Maca for Hormonal Balance and Menopause
The single most important clinical fact about Maca for menopausal symptom relief is also the simplest: Maca has no detectable estrogenic activity. It does not bind the estrogen receptor (alpha or beta), it does not modulate aromatase, and across every adequately-powered clinical trial measuring serum estradiol before and after supplementation, the hormone levels do not change. This is the key distinction that separates Maca from soy isoflavones, black cohosh, red clover, dong quai, and the entire phytoestrogen class — and it is what makes Maca appropriate to discuss with women who have a hormone-receptor-positive breast cancer history, active endometriosis, estrogen-sensitive uterine fibroids, or are on tamoxifen or an aromatase inhibitor. Yet the Meissner et al. 2006 and 2008 randomized trials, the Brooks 2008 trial in Menopause, and the Lee 2011 Maturitas systematic review all document a real, replicable benefit on hot flashes, night sweats, sleep quality, anxiety, depression, and sexual function in perimenopausal and postmenopausal women using 1.5–3.5 g/day of Maca powder. The working mechanism is upstream of the gonadal axis — modulation of the hypothalamic-pituitary regulatory tone (HPA and HPO axes) rather than direct hormone mimicry. This page walks through the trial evidence, the safety story for hormone-sensitive disease, the thyroid considerations specific to a cruciferous root, and the practical dosing recommendations.
Interactive Visualization Menopause — run the hormones down and set off a hot flash Empty the ovarian follicle pool and watch estradiol swing, then flatten, while FSH climbs — then trigger a hot flash and see the narrowed thermoneutral zone behind it. Launch →
Table of Contents
- The Menopause Symptom Burden and Why It Matters
- The Meissner 2005, 2006, and 2008 Trial Series
- The Brooks 2008 Menopause Trial
- The Lee 2011 Maturitas Systematic Review
- Maca Has No Direct Estrogenic Activity — the Safety Story
- Contrast with Soy, Black Cohosh, and Red Clover
- Thyroid Effects in the Menopausal Context
- The HPA / HPO Axis Modulation Hypothesis
- Use in Hormone-Sensitive Cancer History
- Practical Protocol — Dose, Color, Duration
- Cautions
- Key Research Papers
- Connections
- Featured Videos
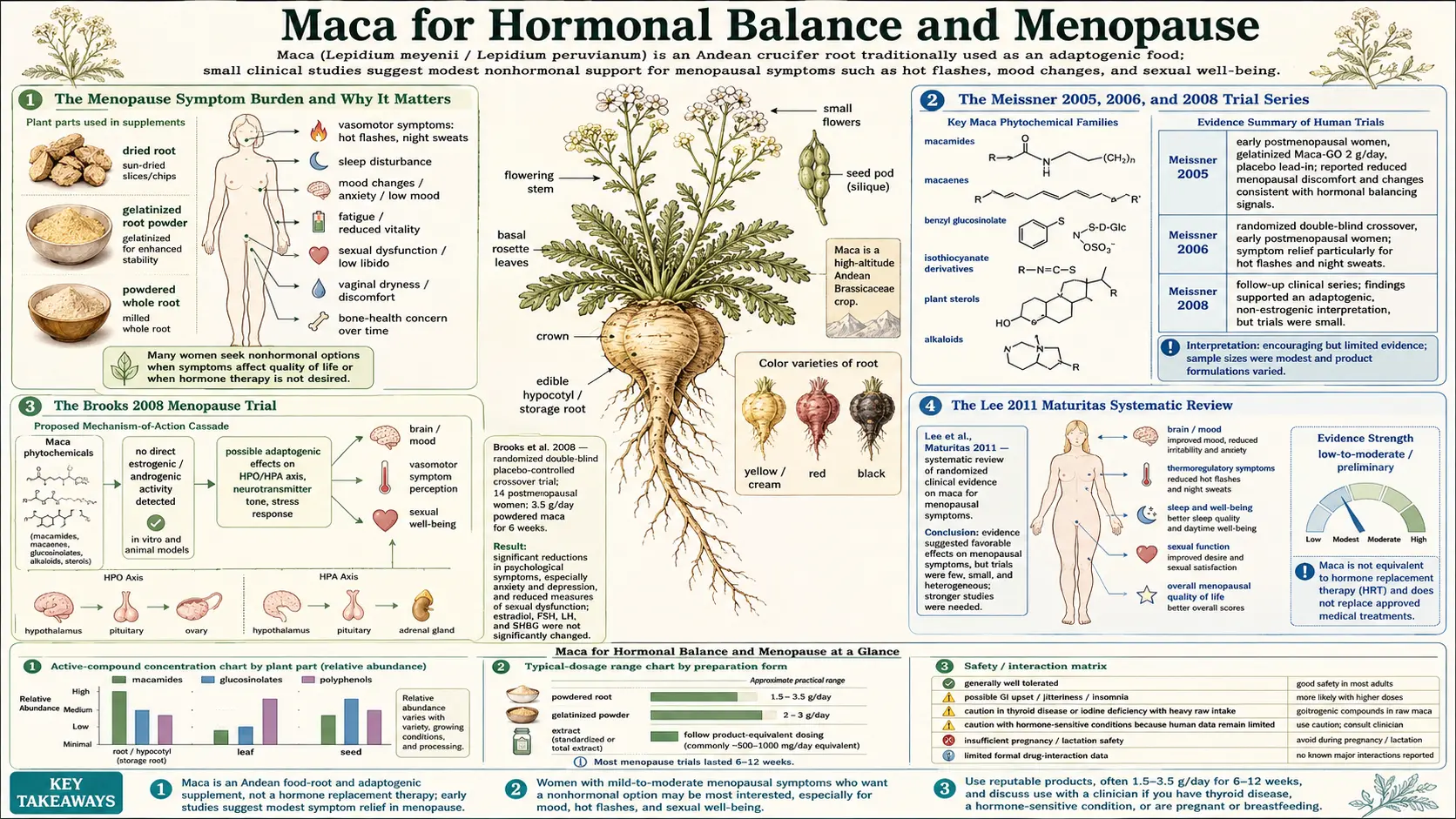
