding affinity.
- In vitro enzyme assays have ruled out significant inhibition of aromatase (the testosterone-to-estradiol converter) and 5-alpha-reductase (the testosterone-to-DHT converter) by Maca extracts.
This negative finding is the clinically actionable distinction between Maca and the genuine phytoestrogens or hormonal-precursor supplements. Soy isoflavones (genistein, daidzein) bind the estrogen receptor beta isoform with meaningful affinity. Black cohosh has complex serotonergic and possibly weakly estrogenic effects (the literature is contested). DHEA and pregnenolone are direct precursors to steroid hormones that elevate serum testosterone and estradiol on supplementation. All three categories are appropriately contraindicated or used with great caution in patients with hormone-receptor-positive breast cancer, estrogen-sensitive uterine fibroids, endometriosis, or active prostate cancer.
Maca does not share these contraindications by mechanism. A woman with a history of ER-positive breast cancer who is on tamoxifen or an aromatase inhibitor and is suffering from low libido as a side effect of treatment can reasonably consider a trial of Maca — with her oncology team's knowledge — because there is no mechanistic basis for Maca to stimulate residual hormone-sensitive tumor cells. This is the single most important clinical point on the page, and the reason Maca occupies a distinct niche in integrative oncology supportive care.
For the parallel discussion in the menopause-symptoms context, see the Hormonal Balance and Menopause deep-dive.
Contrast with Testosterone, DHEA, and Yohimbine
To position Maca correctly in the libido and sexual-function landscape, it helps to compare it to the three most common alternatives.
- Testosterone replacement therapy (TRT) — the conventional treatment for hypogonadal men with documented low serum testosterone and symptoms. TRT produces a large effect on libido in genuinely deficient men, often within 4–8 weeks. It does nothing for eugonadal men with normal testosterone, and it carries a non-trivial risk profile (erythrocytosis, prostate considerations, cardiovascular debate, fertility suppression). Maca occupies a different niche: it is an option for the eugonadal man with low libido who does not have a hormonal indication for TRT, and it can be used alongside TRT for additive libido effect without redundancy.
- DHEA — a direct hormonal precursor that elevates both testosterone and estradiol downstream. DHEA has some evidence for libido benefit in postmenopausal women but raises androgen and estrogen serum levels, with the corresponding contraindications in hormone-sensitive disease. Maca's "hormonally silent" mechanism is the contrast: no downstream serum hormone elevation, no corresponding contraindications, but also potentially smaller effect size for severe hormonal deficiency.
- Yohimbine — an alpha-2 adrenergic antagonist derived from the bark of Pausinystalia yohimbe. Yohimbine has historically been used for erectile dysfunction and reportedly for libido. Its mechanism is sympathomimetic and it carries cardiovascular and anxiety side effects (palpitations, hypertension, panic) that limit its clinical use. Maca is much better tolerated.
The summary positioning: Maca is a low-side-effect tonic best suited for the patient with mildly low libido and normal hormonal status, who wants an adjunctive intervention without committing to ongoing hormone therapy or a drug with stimulant-class side effects.
Practical Dose (1.5–3 g/day) and Black-Phenotype Selection
Across the controlled-trial literature, the consensus effective dose is 1.5 to 3 grams per day of dried Maca powder, taken as a single dose or split. The 2002 Gonzales men's trial found no dose-response advantage of 3 g over 1.5 g for libido, suggesting the lower dose is adequate for most users. The 2010 Dording women's trial found 3 g superior to 1.5 g for SSRI-induced sexual dysfunction specifically, so women in that context should start at the higher dose.
For the libido indication, the black phenotype has the strongest evidence and the highest measured macamide concentration. If the label does not specify color, the product is almost certainly predominantly yellow (the most common harvest fraction). For men specifically targeting libido or sperm parameters, source a single-origin black Maca from a reputable supplier and verify the color claim with the producer if possible.
Two preparation choices:
- Gelatinized vs. raw — gelatinized Maca has been gently heated to break down starches, improving digestibility and reducing the bloating that some users experience with raw powder. Gelatinization does not destroy macamides or glucosinolates at the temperatures used. Most clinical trials have used gelatinized; this is the default for most users.
- Powder vs. extract — whole-root powder mixes easily into smoothies, oatmeal, or yogurt. Capsule extracts are more convenient but typically require 6–10 capsules to reach the 3 g dose used in trials, and the cost per gram is higher. For chronic daily use, powder is more practical; for travel or convenience, capsules.
The libido effect is gradual. Trial endpoints have generally shown statistical significance at weeks 8 and 12, not earlier. A reasonable trial is 12 weeks at 1.5–3 g/day before judging whether the supplement works for the individual user. If there is no perceived effect at 12 weeks, discontinuation and exploration of an alternative is reasonable.
What to Expect — Realistic Effect Size and Timeline
The honest framing of Maca's libido effect, based on the controlled-trial literature, is:
- Effect size: small-to-moderate. On validated sexual function scales (ASEX, MGH-SFQ, IIEF), Maca produces effects roughly 30–50% of the magnitude of phosphodiesterase-5 inhibitors for erectile function, or roughly comparable to bupropion augmentation for SSRI-induced sexual dysfunction. This is a real signal, but it is not transformative.
- Onset timeline: 6–12 weeks of daily use. Maca does not produce an acute on-demand effect like a PDE5 inhibitor. Users expecting an immediate change after a single dose will be disappointed.
- Responder rate: in the trials, a clear majority of subjects show some improvement, but a meaningful minority (roughly 30–40% in most trial cohorts) show no detectable change. Individual variation is large and not currently predictable from biomarkers.
- Duration: effect persists as long as supplementation continues. The trial designs typically did not include long washout periods after discontinuation; anecdotally, the libido effect fades over 4–8 weeks after stopping Maca.
