Licorice Antiviral Activity (Glycyrrhizin)
Glycyrrhizin (and its active metabolite glycyrrhetinic acid) has documented in vitro and in vivo antiviral activity against a wide range of enveloped DNA and RNA viruses — herpes simplex virus (HSV-1, HSV-2), Epstein-Barr virus (EBV), cytomegalovirus (CMV), hepatitis B virus (HBV), hepatitis C virus (HCV), and, historically notable, the original SARS coronavirus in the 2003 outbreak. In Japan, an intravenous glycyrrhizin preparation (Stronger Neo-Minophagen C) has been used in chronic viral hepatitis since the 1970s with documented reductions in liver enzyme elevation and long-term reductions in hepatocellular carcinoma incidence in chronic HCV patients. Topical glycyrrhetinic acid is in widespread cosmetic and over-the-counter use for recurrent labial herpes (cold sores). Oral whole licorice does not reach the systemic glycyrrhizin levels of intravenous preparations and its clinical antiviral effect at oral doses is more modest, but it remains a useful adjunct in integrative protocols for chronic viral infections, particularly chronic EBV reactivation syndromes and chronic hepatitis maintenance. This page covers the mechanism, the major virus families, the pivotal trials (Crance 2003 hepatitis, Cinatl 2003 SARS), and the practical use of glycyrrhizin in modern integrative care.
Table of Contents
- The Antiviral Mechanism — How Glycyrrhizin Works
- The Enveloped-Virus Spectrum
- Herpes Simplex Virus (HSV-1 and HSV-2)
- Topical Glycyrrhetinic Acid for Cold Sores
- Epstein-Barr Virus and Chronic Reactivation
- Cytomegalovirus (CMV)
- Hepatitis B and C — The Crance 2003 HCV Work
- Stronger Neo-Minophagen C — Japan's 50-Year Hepatitis Protocol
- The Cinatl 2003 Lancet SARS Paper — Historical Context
- HIV Pilot Data and Adjunct Use
- Oral vs Intravenous Glycyrrhizin — Why Bioavailability Matters
- Clinical Protocols for Chronic Viral Conditions
- Key Research Papers
- Connections
- Featured Videos
The Antiviral Mechanism — How Glycyrrhizin Works
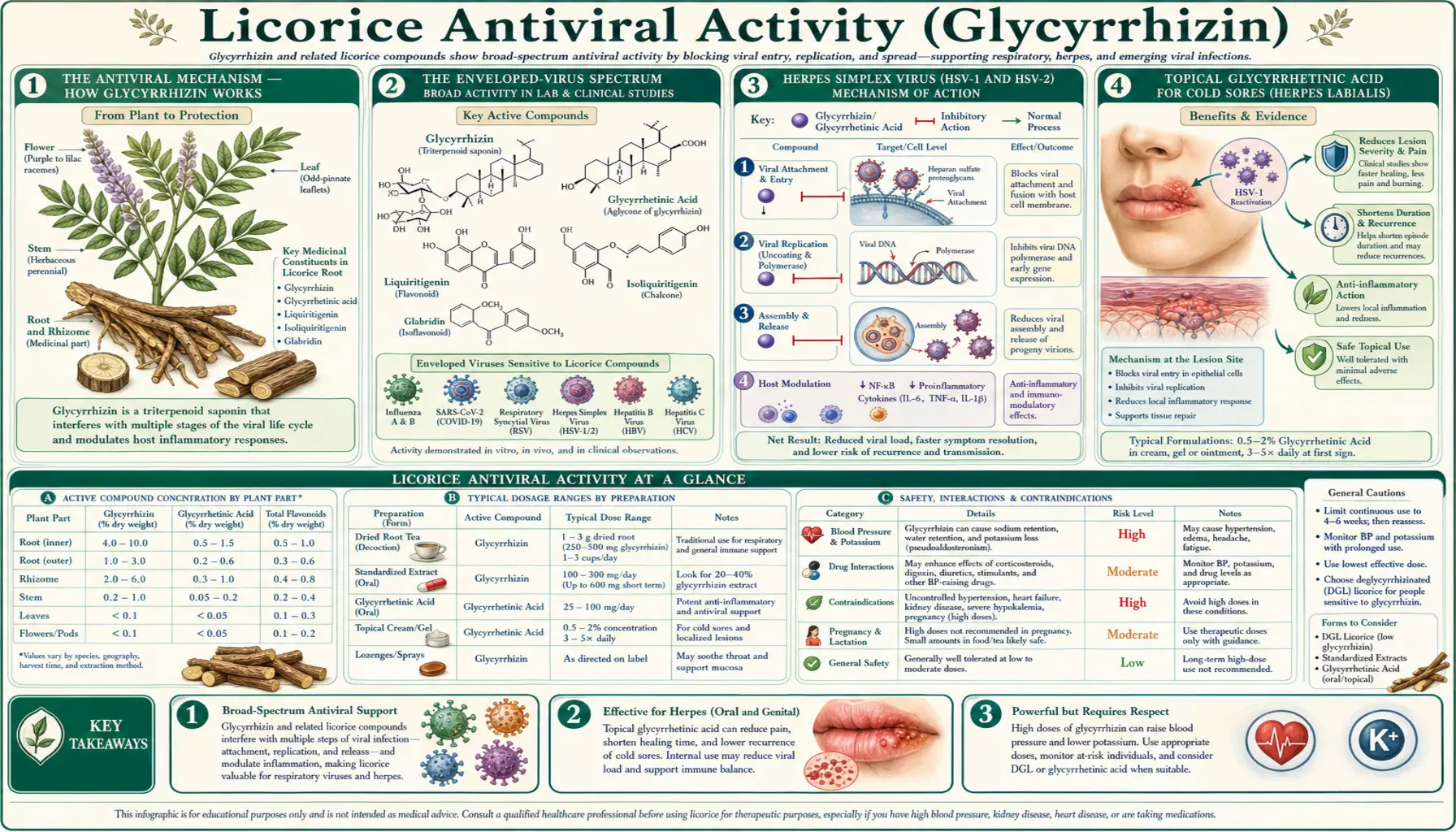