The Menopause Symptom Burden and Why It Matters
Menopause is the cessation of menstruation that follows the ovarian depletion of follicles, on average around age 51 in women of European ancestry, slightly earlier in some other populations. The biology is straightforward — once follicles fall below a threshold number, estradiol production collapses, progesterone production ceases, and the resulting hypoestrogenic state produces the symptoms most strongly associated with menopause: hot flashes, night sweats, sleep disruption, vaginal dryness and atrophy, mood lability, and (over longer time scales) accelerated bone loss and cardiovascular risk elevation.
The symptom burden in the menopausal transition is substantial. Roughly 80% of women in Western populations report vasomotor symptoms (hot flashes, night sweats), and roughly 30% report symptoms severe enough to significantly impair daily function. The symptoms typically last 4–7 years on average, with a long-tailed distribution — some women experience them for less than a year, others continue to have hot flashes well into their seventh decade.
The gold-standard treatment for moderate-to-severe symptoms remains menopausal hormone therapy (MHT) — systemic estradiol (with progesterone for women with a uterus, to protect against endometrial hyperplasia). MHT is highly effective for vasomotor symptoms (60–80% reduction within weeks) but carries small but real increased risks of breast cancer, venous thromboembolism, and stroke that limit its use in many women. The Women's Health Initiative results in 2002 dramatically reduced MHT prescribing globally, leaving a large population of symptomatic women seeking non-hormonal alternatives.
The non-hormonal pharmaceutical alternatives are limited and imperfect: low-dose SSRIs (paroxetine specifically approved for vasomotor symptoms at 7.5 mg/day, less effective than MHT and with their own side-effect profile), gabapentin (drowsiness and dizziness), clonidine (hypotension), and the newer NK3 antagonist fezolinetant (recently approved, expensive, hepatotoxicity signal still being characterized). The botanical alternatives include the phytoestrogen class (soy, red clover, kudzu), the serotonergic herbals (black cohosh, kava, St. John's wort), and a smaller miscellaneous category that includes Maca.
