Hawthorn — Benefits Deep Dive
Hawthorn (Crataegus monogyna, C. oxyacantha / laevigata, and C. pinnatifida) has been the European traditional "heart herb" for more than 400 years. Modern phytochemistry has identified its two principal active fractions — oligomeric proanthocyanidins (OPCs) from leaves and flowers and the flavonoids vitexin, hyperoside, and rutin — as the molecular basis for its gentle but real cardiotonic effect. Germany's Commission E officially approved standardized Hawthorn extract for NYHA Class II congestive heart failure, and the SPICE and HERB CHF placebo-controlled trials demonstrate measurable hemodynamic benefit. The four deep-dive pages below explore Hawthorn's four distinct cardiovascular and emotional applications — heart failure, blood pressure, cardioprotection and angina, and the often-overlooked anxiolytic crossover effect for the patient who is "anxious-with-palpitations."
Deep-Dive Articles
Heart Failure
The HERB CHF 2009 placebo-controlled trial, the larger SPICE trial of WS 1442 extract in 2,681 NYHA II/III patients, and the German Commission E approved indication for NYHA Class II congestive heart failure. The positive inotropic mechanism of OPCs and flavonoids (cAMP-independent, contrasting with digoxin), its complementary role alongside ACE inhibitors and beta-blockers, and the practical clinical positioning of Hawthorn as a long-term safe adjunct in mild-to-moderate systolic dysfunction.
Blood Pressure
The Walker 2002 double-blind trial in type 2 diabetics showing mild but real diastolic blood pressure reduction, the broader evidence base for Hawthorn's antihypertensive effect, and the dual ACE-inhibitor-like + vasodilator mechanism through flavonoid-mediated nitric oxide release and OPC-mediated angiotensin-converting enzyme suppression. Practical positioning for mild hypertension in patients who want a food-based, multi-mechanism approach.
Cardioprotection & Angina
Hawthorn's anti-arrhythmic effect (prolongs effective refractory period), its potent antioxidant cardiac protection against ischemia/reperfusion injury, the older European clinical use for stable angina and ischemic heart disease, and the long traditional history as a gentle "heart tonic" prescribed by herbalists from Dioscorides through Maud Grieve's 1931 Modern Herbal.
Anxiety & Mood