Glycyrrhizin appears to disrupt viral replication through multiple parallel mechanisms, which collectively explain its activity against an unusually broad range of enveloped viruses. The mechanisms identified to date:
- Inhibition of viral entry and membrane fusion — glycyrrhizin disrupts the lipid bilayer of enveloped virions and interferes with the conformational changes in viral fusion proteins that are required for the virus to enter the host cell. This step appears to be one of the most reliable mechanisms and is implicated in activity against HSV, HCV, HBV, and SARS coronavirus.
- Inhibition of viral protein synthesis — in established infections, glycyrrhizin reduces the production of viral structural and non-structural proteins, slowing the production of new virions and shifting the host-virus equilibrium in favor of the host immune response.
- Modulation of host signaling — glycyrrhizin upregulates host interferon production (particularly IFN-gamma) and modulates the NF-kappa-B pathway in ways that enhance antiviral innate immunity. This is a host-directed rather than direct-acting antiviral mechanism.
- Inhibition of viral replication enzymes — for some viruses (HCV in particular), glycyrrhizin shows weak inhibitory activity against viral polymerases and proteases at high concentrations.
- Reduction of latency reactivation — in chronic herpesvirus infections (HSV, EBV, CMV), glycyrrhizin appears to reduce the rate of reactivation from latency, possibly by interfering with the viral transcription factors that initiate the reactivation cascade.
The combined effect explains the unusual breadth of antiviral activity. Glycyrrhizin is not as potent as direct-acting antivirals (acyclovir, oseltamivir, sofosbuvir, the COVID protease inhibitors) against any single virus, but it produces detectable activity against many viruses and acts at multiple steps in the viral lifecycle, which makes resistance development unlikely. The pharmacological profile is that of a broad-spectrum, modest-potency, host-supportive antiviral — useful as adjunct, not as primary therapy for acute serious viral disease.