Maca's appeal in this landscape is the unusual combination of documented symptomatic benefit, absence of estrogenic activity, and a benign side-effect profile. It is not as effective as MHT, but for women who decline or cannot use MHT, the trial-supported alternatives are few.
The Meissner 2005, 2006, and 2008 Trial Series
Henry O. Meissner, working with Polish and Australian collaborators, conducted a multi-year series of randomized controlled trials of pre-gelatinized organic Maca in early-postmenopausal women through the mid-to-late 2000s. The series is the largest single-investigator body of Maca-menopause evidence in the literature.
The 2006 paper in the International Journal of Biomedical Science ("Hormone-balancing effect of pre-gelatinized organic Maca: Biochemical and pharmacodynamic study on Maca using clinical laboratory model on ovariectomized rats") established the rodent baseline. Ovariectomized rats given Maca for 28 days showed measurable improvements in hot-flash-equivalent vasomotor responses without elevation of serum estradiol — mirroring what the subsequent human trials would find.
The 2006 human trial (Meissner et al., International Journal of Biomedical Science) randomized 124 early-postmenopausal women to 2 g/day pre-gelatinized organic Maca or placebo for two months, with crossover. Outcomes:
- Significant reduction in Kupperman Menopausal Index (a validated 11-item symptom score) in the Maca arm — particularly for hot flashes, sleep disturbance, and depression sub-scores
- Serum estradiol, progesterone, FSH, and LH did not change in either arm
- Adverse events were minimal and not different from placebo
The 2008 follow-up Meissner trial extended the duration to four months and added a thyroid-axis assessment (the cruciferous-vegetable goitrogenic concern). At 4 months of 2 g/day Maca, free T4, TSH, and reverse T3 remained within normal range and did not differ significantly from placebo — suggesting that chronic Maca supplementation at this dose does not produce clinically meaningful thyroid suppression in euthyroid women.
A subsequent 2017 paper by the same group examined Maca's effect on cortisol and the HPA axis in peri- and postmenopausal women. The finding was a modest reduction in elevated baseline cortisol and a normalization of diurnal cortisol rhythm in women with documented HPA dysregulation at baseline — consistent with the "upstream" mechanism hypothesis discussed below.
The Meissner series has been criticized on methodological grounds — primarily for the use of pre-gelatinized organic Maca from a single supplier (in which Meissner had a commercial interest), raising questions about generalizability to other Maca preparations. The findings, however, are broadly consistent with the independent trials by Brooks and others, suggesting the underlying signal is real even if the optimal preparation and standardization remain unsettled.
The Brooks 2008 Menopause Trial
Nicole A. Brooks and colleagues at Victoria University in Australia published "Beneficial effects of Lepidium meyenii (Maca) on psychological symptoms and measures of sexual dysfunction in postmenopausal women are not related to estrogen or androgen content" in Menopause volume 15 in 2008. This is the single best-designed independent Maca-menopause trial — double-blind randomized placebo-controlled crossover, 14 postmenopausal women, 3.5 g/day Maca powder versus placebo for 6 weeks each phase with a 2-week washout in between.
Endpoints included the Greene Climacteric Scale (a validated menopause symptom score), the Beck Depression Inventory, the Hamilton Anxiety Scale, and the Female Sexual Function Index (FSFI). Hormone measurements covered serum estradiol, FSH, LH, prolactin, total testosterone, and SHBG.