- Tolerance: tachyphylaxis (loss of effect with continued use) has not been documented in any of the published trials, but the trials are all relatively short (12 weeks to 6 months at most). Whether the libido effect persists at 1 year or 5 years of continuous use is not established.
For the patient who wants a low-side-effect adjunct to support sexual desire, with a realistic 60–70% probability of perceiving some benefit after 8–12 weeks of consistent use, Maca is a reasonable trial. For the patient seeking a dramatic or rapid sexual-function intervention, the conventional pharmaceuticals are the better-evidenced choice.
Cautions
- Thyroid: Maca is a cruciferous vegetable (Brassicaceae family) and contains goitrogenic glucosinolates that can theoretically interfere with thyroid iodine uptake. The amounts at typical 1.5–3 g/day dosing are very small — far less than a serving of broccoli or cabbage — and clinical hypothyroidism from Maca supplementation has not been reported. Patients with established hypothyroidism on levothyroxine replacement do not need to avoid Maca, but should take the levothyroxine and the Maca several hours apart and confirm stable TSH after starting Maca.
- Pregnancy and lactation: insufficient safety data. The traditional Andean use included Maca during pregnancy and lactation without reported harm, and the modern toxicology in animal studies has not identified developmental toxicity, but rigorous human pregnancy trials do not exist. Best practice is to defer Maca during pregnancy and lactation until better safety data are available, and to use it for fertility support only in the preconception period.
- Hormone-sensitive cancers: as discussed above, Maca does not bind sex hormone receptors and is not mechanistically contraindicated in hormone-sensitive disease. Patients on aromatase inhibitors, tamoxifen, GnRH agonists, or anti-androgens for cancer treatment should still discuss any new supplement with their oncology team before starting, but the conventional concern with phytoestrogens does not apply to Maca.
- Drug interactions: no major drug interactions have been documented in the clinical literature. The macamides may have weak CYP enzyme effects but no clinically significant interactions with common medications have been reported. SSRIs are explicitly co-administered with Maca in the Dording trial without adverse interaction.
- Mild gastrointestinal effects: bloating, mild gas, and loose stool are the most commonly reported side effects, primarily with raw (non-gelatinized) Maca powder. Switching to gelatinized typically resolves these.
- Allergic reactions: rare. Patients with documented allergy to other cruciferous vegetables (broccoli, cabbage, kale, mustard, horseradish) should approach Maca cautiously and start at a small test dose.
Key Research Papers
- Gonzales GF et al. (2002). Effect of Lepidium meyenii (MACA) on sexual desire and its absent relationship with serum testosterone levels in adult healthy men. Andrologia, 34(6):367-372. — PubMed
- Gonzales GF et al. (2001). Lepidium meyenii (Maca) improved semen parameters in adult men. Asian Journal of Andrology, 3(4):301-303. — PubMed
- Gonzales C et al. (2006). Effect of short-term and long-term treatments with three ecotypes of Lepidium meyenii (MACA) on spermatogenesis in rats. Journal of Ethnopharmacology, 103(3):448-454. — PubMed
- Shin BC, Lee MS, Yang EJ, Lim HS, Ernst E (2010). Maca (L. meyenii) for improving sexual function: a systematic review. BMC Complementary and Alternative Medicine, 10:44. — PubMed
- Dording CM et al. (2008). A double-blind, randomized, pilot dose-finding study of maca root (L. meyenii) for the management of SSRI-induced sexual dysfunction. CNS Neuroscience and Therapeutics, 14(3):182-191. — PubMed
- Zenico T et al. (2009). Subjective effects of Lepidium meyenii (Maca) extract on well-being and sexual performances in patients with mild erectile dysfunction: a randomised, double-blind clinical trial. Andrologia, 41(2):95-99. — PubMed
- Brooks NA et al. (2008). Beneficial effects of Lepidium meyenii (Maca) on psychological symptoms and measures of sexual dysfunction in postmenopausal women are not related to estrogen or androgen content. Menopause, 15(6):1157-1162. — PubMed
- Gonzales GF (2012). Ethnobiology and ethnopharmacology of Lepidium meyenii (Maca), a plant from the Peruvian highlands. Evidence-Based Complementary and Alternative Medicine, 2012:193496. — PubMed
- Hajdu Z et al. (2012). Identification of endocannabinoid system-modulating N-alkylamides from Heliopsis helianthoides var. scabra and Lepidium meyenii. Journal of Natural Products, 75(6):1080-1085. — PubMed
- Wu H et al. (2013). Macamides and their synthetic analogs: Evaluation of in vitro FAAH inhibition. Bioorganic and Medicinal Chemistry, 21(17):5188-5197. — PubMed
- Stone M et al. (2009). A pilot investigation into the effect of maca supplementation on physical activity and sexual desire in sportsmen. Journal of Ethnopharmacology, 126(3):574-576. — PubMed
- Lee MS et al. (2011). Maca (Lepidium meyenii) for treatment of menopausal symptoms: A systematic review. Maturitas, 70(3):227-233. — PubMed
PubMed Topic Searches
- PubMed: Maca and sexual desire / libido
- PubMed: Maca for SSRI-induced sexual dysfunction
- PubMed: Macamide endocannabinoid / FAAH
- PubMed: Maca sperm count and motility
- PubMed: Black Maca phenotype chemistry
Connections
- Maca Benefits Hub
- Maca Overview
- Maca for Hormonal Balance & Menopause
- Maca for Energy and Endurance
- Maca for Mood and Cognitive Function
- Ashwagandha
- Ginseng
- Rhodiola Rosea
- Testosterone Test
- Hormone Panel
- Zinc
- All Herbs