The Enveloped-Virus Spectrum
Glycyrrhizin's activity is concentrated on enveloped viruses — viruses that acquire a lipid bilayer envelope from the host cell membrane during budding. The list includes most herpesviruses, hepatitis B, hepatitis C, HIV, influenza, RSV, coronaviruses, and many others. Non-enveloped viruses (poliovirus, rotavirus, norovirus, adenovirus, papillomaviruses) are generally less affected, because the mechanisms that target the lipid envelope are not available.
Within the enveloped-virus category, the activity is most reliably documented for:
- Herpesviruses — HSV-1 (oral herpes), HSV-2 (genital herpes), VZV (varicella, shingles), EBV (mononucleosis, lymphoma), CMV (congenital infection, transplant reactivation), HHV-6 (roseola, possible chronic fatigue association), HHV-8 (Kaposi sarcoma)
- Hepatitis viruses — HBV (chronic hepatitis B), HCV (chronic hepatitis C)
- Retroviruses — HIV (mixed evidence, small effect)
- Coronaviruses — SARS-CoV (the original 2003 SARS, documented in Cinatl 2003 Lancet)
- Respiratory viruses — influenza A in animal models, RSV in cell culture
This page covers herpesviruses, hepatitis viruses, and SARS in detail. The other applications are less well-documented and not central to current integrative use of licorice.
Herpes Simplex Virus (HSV-1 and HSV-2)
Herpes simplex viruses establish lifelong latent infection in sensory ganglia after primary infection, with periodic reactivation producing the recognizable mucocutaneous lesions — cold sores (HSV-1 most commonly) or genital herpes (HSV-2 most commonly, with HSV-1 increasingly causing genital disease as well). Standard pharmacologic management uses nucleoside analog antivirals (acyclovir, valacyclovir, famciclovir) for acute outbreaks and chronic suppression.
Glycyrrhizin has documented in vitro activity against both HSV-1 and HSV-2, with EC50 values in the low-micromolar range. The mechanism appears to involve interference with the viral fusion step and possibly inhibition of viral immediate-early gene expression that drives reactivation from latency. In animal models of recurrent ocular HSV-1 keratitis, topical glycyrrhizin reduced reactivation frequency and lesion severity.
The clinical translation has been most successful for topical applications (see next section). For systemic management of recurrent labial or genital herpes, oral whole licorice has been used as an adjunct in integrative protocols at doses of 75-150 mg of glycyrrhizin per day, but the evidence for clinical benefit at these doses is anecdotal rather than trial-based. Patients with frequent outbreaks (>6 per year for labial, >4-6 per year for genital) should be on chronic acyclovir or valacyclovir suppression as primary management, with licorice as adjunct only.
Topical Glycyrrhetinic Acid for Cold Sores
Topical glycyrrhetinic acid is one of the most widely used over-the-counter botanical antivirals globally, found in dozens of branded cold-sore products in Europe and Asia. The typical preparation is a 1-2% glycyrrhetinic acid cream or gel, applied at the first sign of tingling or prodromal symptoms and continued 4-5 times daily until the lesion fully heals.
Randomized controlled trials of topical glycyrrhetinic acid for recurrent labial herpes have shown:
- Reduced lesion duration (typically 1-2 days shorter than placebo)
- Reduced lesion size at peak
- Faster pain resolution
- Reduced rate of vesicle formation if applied very early (prodrome stage)
- Excellent local tolerability (no irritation, no systemic absorption at clinically meaningful levels)
The effect size is modest but real, comparable to topical acyclovir cream (5%) and somewhat less than oral valacyclovir taken at prodrome. For patients with infrequent cold sores who prefer not to use prescription antivirals, topical glycyrrhetinic acid is a reasonable first-line option. For patients with frequent or severe outbreaks, oral valacyclovir is more effective and should be the primary therapy.
An interesting practical note: dabbing whole licorice extract or even DGL paste (DGL powder mixed with a few drops of water) directly on an early cold sore is a folk remedy with the same theoretical rationale and many anecdotal reports of efficacy. The DGL paste lacks the standardized glycyrrhetinic acid concentration of commercial topical products and is unlikely to be as consistently effective, but in a pinch it represents the same active class.