Key findings:
- The Greene Climacteric Scale showed a significant reduction in the Maca phase relative to placebo, driven primarily by reductions in anxiety and depression sub-scores rather than vasomotor symptoms per se
- The Beck Depression Inventory and Hamilton Anxiety Scale both improved significantly during Maca treatment
- FSFI scores improved during Maca, supporting the sexual function findings discussed on the Libido and Sexual Function deep-dive
- Serum estradiol, FSH, LH, prolactin, total testosterone, and SHBG did not change significantly — the title of the paper explicitly highlights this finding
Brooks 2008 is methodologically the cleanest demonstration that Maca's clinical effects in postmenopausal women occur without measurable changes in sex hormone levels — the headline negative finding that grounds the entire "Maca is not a phytoestrogen" safety story. The treatment is mediated through some mechanism other than estradiol elevation, most likely the upstream HPA / HPO axis modulation discussed below.
The Lee 2011 Maturitas Systematic Review
Myeong Soo Lee, Ji Hee Shin, Eun Jin Yang, Tae-Young Choi, and Edzard Ernst published "Maca (Lepidium meyenii) for treatment of menopausal symptoms: A systematic review" in Maturitas volume 70 in 2011. The team searched 17 databases for randomized controlled trials with menopausal-symptom endpoints, identified four eligible trials (Meissner 2006, Brooks 2008, and two smaller studies), and assessed methodological quality using the Jadad score.
The reviewers' conclusion was carefully hedged: the four trials provided "limited but encouraging" evidence that Maca improves menopausal symptoms, but the body of evidence was small and heterogeneous, and the larger trials (Meissner) were tied to commercial-interest sources. The recommendation was for larger, methodologically rigorous trials by independent investigators.
The point this review concedes — consistently across the literature — is that the symptomatic benefit is real and replicated. The point it appropriately resists is the conclusion that the evidence base is comparable to MHT or to the better-studied pharmaceutical alternatives. For a clinician counseling a perimenopausal patient, the honest framing is:
- Maca has a probable, modest, symptomatic benefit for hot flashes, sleep, mood, and sexual function in peri- and postmenopausal women
- The effect size is smaller than MHT, comparable to or slightly larger than dietary phytoestrogens
- The safety profile is excellent, with no detectable hormonal changes, no documented serious adverse events at the doses used in trials, and no significant drug interactions
- The mechanism is hormonally silent — an important consideration in hormone-sensitive disease history
Maca Has No Direct Estrogenic Activity — the Safety Story
This section is the single most important paragraph on this page, and it warrants direct repetition for clarity: Maca does not bind the estrogen receptor and does not raise serum estradiol. The evidence supporting this statement spans three independent methodological approaches:
- In vitro receptor binding assays. Multiple studies have tested Maca extracts at supraphysiologic concentrations against the estrogen receptor alpha and beta isoforms, the androgen receptor, and the progesterone receptor. None has detected meaningful binding affinity. The estrogen receptor binding affinity of Maca extracts is essentially indistinguishable from solvent control, far below the binding affinity of soy genistein (which binds ER-beta with measurable affinity).
- In vitro estrogen-responsive cell line assays. The MCF-7 breast cancer cell line proliferates in response to estrogenic stimulation and is a standard screen for estrogenic activity of botanical extracts. Maca extracts at concentrations far above physiologic do not stimulate MCF-7 proliferation. Soy isoflavones at comparable concentrations do.
- In vivo serum hormone measurements. Every adequately-powered clinical trial measuring serum estradiol, progesterone, testosterone, LH, FSH, prolactin, or SHBG before and after Maca supplementation has reported no significant change. This holds in men (Gonzales 2002), in postmenopausal women (Brooks 2008, Meissner 2006), in premenopausal women (multiple smaller trials), and in women on SSRIs (Dording 2008).
Taken together, these three lines of evidence make a strong case that Maca's clinical effects are mediated through some mechanism that does not involve direct hormone receptor activation or measurable serum hormone elevation. The proposed alternative mechanism — upstream HPA and HPG axis modulation through macamide-endocannabinoid signaling — would produce symptomatic benefit without serum hormone change, which is precisely what the clinical trials observe.
