Licorice Cortisol & Hypertension Warning — Pseudoaldosteronism
THIS IS A SAFETY-CRITICAL PAGE
Pseudoaldosteronism (also called apparent mineralocorticoid excess, AME) from licorice consumption is the single most important adverse-effect syndrome of any herb in widespread popular use. It is a real, well-documented, life-threatening syndrome that has caused hospitalizations, intensive-care admissions, and deaths from cardiac arrhythmia secondary to severe hypokalemia. The FDA has issued a public-health warning that adults over 40 consuming as little as 2 ounces of black licorice candy per day for two weeks have triggered the syndrome. The European Union has set an upper limit of 100 mg of glycyrrhizin per day from food sources. Anyone using whole licorice or any glycyrrhizin-containing product must understand the mechanism, the warning signs, the contraindications, and the monitoring required. Deglycyrrhizinated licorice (DGL) does not produce this syndrome — the glycyrrhizin has been removed. Use DGL wherever GI applications are the indication and where any cardiovascular or renal risk factor is present.
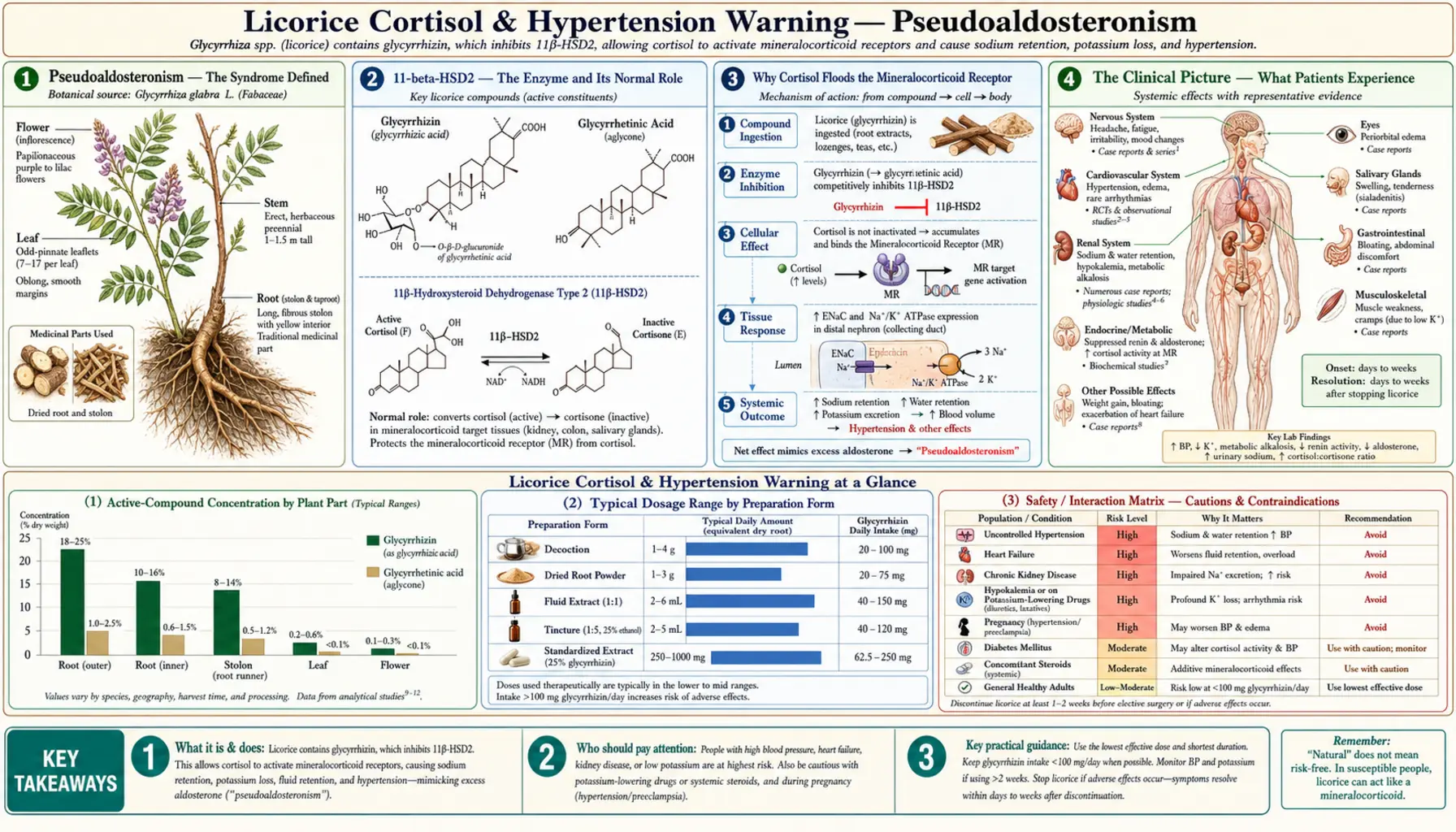
Glycyrrhizin (and its active metabolite glycyrrhetinic acid) inhibits 11-beta-hydroxysteroid dehydrogenase type 2 (11-beta-HSD2) in the renal collecting tubule. The normal function of this enzyme is to inactivate cortisol locally, preventing cortisol from inappropriately activating the mineralocorticoid receptor (which has approximately equal binding affinity for cortisol and aldosterone but is normally protected from cortisol by 11-beta-HSD2). When licorice blocks this enzyme, circulating cortisol — present at roughly 100-fold higher concentration than aldosterone — floods the unprotected mineralocorticoid receptor and triggers the same downstream cascade as primary aldosteronism: sodium and water retention, potassium and hydrogen excretion. The clinical result is hypertension (often severe), hypokalemia (often severe enough to cause muscle weakness, paralysis, rhabdomyolysis, or cardiac arrhythmia), metabolic alkalosis, edema, and suppressed renin and aldosterone (because the body interprets the mineralocorticoid excess and shuts down the renin-angiotensin-aldosterone axis). The syndrome is fully reversible on discontinuation of licorice, but resolution can take weeks. This page covers the mechanism in detail, the case literature, the regulatory warnings, every contraindication, and the safe-use envelope for therapeutic whole licorice.
Table of Contents
- Pseudoaldosteronism — The Syndrome Defined
- 11-beta-HSD2 — The Enzyme and Its Normal Role
- Why Cortisol Floods the Mineralocorticoid Receptor
- The Clinical Picture — What Patients Experience
- The Case Report Literature