Epstein-Barr Virus and Chronic Reactivation
Epstein-Barr virus (EBV) infects roughly 95% of adults worldwide. Primary infection in adolescence or young adulthood causes infectious mononucleosis; primary infection in childhood is typically asymptomatic. After primary infection, EBV establishes lifelong latency in memory B cells. Chronic active EBV (CAEBV) and chronic EBV reactivation syndromes are increasingly recognized as contributors to chronic fatigue, autoimmune disease (multiple sclerosis, lupus, rheumatoid arthritis), and several lymphoproliferative malignancies.
Glycyrrhizin has documented anti-EBV activity in cell culture, with reduction of viral DNA replication and reduction of viral antigen expression. The mechanism is similar to its anti-HSV activity, with the additional consideration that EBV-driven B cell proliferation is also reduced by glycyrrhizin's anti-inflammatory and immune-modulating effects.
The clinical evidence for licorice in chronic active EBV is suggestive but limited. Integrative-medicine practitioners working with chronic fatigue and post-viral fatigue patients often include licorice (typically whole-root extract at 100-300 mg standardized to glycyrrhizin) as part of multi-herb antiviral protocols that also include monolaurin, lysine, lemon balm, and olive leaf extract. The evidence for the combined protocol is anecdotal-to-case-series in quality. For patients with documented chronic EBV reactivation (positive EBV early antigen antibody, elevated viral loads), this approach is reasonable as adjunct alongside standard medical evaluation.
For more on the chronic fatigue and post-viral fatigue context, see our Chronic Fatigue page.
Cytomegalovirus (CMV)
Cytomegalovirus is another ubiquitous herpesvirus (50-90% seroprevalence depending on geography and socioeconomics) that establishes lifelong latency and can reactivate in immunocompromised hosts — particularly transplant recipients, late-stage HIV patients, and chemotherapy patients. Primary CMV in pregnancy is a leading cause of congenital infection. Glycyrrhizin has documented activity against CMV in cell culture, with EC50 values comparable to those for HSV.
The clinical use of glycyrrhizin in CMV is limited but interesting. In Japan, intravenous glycyrrhizin (Stronger Neo-Minophagen C, see below) has been used as adjunct in CMV hepatitis in immunocompromised hosts when ganciclovir resistance or toxicity is a problem. The evidence is case-series quality but supports the broad-spectrum antiviral activity of the molecule.
For most clinical scenarios where CMV is the issue (transplant prophylaxis, AIDS-associated CMV retinitis), licorice is not relevant therapy; ganciclovir, valganciclovir, foscarnet, and letermovir are the appropriate drugs. Licorice may have a small adjunct role in immunocompetent CMV-mononucleosis syndromes, where the clinical picture is closer to EBV mononucleosis and supportive antiviral effects are useful but specific antiviral therapy is not indicated.
Hepatitis B and C — The Crance 2003 HCV Work
Chronic viral hepatitis (HBV and HCV) is the most-studied indication for therapeutic glycyrrhizin, with decades of Japanese clinical experience and a respectable in-vitro literature. The Crance JM et al. 2003 paper in Antiviral Research is one of the most-cited mechanistic papers in this area. Crance and colleagues compared the in-vitro activity of interferon-alpha, ribavirin, 6-azauridine, and glycyrrhizin against hepatitis A and hepatitis C viruses in cultured hepatocyte models.
Key findings:
- Glycyrrhizin produced dose-dependent reduction in HCV core antigen expression at concentrations achievable with intravenous (but not oral) administration in humans
- The activity appeared to derive primarily from inhibition of viral entry and inhibition of HCV replication, not from direct inhibition of viral polymerase
- Combination with interferon-alpha produced additive (not synergistic) effects
- Activity was not dependent on the cortisol-related 11-beta-HSD2 mechanism — this is a separate molecular action of glycyrrhizin
The Crance work supported the long-running Japanese clinical experience with intravenous glycyrrhizin in chronic HCV, which had documented reductions in liver enzyme elevation, possible reductions in long-term liver fibrosis, and most importantly a reduction in hepatocellular carcinoma incidence in long-term chronic HCV patients on chronic glycyrrhizin therapy. With the arrival of direct-acting antivirals (sofosbuvir-based regimens) for HCV in the 2010s, the role of glycyrrhizin in HCV management has shrunk dramatically — HCV is now curable in >95% of patients with 8-12 weeks of well-tolerated oral antivirals, and there is no reason to use glycyrrhizin as primary therapy. Glycyrrhizin retains a small role for the rare patient who has failed direct-acting antiviral therapy or who has contraindications to it.