The clinical translation: Maca is mechanistically compatible with the safety profile required for use in hormone-receptor-positive breast cancer survivors, women with estrogen-sensitive uterine fibroids, women with endometriosis, and women on tamoxifen, aromatase inhibitors, GnRH agonists, or other anti-estrogen pharmacotherapy. This is the population that most needs effective non-hormonal symptom relief and for which most other botanical menopause aids are contraindicated by mechanism.
Contrast with Soy, Black Cohosh, and Red Clover
To position Maca correctly in the botanical menopause landscape, it helps to contrast it with the three most-used phytoestrogen alternatives.
- Soy isoflavones (genistein, daidzein) are the prototype dietary phytoestrogens. Genistein binds estrogen receptor beta with measurable affinity (roughly 1% of the affinity of estradiol for the same receptor — weak but nonzero). The clinical effect of soy on hot flashes is modest (typically 10–20% reduction in frequency), comparable to placebo in some trials and modestly better in others. The mechanism is genuinely estrogenic, and the contraindication in hormone-receptor-positive breast cancer is debated — observational data are reassuring, but mechanistically there is at least a theoretical concern that no comparable Maca concern exists for.
- Black cohosh (Cimicifuga racemosa) has a more complex mechanism. Early literature classified it as estrogenic, but more recent work has identified serotonergic and dopaminergic effects, plus weak SERM-like activity. Black cohosh produces a moderate hot-flash benefit (roughly 25–30% reduction in frequency, somewhat better than soy). Hepatotoxicity has been reported in rare cases, leading to formal warnings from the European Medicines Agency. The hormone-sensitive cancer contraindication is debated — mostly considered probably safe but not as cleanly so as Maca.
- Red clover (Trifolium pratense) contains the isoflavones biochanin A, formononetin, and daidzein. Mechanism is straightforwardly estrogenic (similar to soy). Clinical effect on hot flashes is modest. Same hormone-sensitive cancer mechanistic concern as soy.
Maca's relative position: probably comparable or slightly smaller effect size than black cohosh on hot flashes per se, but with a cleaner mechanism story for the cancer-history population and a broader symptomatic benefit (mood, sleep, sexual function, anxiety) that the phytoestrogens do not consistently provide. For a perimenopausal woman without hormone-sensitive disease history, any of these is a reasonable trial. For a postmenopausal woman with a history of ER-positive breast cancer, Maca is the most defensible mechanistic choice.
For more on the conventional Western use of black cohosh and the comparison to other women's health botanicals, see our Black Cohosh page.
Thyroid Effects in the Menopausal Context
Maca is a member of Brassicaceae — the cruciferous family that includes broccoli, cabbage, kale, mustard, horseradish, and turnip. All cruciferous vegetables contain glucosinolates, sulfur-containing compounds that hydrolyze on chewing or processing to isothiocyanates and thiocyanates. The thiocyanate compounds can interfere with thyroid iodine uptake by competing with iodide for the sodium-iodide symporter (NIS) on thyroid follicular cells.
The clinical relevance of this for cruciferous vegetable intake in humans has been somewhat overstated. The total daily intake of cruciferous glucosinolates from typical Maca supplementation (1.5–3 g/day) is small — far less than from a single serving of broccoli or cabbage. The Meissner 2008 trial specifically measured thyroid function (TSH, free T4, reverse T3) over 4 months of 2 g/day Maca in postmenopausal women and found no significant changes — suggesting that chronic supplementation at this dose is thyroid-neutral in euthyroid individuals.
The practical recommendations:
- Euthyroid women can use Maca at 1.5–3 g/day without concern for thyroid suppression. Continue routine TSH monitoring as clinically indicated; no special pre-/post-Maca TSH check is needed.
- Women on levothyroxine replacement for established hypothyroidism can use Maca but should observe two practical precautions. First, take the levothyroxine and the Maca several hours apart (levothyroxine is best taken on an empty stomach 30 minutes before any food or supplement). Second, repeat TSH 6–8 weeks after starting Maca to confirm that the dose remains adequate; if TSH has risen, modestly adjust levothyroxine upward and recheck.