- The FDA Black Licorice Candy Warning
- The European 100 mg/day Glycyrrhizin Upper Limit
- Hidden Sources of Glycyrrhizin in the Food Supply
- Dose-Response and Individual Variation
- Absolute Contraindications
- Relative Contraindications and Drug Interactions
- Monitoring Protocol for Therapeutic Use
- Management of Licorice-Induced Toxicity
- Why DGL Bypasses the Entire Risk
- Pregnancy and Lactation
- Pediatric Considerations
- Key Research Papers
- Connections
- Featured Videos
Pseudoaldosteronism — The Syndrome Defined
Pseudoaldosteronism is a state in which the kidney behaves as if there is excess aldosterone signaling, even though circulating aldosterone is actually low or normal. The syndrome was first formally described in the medical literature in the late 1960s as a recognized complication of carbenoxolone therapy (the synthetic glycyrrhetinic acid derivative used for peptic ulcers), and was extended to whole licorice and licorice candy in subsequent case series.
The defining biochemical features:
- Hypertension — often moderate-to-severe; can develop rapidly (within 1-2 weeks of high licorice intake) or insidiously over months of moderate intake
- Hypokalemia — serum potassium typically <3.5 mmol/L, can fall below 2.5 mmol/L in severe cases
- Hypernatremia — usually mild; sodium retention dominates over water retention
- Metabolic alkalosis — from urinary hydrogen-ion loss; serum bicarbonate >30 mmol/L
- Suppressed plasma renin activity — the renin-angiotensin-aldosterone system shuts down in response to the apparent mineralocorticoid excess
- Suppressed serum aldosterone — same reason
- Edema — particularly facial puffiness and ankle swelling; can be the presenting complaint
- Weight gain — 2-5 kg of fluid retention in the first 1-2 weeks of significant exposure
The syndrome is biochemically identical to apparent mineralocorticoid excess (AME), the rare congenital deficiency of 11-beta-HSD2 in which children are born with the same renal phenotype. The 1987 Stewart Lancet paper, "Mineralocorticoid activity of liquorice: 11-beta-hydroxysteroid dehydrogenase deficiency comes of age," explicitly linked the two and provided the mechanistic understanding that unified the inherited deficiency, the acquired form from licorice, and the carbenoxolone iatrogenic form into a single pathophysiologic framework.
The danger of pseudoaldosteronism is not the hypertension per se (which is treatable) but the hypokalemia. Severe hypokalemia (K <2.5 mmol/L) produces predictable cardiac instability: prolonged QT interval, U waves, T wave flattening, frequent premature ventricular contractions, and risk of torsades de pointes or ventricular fibrillation. Death from licorice-induced hypokalemic cardiac arrhythmia is rare but documented.