For HBV, glycyrrhizin shows similar in-vitro activity but the clinical evidence base is smaller. The mainstays of HBV therapy remain tenofovir, entecavir, and pegylated interferon; glycyrrhizin has only an adjunct role at most.
Stronger Neo-Minophagen C — Japan's 50-Year Hepatitis Protocol
Stronger Neo-Minophagen C (SNMC) is an intravenous preparation containing 0.2% glycyrrhizin, 0.1% cysteine, and 2.0% glycine, developed in Japan in the 1950s for liver disease and used continuously since. The cysteine and glycine are added to the formulation primarily to mitigate the mineralocorticoid effects of the glycyrrhizin (the rationale is partly empirical, partly based on amino-acid metabolism in the liver), though the mineralocorticoid effects are not fully eliminated and SNMC patients still require blood pressure and potassium monitoring.
The standard SNMC protocol for chronic hepatitis is 40-100 mL daily by slow IV infusion, 5 days per week, for an extended period (months to years in some patients). Documented effects:
- Sustained reductions in serum ALT and AST elevations (the conventional surrogate for liver inflammation)
- Modest reductions in viral load in chronic HBV and HCV (smaller than direct-acting antivirals)
- In a long-term Japanese cohort, reduced incidence of hepatocellular carcinoma in chronic HCV patients on chronic SNMC compared to historical controls
- Reduced incidence of liver fibrosis progression on serial biopsy
- Generally well-tolerated when monitored, with the principal adverse effect being the predicted mineralocorticoid syndrome (hypokalemia, hypertension, edema) in some patients requiring dose adjustment
SNMC remains in active use in Japan and several Asian countries, primarily for patients with chronic HBV (for which direct-acting cures do not yet exist), for HCV patients who failed or could not tolerate direct-acting antivirals, and for non-viral chronic liver disease (alcoholic liver disease, nonalcoholic steatohepatitis, autoimmune hepatitis). Outside Japan it is rarely used; the closest Western equivalent is oral glycyrrhizin extract preparations at high dose, which do not approach the systemic glycyrrhizin exposure of SNMC but provide a partial substitute.
The SNMC experience is the strongest single piece of evidence for glycyrrhizin's genuine antiviral activity in human disease. The decades-long clinical record, with serial biopsies and long-term outcome data, is much more substantial than any equivalent natural-product clinical experience in Western pharmacology.
The Cinatl 2003 Lancet SARS Paper — Historical Context
In June 2003, in the immediate aftermath of the original SARS coronavirus outbreak (SARS-CoV, distinct from the much later SARS-CoV-2 of 2019-2023), Jindrich Cinatl and colleagues published a Lancet letter titled "Glycyrrhizin, an active component of liquorice roots, and replication of SARS-associated coronavirus." The work was rapid and limited — an in-vitro screen comparing the antiviral activity of glycyrrhizin, ribavirin, 6-azauridine, pyrazofurin, and mycophenolic acid against two clinical isolates of the SARS coronavirus in Vero cell culture.
The finding was striking: glycyrrhizin produced the lowest EC50 of any of the compounds tested, with a measured EC50 of approximately 300 mg/L and a clear selectivity index favorable for therapeutic use. The mechanism appeared to involve inhibition of viral replication and viral adsorption to host cells. The authors explicitly suggested that further clinical investigation of glycyrrhizin in SARS patients would be warranted.