The mild GABAergic and serotonergic effects documented in animal models, the Hanus 2004 randomized trial of a hawthorn + magnesium + California poppy combination for mild-to-moderate anxiety, and the unique "cardio-emotional crossover" niche — the patient who presents with palpitations, chest tightness, and free-floating anxiety where conventional medicine separates the cardiac and psychiatric workups. Historical use as a remedy for "broken heart" and grief.
Table of Contents
- Deep-Dive Articles
- Why Hawthorn Produces Effects
- Key Research Papers
- External Authoritative Resources
- Connections
- Featured Videos
Why Hawthorn Produces Effects
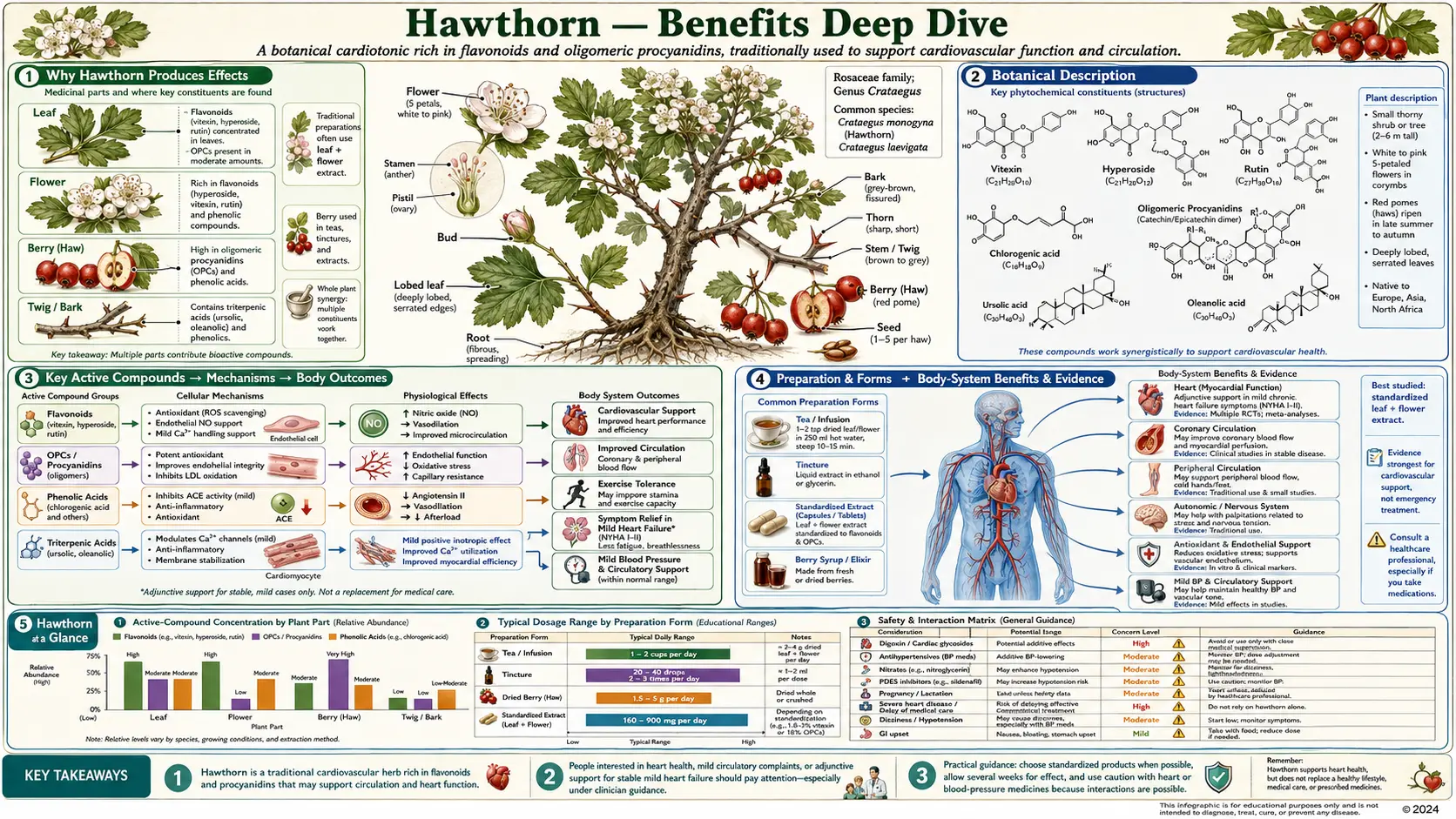
Hawthorn is unusual among medicinal plants because its principal effects cluster in a single organ system — the cardiovascular — yet within that system it touches almost every distinct mechanism the heart and vasculature use to regulate themselves. The two active fractions are well characterized:
- Oligomeric proanthocyanidins (OPCs) — condensed tannins built from catechin and epicatechin monomers, concentrated in the leaves, flowers, and (to a lesser extent) berries. OPCs are the dominant cardioactive fraction in the standardized German WS 1442 extract used in the SPICE and HERB CHF trials.
- Flavonoids — principally vitexin and vitexin-2″-O-rhamnoside, hyperoside, rutin, and quercetin glycosides. These contribute the antioxidant, vasodilator, and mild anxiolytic effects.
Together these two fractions act on five distinct cardiovascular and neurologic mechanisms, which is why Hawthorn produces such a broad set of clinical effects from a single botanical preparation:
- Positive inotropic effect (increased force of cardiac contraction) — Hawthorn OPCs increase cardiac contractility through a cAMP-independent mechanism that contrasts with digoxin (which inhibits the Na+/K+-ATPase). The inotropic effect is gentler than digoxin and lacks digoxin's narrow therapeutic window, making Hawthorn safer for long-term use in mild-to-moderate heart failure.
- ACE-inhibitor-like activity — both the OPC fraction and several Hawthorn flavonoids inhibit angiotensin-converting enzyme in cell-free and animal models. This produces a mild but real reduction in blood pressure through the same renin-angiotensin axis that lisinopril and enalapril target pharmacologically.