11-beta-HSD2 — The Enzyme and Its Normal Role
11-beta-hydroxysteroid dehydrogenase type 2 (11-beta-HSD2) is a NAD+-dependent enzyme expressed primarily in the principal cells of the renal cortical collecting duct, with additional expression in placenta, colon, and sweat glands. Its catalytic function is the oxidation of the 11-beta-hydroxyl group of cortisol to a keto group, producing cortisone — the inactive 11-keto form. Cortisone does not bind the mineralocorticoid receptor and does not bind the glucocorticoid receptor effectively. Cortisol is biologically active; cortisone is not.
This is a pre-receptor metabolic gating mechanism. The mineralocorticoid receptor has roughly equal binding affinity for aldosterone and cortisol. Aldosterone circulates at low concentrations (typically 50-150 pg/mL) under tight regulation by the renin-angiotensin system. Cortisol circulates at much higher concentrations (typically 50-250 ng/mL, roughly 1,000-fold higher in mass terms and even higher in molar terms). Without 11-beta-HSD2 inactivating cortisol locally at the renal tubule, cortisol would always dominate at the mineralocorticoid receptor and produce constant mineralocorticoid signaling regardless of aldosterone status.
11-beta-HSD2 is therefore a clever evolutionary solution: the enzyme is co-expressed with the mineralocorticoid receptor in target tissues, inactivating cortisol at the cell surface before it can bind the receptor. The unbound aldosterone then has clear access to the receptor and drives appropriate physiologic mineralocorticoid signaling (sodium retention, potassium excretion) under renin-angiotensin control. This is sometimes called the "pre-receptor specificity" mechanism.
When the enzyme is inhibited — whether genetically (congenital 11-beta-HSD2 deficiency, also called AME), pharmacologically (glycyrrhizin, carbenoxolone), or rarely by competitive inhibition from other steroids — the pre-receptor specificity collapses. Cortisol now reaches the mineralocorticoid receptor in much greater amounts than aldosterone does, and the receptor is essentially saturated with cortisol-driven signaling. The biochemical and clinical picture is indistinguishable from primary aldosteronism (Conn syndrome), except that aldosterone levels are low (suppressed by the apparent excess), not high.
Why Cortisol Floods the Mineralocorticoid Receptor
To understand the magnitude of the problem when 11-beta-HSD2 is blocked, the molar arithmetic helps. Aldosterone circulates at approximately 0.1-0.5 nM in the bloodstream. Cortisol circulates at approximately 150-700 nM in the bloodstream — roughly 1,000-fold higher molar concentration. At the mineralocorticoid receptor, the binding affinities are similar (aldosterone has a slightly higher affinity by a factor of ~2-3, not 1,000). Mass action therefore predicts that without 11-beta-HSD2, cortisol would occupy the receptor several hundred-fold more frequently than aldosterone, producing maximal mineralocorticoid signaling continuously.
This is exactly what happens in licorice-induced pseudoaldosteronism. Even at partial 11-beta-HSD2 inhibition (50% enzyme blockade is enough to produce clinical effects in many patients), the local cortisol-to-active-aldosterone ratio at the renal tubule shifts dramatically in favor of cortisol. The mineralocorticoid receptor sees what it interprets as massive aldosterone exposure and signals accordingly: sodium reabsorption, water reabsorption, potassium secretion, hydrogen-ion secretion.
The downstream physiologic effects:
- Increased blood pressure — from sodium and water retention expanding blood volume; from vascular smooth-muscle effects of mineralocorticoid signaling that increase peripheral resistance
- Hypokalemia — from urinary potassium loss as the principal cell sodium-potassium exchange is upregulated
- Metabolic alkalosis — from urinary hydrogen-ion loss in parallel with potassium loss
- Suppression of the renin-angiotensin-aldosterone system — the body senses the apparent mineralocorticoid excess and shuts down endogenous aldosterone production. Plasma renin activity falls. Serum aldosterone falls. This is paradoxical because the patient looks biochemically like primary aldosteronism but has the lowest possible aldosterone level — it is "apparent" mineralocorticoid excess driven by cortisol.
The patient with severe licorice-induced pseudoaldosteronism has the renal phenotype of a Conn syndrome patient with the aldosterone profile of an Addison's patient. This combination is essentially never seen except in 11-beta-HSD2 deficiency syndromes — congenital AME or its acquired licorice-induced form.