The 2003 SARS outbreak was contained primarily by public-health measures (case isolation, quarantine, contact tracing) before any antiviral therapy was tested in randomized trials. SARS-CoV essentially disappeared by mid-2004. Glycyrrhizin was never formally trialed in SARS patients. The Cinatl paper remained a curious historical footnote — an early example of natural-product screening in a novel respiratory virus outbreak — until the 2019-2023 SARS-CoV-2 pandemic produced renewed interest in the question of whether glycyrrhizin had analogous activity against the new coronavirus.
Per the site's editorial policy, this page does not discuss SARS-CoV-2 or COVID-19. The historical SARS-CoV (2003) discussion is included because it is part of the long-standing scientific record of glycyrrhizin's antiviral activity and predates the much more politicized later coronavirus context. The 2003 in-vitro signal informs the general antiviral mechanism discussion but does not by itself support any specific clinical recommendation.
HIV Pilot Data and Adjunct Use
Glycyrrhizin and HIV is a small but interesting literature. The earliest work in the 1980s and 1990s showed in-vitro inhibition of HIV-1 replication in cultured T cells at concentrations achievable with intravenous SNMC, and several small clinical case series from Japan reported sustained CD4 count stability or improvement in chronic HIV patients on long-term IV glycyrrhizin. The mechanism appeared to involve interference with reverse transcriptase activity at high glycyrrhizin concentrations and possibly with viral entry through gp120-CD4 interactions.
The arrival of effective combination antiretroviral therapy (the protease-inhibitor breakthrough of 1996 and subsequent integrase-inhibitor era) made glycyrrhizin clinically irrelevant as primary HIV therapy — the small reductions in viral activity from glycyrrhizin are dwarfed by the multi-log reductions achievable with modern ART. Glycyrrhizin retains a possible adjunct role in two scenarios: chronic-hepatitis-coinfected HIV patients (where the liver-protective effects are theoretically useful) and patients on long-term ART who have stable virologic suppression but ongoing immune activation (a population in whom anti-inflammatory adjuncts are an area of clinical research).
The 1990s positive Japanese clinical reports have not been independently replicated in modern trials and would not by themselves support recommending glycyrrhizin in HIV care today. The CART era has settled the primary therapy question definitively.
Oral vs Intravenous Glycyrrhizin — Why Bioavailability Matters
The single most important practical limitation on oral whole licorice as an antiviral is bioavailability. Glycyrrhizin is poorly absorbed from the intestine in its native form (5-10% oral bioavailability) and undergoes substantial first-pass metabolism in the liver to glycyrrhetinic acid, which is more bioavailable but has different pharmacological activity. Peak plasma concentrations of glycyrrhizin after oral administration are typically in the low micromolar range — below the concentrations at which significant in-vitro antiviral activity is observed for most viruses.
Intravenous glycyrrhizin (SNMC) bypasses this bioavailability limitation entirely and reliably achieves the high-micromolar plasma concentrations needed for measurable antiviral activity. This is why the strongest clinical evidence for glycyrrhizin antiviral effect comes from the Japanese SNMC experience — the route of administration is doing critical pharmacological work that oral preparations cannot match.
For the patient using oral whole licorice as an integrative antiviral, this means realistic expectations: modest, supportive, host-directed effects are plausible; direct potent antiviral effects comparable to oseltamivir or valacyclovir are not. The oral antiviral activity is more about supporting the host's own antiviral response (innate immunity modulation, mucosal IgA support, anti-inflammatory action) than about reaching virion-killing concentrations in tissue. This framing helps explain why oral licorice shows benefit in some chronic indolent viral conditions (chronic EBV reactivation, chronic hepatitis maintenance) but is rarely the right answer for acute severe viral illness.
Clinical Protocols for Chronic Viral Conditions
- Recurrent labial herpes (cold sores) — topical 1-2% glycyrrhetinic acid cream applied 4-5× daily at first prodrome, continued until lesion heals. May be combined with oral lysine (1 g 3× daily) and topical melissa officinalis (lemon balm). For frequent outbreaks, oral valacyclovir suppression is more effective and should be considered.