- Endothelial vasodilation — flavonoids in Hawthorn (particularly vitexin and hyperoside) trigger endothelial nitric oxide synthase (eNOS) activity, producing NO-mediated vasodilation that complements the ACE-inhibitor-like effect. Vasodilation reduces afterload, which helps both the failing heart and the hypertensive patient.
- Antioxidant cardioprotection — the OPC fraction is among the most potent free-radical scavengers in the plant kingdom on a milligram-per-milligram basis. In animal models of ischemia/reperfusion injury, Hawthorn extract reduces infarct size and preserves contractile function, with the protective effect attributed to scavenging reactive oxygen species generated during reperfusion. This is the mechanism behind Hawthorn's cardioprotective and anti-anginal effects.
- Mild nervine / anxiolytic action — flavonoids in Hawthorn show binding affinity for GABA-A receptors in radioligand-binding studies, and animal models show anxiolytic activity in the elevated plus-maze paradigm at relevant doses. The serotonergic contribution appears smaller but is documented. This is the molecular basis for the traditional use of Hawthorn for "anxious-with-palpitations" presentations.
The combined effect is what nineteenth-century herbalists called a "heart tonic" — a gentle, multi-mechanism agent that supports cardiac function across several axes simultaneously without the narrow therapeutic window of digoxin or the systemic effects of beta-blockers. Modern phytochemistry has substantially validated this traditional characterization.
Drug interaction note — digoxin and beta-blockers: because Hawthorn produces a mild positive inotropic effect of its own, the theoretical concern is additive contractility when combined with digoxin (also positive inotropic) or potential blunting of beta-blocker negative inotropic action. In practice, the magnitude of Hawthorn's inotropic effect is small enough that combination use is generally well tolerated, but patients on digoxin should have serum digoxin levels monitored when starting or stopping Hawthorn, and those on beta-blockers may want to coordinate the addition with their cardiologist. The SPICE trial enrolled patients on standard heart failure regimens (ACE inhibitors, beta-blockers, diuretics) and found Hawthorn well tolerated as an add-on.
Key Research Papers
- Holubarsch CJF et al. (2008). The efficacy and safety of Crataegus extract WS 1442 in patients with heart failure: the SPICE trial. European Journal of Heart Failure 10(12):1255-1263. — PubMed: Holubarsch SPICE 2008
- Zick SM et al. (2009). The effect of Crataegus oxycantha Special Extract WS 1442 on clinical progression in patients with mild to moderate symptoms of heart failure (HERB CHF). European Journal of Heart Failure 11(10):990-999. — PubMed: Zick HERB CHF 2009
- Pittler MH et al. (2008). Hawthorn extract for treating chronic heart failure (Cochrane review). Cochrane Database Syst Rev. — PubMed: Pittler Cochrane 2008
- Walker AF et al. (2002). Promising hypotensive effect of hawthorn extract: a randomized double-blind pilot study of mild, essential hypertension. Phytotherapy Research 16(1):48-54. — PubMed: Walker 2002
- Hanus M et al. (2004). Double-blind, randomised, placebo-controlled study to evaluate the efficacy and safety of a fixed combination containing two plant extracts (Crataegus oxyacantha and Eschscholtzia californica) and magnesium in mild-to-moderate anxiety disorders. Current Medical Research and Opinion 20(1):63-71. — PubMed: Hanus 2004
External Authoritative Resources
- European Medicines Agency (EMA) — Crataegi folium cum flore herbal monograph — the EU's formal regulatory monograph on Hawthorn leaf and flower
- NIH NCCIH — Hawthorn — National Center for Complementary and Integrative Health overview
- MedlinePlus — Hawthorn — consumer-facing safety and efficacy reference
- ESCOP — European Scientific Cooperative on Phytotherapy (Hawthorn leaf and flower monograph, fee-based access)
- PubMed — All research on Crataegus and the heart
Connections
- Hawthorn (Main Page)
- Hawthorn for Heart Failure
- Hawthorn for Blood Pressure
- Hawthorn for Cardioprotection & Angina
- Hawthorn for Anxiety & Mood
- All Herbs
- Heart Failure
- Hypertension
- Anxiety
- Chest Pain
- Edema
- Garlic
- Passionflower
- Lemon Balm
- Cardiovascular Health
- Blood Pressure (Celery Juice)
- Lipid Panel
- Quercetin