The Clinical Picture — What Patients Experience
Most patients with mild-to-moderate licorice-induced pseudoaldosteronism are asymptomatic and the syndrome is detected only by routine monitoring (blood pressure check, serum potassium check). The symptomatic forms typically present with a combination of:
- Hypertension symptoms — headache (often morning), facial flushing, occasional vision changes, palpitations
- Hypokalemia symptoms — muscle weakness (often proximal, particularly thigh and shoulder girdle), muscle cramps, fatigue, exercise intolerance, sometimes leg paralysis at potassium <2.5 mmol/L
- Fluid retention symptoms — facial puffiness (particularly around the eyes on waking), ankle swelling, sudden weight gain (2-5 kg in a few weeks without dietary change), rings becoming tight on fingers
- Severe cases — flaccid paralysis (the dramatic hypokalemic paralysis presentation), cardiac arrhythmia, rhabdomyolysis with dark urine and elevated CK, hypertensive crisis
The most diagnostic feature is the temporal association with licorice intake. A patient who develops new-onset hypertension, hypokalemia, or facial edema in the weeks following a substantial increase in licorice candy consumption, licorice tea consumption, herbal-supplement use, or shisha/hookah smoking (some shisha tobacco contains licorice) should prompt the question. Many published case reports involve the patient denying licorice consumption initially, only to recall on direct questioning a recent shift to large amounts of black licorice candy, an herbal tea blend containing licorice (some "throat coat" or "stomach soothing" teas), or a multi-herb supplement that includes licorice in the ingredient list.
The Case Report Literature
The medical literature contains hundreds of published case reports of licorice-induced pseudoaldosteronism from sources including:
- Black licorice candy — the most common identifiable trigger in case reports. Doses associated with toxicity range from approximately 50 g/day for several weeks (in sensitive individuals) to several hundred grams/day for a few weeks (in less sensitive individuals).
- Licorice tea — commercial "throat coat," "stomach soothing," and "adrenal support" tea blends often contain licorice as a primary ingredient. Heavy consumption (5-10 cups daily) of strong licorice tea can produce the syndrome.
- Herbal multi-supplement preparations — Chinese medicine formulas containing licorice (gan cao) as a harmonizer, Western herbal blends for adrenal support, women's reproductive support formulas containing licorice for phytoestrogen content
- Carbenoxolone — the synthetic ulcer drug, when it was still in widespread use, was a major source of iatrogenic pseudoaldosteronism in the 1960s-1970s
- Glycyrrhizin-flavored chewing tobacco and shisha — less commonly recognized but documented
- Licorice-flavored alcoholic beverages — certain herbal liqueurs (Sambuca, Pastis, Ouzo, Jagermeister) contain anise, which is flavor-similar but does not contain glycyrrhizin; true licorice-containing beverages are rare but exist
Several notable case reports illustrate the range:
- A 70-year-old woman developed severe hypertension (200/120), hypokalemia (K 2.1), and lower-extremity weakness after several weeks of eating one bag of black licorice candy daily. Required ICU admission for potassium replacement. Full recovery over 6 weeks after licorice cessation.
- A 54-year-old man died from cardiac arrhythmia. Postmortem investigation revealed severe hypokalemia and a history of consuming approximately a pound and a half of black licorice candy per week for several years.
- A 45-year-old woman on routine antihypertensive medication developed worsening BP control after starting a daily licorice tea regimen for "adrenal support." Discontinuation of the tea restored prior BP control without medication change.
- Multiple case reports of pediatric pseudoaldosteronism in children who ate large quantities of black licorice candy — children appear to be more sensitive per kg of body weight.
- Case series from Italy and Greece, where licorice is more commonly used in traditional food preparations, document chronic low-level pseudoaldosteronism in healthy adults that resolved with dietary modification.
The case literature is consistent on three points: (a) the syndrome is real and reproducible, (b) the doses required to produce clinically significant disease are within reach of ordinary consumption patterns (not just medicinal use), and (c) the toxicity is fully reversible on discontinuation but resolution can take weeks.
The FDA Black Licorice Candy Warning
In October 2017, the U.S. Food and Drug Administration issued a public-health advisory titled "Black Licorice: Trick or Treat?" warning consumers about the cardiac risks of black licorice candy. The advisory specifically stated that "if you're 40 or older, eating 2 ounces of black licorice a day for at least two weeks could land you in the hospital with an irregular heart rhythm or arrhythmia." The advisory was prompted by the FDA's receipt of a report of a fatal case of cardiac arrhythmia in an adult consuming large quantities of black licorice.
The FDA noted several key points:
- Glycyrrhizin is the active compound in real black licorice candy (the candy made from Glycyrrhiza glabra extract, as distinct from anise-flavored candy that may be called "licorice" but contains no glycyrrhizin)
- Eating large amounts of black licorice candy can cause potassium levels in the body to fall, which can lead to abnormal heart rhythms, high blood pressure, edema, lethargy, and congestive heart failure
- Older adults (40+) appear to be at higher risk for the cardiac complications
- Stopping black licorice intake produces resolution of the abnormal potassium levels, usually within hours to days, with full clinical recovery over weeks
- Consumers should consult a healthcare provider if eating black licorice has caused irregular heart rhythm or muscle weakness
The FDA does not require warning labels on black licorice candy products and does not regulate glycyrrhizin content in food. The advisory was educational rather than regulatory. Consumers in the U.S. should read ingredient labels: products containing "licorice extract" or "licorice root" likely contain glycyrrhizin, while products containing only "natural flavor" or "anise" likely do not.