- Chronic EBV reactivation — standardized whole-root licorice extract 100-300 mg twice daily (delivering ~75-150 mg glycyrrhizin per day), combined with monolaurin, lysine, and lemon balm. Time-limited to 8-12 weeks at therapeutic dose with subsequent break or DGL substitution. Requires blood pressure and potassium monitoring per safety page.
- Chronic hepatitis B or C maintenance (post-eradication or eradication-ineligible) — under hepatology supervision only. Oral high-dose glycyrrhizin preparations or, where available, IV SNMC protocols. Not a substitute for direct-acting antivirals when those are indicated.
- Genital herpes outbreaks — oral valacyclovir or acyclovir is the standard of care. Licorice has at most an adjunct role and should not delay appropriate antiviral therapy.
- Generic adjunct antiviral support during cold/flu season — DGL chewables daily (for the gut-mucosal IgA support) plus episodic short-course whole licorice extract during active illness; combined with elderberry, zinc, and vitamin D.
For all chronic uses of whole licorice, the safety constraints outlined on the Cortisol and Hypertension Warning page apply — the antiviral indication does not waive the mineralocorticoid risk profile.
Key Research Papers
- Cinatl J et al. (2003). Glycyrrhizin, an active component of liquorice roots, and replication of SARS-associated coronavirus. The Lancet 361(9374):2045-46. — PubMed
- Crance JM et al. (2003). Interferon, ribavirin, 6-azauridine and glycyrrhizin: antiviral compounds active against pathogenic flaviviruses. Antiviral Research 58(1):73-79. — PubMed
- Pompei R et al. (1979). Glycyrrhizic acid inhibits virus growth and inactivates virus particles. Nature 281:689-690. — PubMed
- Arase Y et al. (1997). The long-term efficacy of glycyrrhizin in chronic hepatitis C patients. Cancer 79(8):1494-1500. — PubMed
- van Rossum TG et al. (1998). Glycyrrhizin as a potential treatment for chronic hepatitis C. Alimentary Pharmacology & Therapeutics. — PubMed
- Sato H et al. (1996). Therapeutic basis of glycyrrhizin on chronic hepatitis B. Antiviral Research. — PubMed
- Lin JC (2003). Mechanism of action of glycyrrhizic acid in inhibition of Epstein-Barr virus replication in vitro. Antiviral Research. — PubMed
- Lampi G et al. (2001). Antiviral activity of glycyrrhizic acid derivatives against SARS coronavirus. Bioorganic & Medicinal Chemistry Letters. — PubMed
- Numazaki K et al. (1994). Effect of glycyrrhizin in children with liver dysfunction associated with cytomegalovirus infections. Tohoku Journal of Experimental Medicine. — PubMed
- Mori K et al. (1989). Effects of glycyrrhizin (SNMC: Stronger Neo-Minophagen C) in hemophilia patients with HIV-1 infection. Tohoku Journal of Experimental Medicine. — PubMed
- Curreli F et al. (2005). Glycyrrhizic acid alters Kaposi sarcoma-associated herpesvirus latency, triggering p53-mediated apoptosis in transformed B lymphocytes. Journal of Clinical Investigation. — PubMed
- Fiore C et al. (2008). Antiviral effects of Glycyrrhiza species. Phytotherapy Research. — PubMed
PubMed Topic Searches
- PubMed: Glycyrrhizin antiviral mechanism
- PubMed: Glycyrrhizin and hepatitis C
- PubMed: Topical glycyrrhetinic acid and HSV
- PubMed: Glycyrrhizin and Epstein-Barr virus
- PubMed: Stronger Neo-Minophagen C (SNMC)
Connections
- Licorice Overview
- Licorice Benefits Hub
- Adrenal Support and Cortisol
- GI Health and Ulcers
- Cortisol and Hypertension Warning
- Lemon Balm
- Elderberry
- Olive Leaf
- Echinacea
- Hepatitis
- Herpes Simplex Virus
- Epstein-Barr Virus
- Chronic Fatigue
- Vitamin D3
- Vitamin C
- Zinc
- Lysine
- Immune Boosting