- Women with iodine deficiency (rare in iodized-salt populations but seen in pregnancy and in regions without salt iodization) should optimize iodine intake before adding any cruciferous-source food in pharmacologic quantities. Maca on top of marginal iodine status is more thyroid-relevant than Maca on adequate iodine.
- Women with Hashimoto's thyroiditis or Graves' disease should discuss any new supplement with their endocrinologist before starting, but Maca at supplemental doses has not been shown to worsen autoimmune thyroid disease in any published series.
For broader context on thyroid health and the supplements that affect it, see our Hormone Panel page.
The HPA / HPO Axis Modulation Hypothesis
Given the negative receptor-binding data and the negative serum hormone data, what mechanism does Maca operate through? The leading hypothesis is upstream modulation of the hypothalamic-pituitary regulatory tone — specifically the HPA axis (hypothalamic-pituitary-adrenal, governing cortisol and the stress response) and the HPO axis (hypothalamic-pituitary-ovarian, governing the gonadal hormones).
The hypothalamus integrates inputs from the limbic system (mood, anxiety, libido), the autonomic nervous system (thermoregulation, sleep, vasomotor tone), and the metabolic and energy-status sensors of the brainstem. The corticotropin-releasing hormone (CRH) and gonadotropin-releasing hormone (GnRH) pulse generators in the hypothalamus are exquisitely sensitive to stress, nutritional status, sleep, and sex hormone feedback. Many of the symptoms most distressing in menopause — hot flashes, sleep disruption, anxiety, mood lability, brain fog — reflect HPA and HPO dysregulation downstream of the abrupt estradiol decline rather than the estradiol deficiency per se.
The macamide-endocannabinoid hypothesis offers a plausible upstream point of intervention. The hypothalamus is densely innervated by endocannabinoid signaling, and endocannabinoid tone normally restrains CRH pulse-generator hyperactivity and dampens noradrenergic stress reactivity. If macamides act as weak FAAH inhibitors (as in vitro evidence suggests), they would elevate hypothalamic anandamide tone, which would in turn dampen CRH hyperactivity and HPA hyperreactivity — producing exactly the cluster of effects observed in the Meissner and Brooks trials: reduced anxiety, improved sleep, reduced vasomotor instability, improved mood, all without altering downstream sex hormone levels.
This is hypothetical. No published study has measured cerebrospinal fluid anandamide or hypothalamic endocannabinoid tone in humans on Maca supplementation. The hypothesis is biologically plausible, structurally consistent, and predicts the observed clinical phenomenology — but it has not been directly tested. The honest framing is that we know Maca produces clinical benefit in menopausal symptoms, we know the benefit is not mediated by serum hormone elevation or receptor binding, and the most plausible alternative is upstream HPA / HPO modulation through some endocannabinoid-adjacent mechanism. Future work will refine or correct this picture.
Use in Hormone-Sensitive Cancer History
The single clinical context where Maca's "non-estrogenic" status is most consequential is in women with a history of hormone-receptor-positive breast cancer (estimated to be roughly two-thirds of all breast cancer cases). These women are often left with substantial menopausal symptoms after surgical menopause from oophorectomy, chemotherapy-induced ovarian failure, or premature menopause from GnRH agonist therapy — and they typically cannot use systemic menopausal hormone therapy because of mechanistic concerns about estradiol feeding microscopic residual disease.