The European 100 mg/day Glycyrrhizin Upper Limit
The European Commission's Scientific Committee on Food (SCF) reviewed the safety of glycyrrhizin in 2003 and concluded that habitual intake should not exceed 100 mg of glycyrrhizin per day from food sources. This recommendation has been adopted by the European Food Safety Authority (EFSA) and forms the basis of food labeling requirements in EU member states for products containing licorice extract.
The 100 mg/day threshold was set based on:
- Pharmacokinetic studies showing that 100 mg of glycyrrhizin per day produces measurable cortisol-prolongation and partial 11-beta-HSD2 inhibition in healthy adults
- The lowest-observed-adverse-effect level (LOAEL) for clinically detectable mineralocorticoid effects in human volunteer studies
- An additional safety factor for sensitive subpopulations (older adults, women, those with renal disease)
For reference, 100 mg of glycyrrhizin corresponds approximately to:
- 50-100 g of black licorice candy per day (varies widely by brand)
- 1-2 cups of strong licorice tea per day
- 500-1500 mg of standardized whole-root extract (depending on the glycyrrhizin content of the extract, typically 4-12%)
- A daily dose of many multi-herb formulas containing licorice as a co-ingredient
European licorice candy products are required to carry warning labels: products with 4-50 mg glycyrrhizin per 100 g must indicate "contains liquorice"; products with >50 mg per 100 g must indicate "contains liquorice — people suffering from hypertension should avoid excessive consumption." This is more stringent than the U.S. labeling regime.
Hidden Sources of Glycyrrhizin in the Food Supply
Patients who develop unexplained pseudoaldosteronism sometimes report no obvious licorice consumption, but careful dietary history reveals one or more hidden sources:
- Herbal teas marketed for other purposes — "throat coat," "stomach soothe," "adrenal support," "menopausal balance," "pregnancy tea," and many other branded herbal teas contain licorice as a primary or secondary ingredient. Heavy daily consumption of these can deliver substantial glycyrrhizin.
- Multi-ingredient supplement formulas — many adrenal-support, women's-hormone, immune-support, and Chinese-medicine combination products contain licorice. Always read the full ingredient list, not just the front label.
- "Sugar-free" or "natural sweetener" products — glycyrrhizin's 50-fold sweetness over sucrose makes it a natural choice for sugar-reduction formulations. Some specialty candies, baked goods, and confections marketed as low-sugar use glycyrrhizin as a sweetener.
- Chewing gum and breath mints — some brands include licorice extract for flavor or for purported breath benefits
- Chewing tobacco and pipe tobacco — licorice has long been used as a flavoring and humectant in tobacco products
- Shisha (hookah tobacco) — some shisha flavorings contain licorice
- Pharmaceutical excipients — rarely, licorice extract is used as a flavoring agent in pediatric liquid medications to mask bitter active ingredients
- Beer — certain craft beers and traditional European beer styles (some Belgian and Czech beers) include licorice root in the brewing process
For the patient with unexplained hypokalemia, hypertension, or edema, the question "do you consume anything that might contain licorice?" deserves a careful exploration of all the categories above before concluding that the source is something else.
Dose-Response and Individual Variation
Individual sensitivity to glycyrrhizin-induced pseudoaldosteronism varies substantially — estimates from human volunteer studies suggest a range of approximately 10-fold between the most sensitive and least sensitive healthy adults. Factors that increase sensitivity:
- Age >40 — older adults appear more sensitive, possibly due to age-related decline in 11-beta-HSD2 expression baseline
- Female sex — women appear slightly more sensitive than men at equivalent doses, possibly due to estrogen effects on 11-beta-HSD2
- Lower body weight — smaller individuals receive proportionally larger per-kg doses for the same intake
- Preexisting hypertension — the additional sodium retention adds to baseline volume status
- Renal disease — reduced kidney function reduces the kidney's ability to compensate for the mineralocorticoid signaling
- Concurrent potassium-wasting drugs — loop and thiazide diuretics produce additive hypokalemia
- Low dietary potassium — chronically low potassium intake reduces the buffer against acute potassium loss
- High dietary sodium — amplifies the volume-expansion effect
The lowest documented dose to produce clinical pseudoaldosteronism in a sensitive adult is approximately 100 mg of glycyrrhizin per day for 2 weeks. The threshold dose for the average healthy adult is closer to 400-600 mg of glycyrrhizin per day. Persons consuming >1 g of glycyrrhizin per day chronically will almost universally develop the syndrome within 4-12 weeks.
The variability means that no single "safe daily dose" can be guaranteed for any individual. The conservative practice for therapeutic whole-licorice use is the European-derived 100 mg/day ceiling, time-limited, with monitoring.
Absolute Contraindications
The following are absolute contraindications to whole licorice or any glycyrrhizin-containing preparation. DGL is acceptable in all of these.
- Uncontrolled hypertension — any patient with BP consistently >140/90 not at goal on current medication. Licorice will antagonize antihypertensive therapy and worsen control.
- Congestive heart failure (any class) — the sodium and fluid retention will precipitate or worsen decompensation
- Hypokalemia at baseline (K <3.8) — the kaliuretic effect will deepen the hypokalemia
- Chronic kidney disease (eGFR <45) — reduced ability to handle sodium and potassium loads
- Cirrhosis with ascites — the additional sodium retention will worsen ascites and hepatorenal syndrome risk
- Cushing's syndrome of any cause — the patient is already hypercortisolemic; adding cortisol prolongation is contraindicated
- Primary aldosteronism (Conn syndrome) — mineralocorticoid excess is already present
- Pregnancy — substantial epidemiologic evidence (Finnish cohort) links high pregnancy licorice intake to preterm delivery, lower birth weight, and altered offspring cortisol regulation, cognitive function, and behavior years later. Avoid >100 mg glycyrrhizin per week during pregnancy.
- Breastfeeding — glycyrrhizin is excreted in breast milk and can produce neonatal effects
- Concurrent digoxin therapy — hypokalemia potentiates digoxin toxicity at therapeutic digoxin levels, with risk of fatal arrhythmia
- Concurrent potassium-wasting diuretics (loop or thiazide) — additive hypokalemia
- Hypokalemic periodic paralysis or other channelopathies — baseline hypokalemic sensitivity
- Long QT syndrome — hypokalemia further prolongs QT and increases torsades risk
Relative Contraindications and Drug Interactions
The following deserve clinical caution and individual risk-benefit assessment:
- Stable controlled hypertension on antihypertensive medication — licorice will antagonize the medication effect; either avoid licorice or monitor BP carefully and titrate medication if needed
- Concurrent oral corticosteroids (prednisone, hydrocortisone) — licorice prolongs the activity of the exogenous corticosteroid as well as endogenous cortisol, potentially producing iatrogenic hypercortisolism
- Warfarin or other anticoagulants — CYP-mediated interactions can alter anticoagulant metabolism and INR control
- Oral contraceptives — mixed reports of altered contraceptive metabolism; consider backup contraception during therapeutic licorice use
- Methadone and other CYP3A4 substrates — licorice inhibits CYP3A4, increasing methadone exposure with risk of respiratory depression
- Statins (simvastatin, atorvastatin) — CYP3A4 inhibition can elevate statin levels with risk of myopathy
- Diabetes (type 1 or 2) — cortisol prolongation worsens hyperglycemia; monitor blood glucose
- Hypothyroidism on thyroid replacement — glycyrrhizin affects thyroid hormone metabolism; monitor TSH
- Erectile dysfunction — chronic high-dose licorice has been associated with reduced testosterone in some men
Monitoring Protocol for Therapeutic Use
For the patient using whole licorice therapeutically (under clinical supervision, with no absolute contraindications, for a specific indication, time-limited):
- Baseline assessment
- Home blood pressure measurements for 1 week before starting (establishes baseline)
- Serum electrolytes (sodium, potassium, chloride, bicarbonate, creatinine, eGFR)
- Aldosterone and renin levels (optional, for the rare case where Conn syndrome needs to be excluded)
- EKG if any cardiac history
- Initial monitoring (first 4 weeks)
- Daily home BP for the first 2 weeks, then twice weekly
- Serum electrolytes at 2 weeks and 4 weeks
- Daily weight check; flag >1 kg gain in any 3-day window
- Symptom check: facial puffiness, ankle swelling, muscle weakness, palpitations, headache
- Maintenance monitoring (weeks 4-12)
- Weekly home BP
- Serum electrolytes monthly
- Weekly weight check
- Discontinuation triggers
- Systolic BP rise >15 mmHg above baseline
- Any BP reading >160/100
- Serum potassium <3.5
- Weight gain >2 kg in 2 weeks
- New-onset edema, palpitations, or muscle weakness
- Any cardiac arrhythmia on EKG
The monitoring effort may seem disproportionate to the herb's reputation as a "gentle" botanical, but the case literature is unambiguous: pseudoaldosteronism is silent until it crosses into the cardiac-arrhythmia range. The lab value is the only reliable warning shot. Skipping the monitoring is the most common factor in catastrophic outcomes.