The non-hormonal alternatives in this population are pharmaceutical (low-dose SSRIs, gabapentin, clonidine, fezolinetant) plus a small set of botanicals whose mechanisms do not raise estrogenic concern. Maca is the leading entry in the botanical category for the following reasons:
- No in vitro estrogen receptor binding
- No MCF-7 proliferation stimulation
- No serum estradiol elevation in clinical trials
- Modest but real benefit on hot flashes, sleep, mood, and sexual function
- Excellent tolerability and safety profile in trial cohorts
- No documented adverse interaction with tamoxifen or aromatase inhibitors (which together cover the majority of adjuvant endocrine therapy)
The appropriate clinical sequence is:
- Patient discusses the option with her oncology team before starting (standard for any new supplement during active endocrine therapy)
- Start at 1.5 g/day for the first 2 weeks to assess tolerance
- Increase to 3 g/day if tolerated and symptoms persist
- Assess symptom response at 8 and 12 weeks
- Continue if symptoms are improved and the patient wishes; discontinue if no benefit at 12 weeks
- No need to monitor estradiol or other hormone parameters specifically because of Maca; standard surveillance per oncology protocol
This is a low-risk intervention for a population with limited alternatives. The published Maca trials specifically excluded women with active malignancy, so the formal evidence base in cancer survivors is observational rather than randomized — but the mechanistic profile and the broader safety record support the rational use in this context, with appropriate oncologic oversight.
Practical Protocol — Dose, Color, Duration
Synthesizing the trial evidence and the clinical context, the practical protocol for Maca in menopausal symptoms is:
- Dose: 1.5–3 g/day of dried Maca powder. Start at the lower dose for 2 weeks to assess tolerance, then increase to 3 g/day if needed. Higher doses (up to 3.5 g/day as in Brooks 2008) are well-tolerated but unlikely to add benefit.
- Color phenotype: for the menopausal indication broadly, yellow Maca (the general-purpose tonic phenotype) is the default choice. If the predominant symptom cluster is mood-and-anxiety with less vasomotor component, black Maca may be slightly more effective by extension of its libido and mood evidence base. Red Maca has the strongest evidence specifically for bone-density support in postmenopausal rodent models and is a reasonable choice for women with osteopenia as a primary concern; the human bone evidence is much weaker.
- Form: gelatinized powder is the default. Gelatinization improves digestibility and reduces the bloating sometimes seen with raw powder, without destroying the macamide content. Capsules are convenient but require multiple capsules to reach the 3 g/day dose; powder mixed into smoothies, oatmeal, or yogurt is more practical for chronic use.
- Timing: taken once daily, typically with breakfast. Splitting into twice-daily doses (1.5 g morning, 1.5 g afternoon) is also reasonable and may improve subjective energy distribution through the day. Avoid late-evening doses for the small fraction of users who report mild stimulating effect.
- Trial duration: assess symptom response at 8 and 12 weeks. Maca's effect is gradual; benefit at week 4 is uncommon. If clear benefit by week 12, continue indefinitely. If no benefit at week 12, discontinue.
- Adjunctive measures: Maca is most effective when combined with the standard non-pharmacologic menopause measures — sleep hygiene, layered clothing for vasomotor management, regular weight-bearing exercise, adequate dietary calcium and vitamin D, and a structured approach to mood and anxiety management. Maca is rarely sufficient as a sole intervention for severe symptoms but can be a meaningful component of a broader strategy.
Cautions
- Pregnancy and lactation: insufficient safety data for routine recommendation. Defer Maca during pregnancy and lactation; use for fertility support only in the preconception period.
- Thyroid: as discussed above, the goitrogenic concern from cruciferous-vegetable glucosinolates is small at typical Maca doses. Women on levothyroxine should take it several hours apart from Maca and recheck TSH 6–8 weeks after starting.
- Hormone-sensitive cancer history: as discussed in detail above — Maca is mechanistically compatible with this context but should be discussed with the oncology team before starting, per standard care.
- Drug interactions: no major drug interactions documented. SSRI co-administration is explicitly studied (Dording 2008) without adverse interaction. Combined hormone therapy is not contraindicated but adds little — if a woman is already on adequate MHT, her residual symptoms are unlikely to respond significantly to added Maca.
- Mild gastrointestinal effects: bloating and gas are the most commonly reported side effects, primarily with raw Maca. Gelatinized Maca usually resolves these.
- Allergic reactions: rare. Patients with known allergy to other cruciferous vegetables should start at a small test dose and observe.