Management of Licorice-Induced Toxicity
When pseudoaldosteronism is identified, management depends on severity:
- Mild (asymptomatic, K 3.5-3.8, BP modestly elevated) — discontinue licorice. Increase dietary potassium (banana, orange juice, leafy greens, potato). Re-check electrolytes and BP in 1-2 weeks; both should normalize.
- Moderate (mild symptoms, K 3.0-3.5, BP >160 systolic) — discontinue licorice. Oral potassium replacement 40-60 mEq daily. BP medication adjustment if needed. Outpatient follow-up at 1 week.
- Severe (K <3.0, hypertensive urgency, edema, weakness) — emergency department or hospital admission. IV potassium replacement (carefully, with EKG monitoring), continuous cardiac monitoring, BP control with appropriate IV agents. Spironolactone (a mineralocorticoid receptor blocker) is the mechanistically targeted therapy and can be added; it blocks the cortisol-mediated mineralocorticoid signaling pharmacologically.
- Life-threatening (cardiac arrhythmia, paralysis) — ICU admission, advanced cardiac life support if needed, IV potassium replacement, spironolactone. Recovery is expected with discontinuation but the patient may require days of intensive monitoring.
The biochemical recovery timeline:
- Plasma glycyrrhetinic acid clears within 24-48 hours of discontinuation
- Potassium begins to normalize within 1-2 days with appropriate replacement
- Blood pressure normalizes over 1-2 weeks as fluid volume reverts
- Renin and aldosterone suppression resolves over 4-8 weeks
- Full recovery of the renin-angiotensin-aldosterone axis takes up to 12 weeks in long-exposed patients
The patient must understand that recurrence on re-exposure is essentially guaranteed and that lifelong avoidance of licorice and licorice candy is appropriate after a significant pseudoaldosteronism episode.
Why DGL Bypasses the Entire Risk
Deglycyrrhizinated licorice (DGL) is whole-root licorice from which the glycyrrhizin has been removed by solvent extraction. The standard product contains less than 3 mg of residual glycyrrhizin per dose, well below the pharmacologic threshold for 11-beta-HSD2 inhibition. Because glycyrrhizin is the constituent responsible for the entire pseudoaldosteronism syndrome — the cortisol prolongation, the mineralocorticoid receptor flooding, the sodium retention, the potassium loss, the hypertension, the cardiac arrhythmia risk — removing glycyrrhizin eliminates the entire safety problem.
The DGL flavonoid fraction (liquiritin, liquiritigenin, isoliquiritigenin, glabridin) does not affect 11-beta-HSD2 and does not bind the mineralocorticoid receptor. Patients with absolute contraindications to whole licorice (hypertension, heart failure, diuretic users, pregnancy, etc.) can use DGL safely at the standard 380-760 mg per dose for the standard GI indications.
The clinical bottom line is straightforward: for GI indications, always start with DGL. There is no GI indication for which whole licorice is preferable to DGL. Whole licorice is reserved for indications where the glycyrrhizin-mediated effects are explicitly desired (cortisol prolongation for documented hypocortisolism; high-dose antiviral therapy), where contraindications are absent, and where appropriate monitoring is in place.
Pregnancy and Lactation
The Finnish prospective cohort studies (Raikkonen et al., subsequent follow-up papers over 20 years) are the strongest pregnancy-licorice data in the human literature. The cohort, recruited in Finland in 1998 (where licorice is a popular snack and many pregnancies have substantial licorice exposure), tracked maternal licorice intake during pregnancy and followed the offspring through adolescence. Key findings:
- High maternal licorice intake during pregnancy (defined as >500 mg of glycyrrhizin per week) was associated with shorter gestational age and modestly lower birth weight
- Offspring of high-licorice mothers showed altered HPA-axis reactivity at age 8 and again at age 12-13 — specifically, elevated salivary cortisol response to stress
- Offspring showed measurably poorer performance on cognitive tests (verbal IQ, narrative memory) at age 8
- Offspring showed higher rates of attention problems and aggressive behavior on parent-reported behavioral scales
- Female offspring of high-licorice mothers reached menarche earlier than offspring of low-licorice mothers
The Finnish data are observational, not interventional, but the associations are robust across multiple outcomes and persist after adjustment for potential confounders. The proposed mechanism is glycyrrhizin-mediated inhibition of placental 11-beta-HSD2, exposing the developing fetus to higher levels of maternal cortisol than would otherwise reach fetal circulation. Glucocorticoid exposure in utero is known from animal models to program lifelong HPA axis abnormalities, and the human Finnish data are consistent with that mechanism.