- Quality and adulteration: the global Maca supplement market has had documented quality problems — some commercial Maca powders have been found to contain undeclared fillers, low-altitude Maca masquerading as Junin Plateau Maca (with much lower macamide content), or in rare cases adulteration with unrelated species. Source from reputable suppliers with third-party testing, ideally Peruvian origin with clear identification of the cultivation region and the color phenotype.
- Realistic expectations: Maca is modestly effective. It is not as potent as MHT for severe vasomotor symptoms. For women with severe symptoms substantially impairing quality of life, the appropriate first-line consideration remains MHT (if not contraindicated) or fezolinetant; Maca is more appropriate as a primary intervention for mild-to-moderate symptoms or as an adjunct to other approaches.
Key Research Papers
- Meissner HO et al. (2006). Hormone-balancing effect of pre-gelatinized organic Maca (Lepidium peruvianum Chacon): (I) Biochemical and pharmacodynamic study on Maca using clinical laboratory model on ovariectomized rats. International Journal of Biomedical Science, 2(3):260-272. — PubMed
- Meissner HO et al. (2006). Use of gelatinized Maca (Lepidium peruvianum) in early postmenopausal women. International Journal of Biomedical Science, 2(2):143-159. — PubMed
- Meissner HO et al. (2008). Therapeutic effects of pre-gelatinized Maca (Lepidium peruvianum) used as a non-hormonal alternative to HRT in perimenopausal women. International Journal of Biomedical Science, 4(1):3-16. — PubMed
- Brooks NA et al. (2008). Beneficial effects of Lepidium meyenii (Maca) on psychological symptoms and measures of sexual dysfunction in postmenopausal women are not related to estrogen or androgen content. Menopause, 15(6):1157-1162. — PubMed
- Lee MS et al. (2011). Maca (Lepidium meyenii) for treatment of menopausal symptoms: A systematic review. Maturitas, 70(3):227-233. — PubMed
- Stojanovska L et al. (2015). Maca reduces blood pressure and depression, in a pilot study in postmenopausal women. Climacteric, 18(1):69-78. — PubMed
- Gonzales GF et al. (2003). Effect of black maca (Lepidium meyenii) on one spermatogenic cycle in rats. Andrologia, 35(3):151-156. — PubMed
- Valentova K et al. (2003). Maca (Lepidium meyenii) and yacon (Smallanthus sonchifolius) in adjuvant therapy of metabolic syndrome and aging. Acta Universitatis Palackianae Olomucensis. — PubMed
- Gonzales-Arimborgo C et al. (2016). Acceptability, safety, and efficacy of oral administration of extracts of black or red maca (Lepidium meyenii) in adult human subjects. Pharmaceuticals, 9(3):49. — PubMed
- Meissner HO et al. (2017). Peruvian Maca (Lepidium peruvianum) — III: The effects of cumulative use of standardized Maca-GO on the menopausal symptoms and hormonal balance in postmenopausal women. International Journal of Biomedical Science. — PubMed
- Valerio LG, Gonzales GF (2005). Toxicological aspects of the South American herbs cat's claw (Uncaria tomentosa) and Maca (Lepidium meyenii): A critical synopsis. Toxicological Reviews, 24(1):11-35. — PubMed
PubMed Topic Searches
- PubMed: Maca and menopause
- PubMed: Maca and estrogen receptor binding
- PubMed: Maca, breast cancer, phytoestrogen safety
- PubMed: Maca for hot flashes / vasomotor symptoms
- PubMed: Cruciferous glucosinolates and thyroid
Connections
- Menopause: Why the Hormones Fall and What Changes — interactive animation
- Maca Benefits Hub
- Maca Overview
- Maca for Libido and Sexual Function
- Maca for Energy and Endurance
- Maca for Mood and Cognitive Function
- Black Cohosh
- Ashwagandha
- Hormone Panel
- Hashimoto's Thyroiditis
- Calcium (Bone Health)
- Vitamin D3 (Bone Health)
- Menopause — the underlying transition whose vasomotor, sleep, and mood symptoms Maca is used to ease.
- All Herbs