Practical guidance: pregnant women should avoid whole licorice and licorice candy. DGL is presumably safer (no glycyrrhizin) but lacks formal pregnancy trial data, so conservative practice limits DGL during pregnancy to short-course symptomatic use rather than chronic high-dose therapy. Breastfeeding women should avoid whole licorice; glycyrrhizin and glycyrrhetinic acid are excreted in breast milk.
Pediatric Considerations
Children appear more sensitive to glycyrrhizin per kg of body weight than adults. Several case reports document pseudoaldosteronism in children who consumed substantial quantities of black licorice candy — in some cases, just a few weeks of daily candy bag consumption is enough to produce clinically significant hypokalemia and hypertension. The smaller body size means smaller absolute glycyrrhizin loads produce proportionally larger pharmacologic effects.
Whole licorice is generally not indicated in pediatric practice. The principal therapeutic indications (cortisol prolongation, high-dose antiviral therapy) do not commonly arise in children. DGL has been used in pediatric reflux and gastritis without reported safety concerns, though formal pediatric dosing studies are sparse. Conservative pediatric practice would limit DGL to specific indications, in age-appropriate doses, after standard medical evaluation.
Parents should be aware that black licorice candy is genuinely dangerous in childhood in large quantities. The "candy candy" perception understates the pharmacology — a 30-kg child eating a 100-g bag of black licorice candy is receiving a glycyrrhizin dose comparable to a therapeutic adult licorice extract dose. Children with cardiac, renal, or hypertension history should avoid black licorice candy entirely.
Key Research Papers
- Stewart PM et al. (1987). Mineralocorticoid activity of liquorice: 11-beta-hydroxysteroid dehydrogenase deficiency comes of age. The Lancet 2(8563):821-4. — PubMed
- Walker BR & Edwards CR (1994). Licorice-induced hypertension and syndromes of apparent mineralocorticoid excess. Endocrinology and Metabolism Clinics of North America. — PubMed
- FDA Consumer Update (2017). Black Licorice: Trick or Treat? — PubMed: FDA warning
- Omar HR et al. (2012). Licorice abuse: time to send a warning message. Therapeutic Advances in Endocrinology and Metabolism. — PubMed
- Raikkonen K et al. (2017). Maternal liquorice consumption during pregnancy and pubertal, cognitive, and psychiatric outcomes in children. American Journal of Epidemiology. — PubMed
- Raikkonen K et al. (2010). Maternal licorice consumption and detrimental cognitive and psychiatric outcomes in children. American Journal of Epidemiology. — PubMed
- Sigurjonsdottir HA et al. (2001). Liquorice-induced rise in blood pressure: a linear dose-response relationship. Journal of Human Hypertension. — PubMed
- Olukoga A & Donaldson D (2000). Liquorice and its health implications. Journal of the Royal Society for the Promotion of Health. — PubMed
- Edwards CR (1991). Lessons from licorice. New England Journal of Medicine. — PubMed
- Hammer F & Stewart PM (2006). Cortisol metabolism in hypertension. Best Practice & Research Clinical Endocrinology & Metabolism. — PubMed
- Eriksson JW et al. (1999). Life-threatening ventricular tachycardia due to liquorice-induced hypokalaemia. Journal of Internal Medicine. — PubMed
- Brouwers AJ & van der Meulen J (2001). "Licorice hypertension" also caused by licorice tea. Nederlands Tijdschrift voor Geneeskunde. — PubMed
- Allcock E & Cowdery J (2015). Hypertension induced by liquorice tea. BMJ Case Reports. — PubMed
- Ottenbacher R & Blehar D (2015). Licorice-induced hypokalemia: a case report and review of pathophysiology. Journal of Emergency Medicine. — PubMed
PubMed Topic Searches
- PubMed: Licorice pseudoaldosteronism
- PubMed: Glycyrrhizin and 11-beta-HSD2
- PubMed: Licorice hypokalemia and arrhythmia
- PubMed: Licorice pregnancy outcomes
- PubMed: Apparent mineralocorticoid excess
Connections
- Licorice Overview
- Licorice Benefits Hub
- Adrenal Support and Cortisol
- GI Health and Ulcers (DGL)
- Antiviral Activity
- Hypertension
- Cardiac Arrhythmia
- Potassium
- Sodium
- Cortisol Test
- Electrolyte Panel
- Cushing's Syndrome
- Hyperaldosteronism (Conn Syndrome)
- Chronic Kidney Disease
- Heart Failure
- Pregnancy
- Adrenal Support
- Food Additives