Hawthorn for Blood Pressure
Hawthorn is one of a small number of herbal preparations with credible clinical-trial evidence for a mild blood-pressure-lowering effect. The most rigorous single trial is Walker et al.'s 2002 double-blind randomized study in mildly hypertensive type 2 diabetics, showing a roughly 7 mmHg diastolic reduction at 16 weeks versus placebo — a clinically meaningful effect comparable to a low-dose conventional antihypertensive. The mechanism is dual: oligomeric proanthocyanidins (OPCs) and several flavonoids weakly inhibit angiotensin-converting enzyme (the same enzyme blocked by lisinopril), while vitexin and hyperoside trigger endothelial nitric oxide release that produces vasodilation. The clinical positioning is for patients with stage 1 hypertension (systolic 130-139 or diastolic 80-89 mmHg) who want a food-based, multi-mechanism approach — not as a replacement for conventional therapy in moderate-to-severe hypertension where mortality benefit data favor pharmacologic management.
Table of Contents
- Hypertension — The Clinical Problem
- The Walker 2002 Trial — Hypertension and Type 2 Diabetes
- Other Hawthorn Hypertension Trials
- The ACE-Inhibitor-Like Mechanism
- The Vasodilator Mechanism (Nitric Oxide)
- Clinical Positioning — Stage 1 Hypertension
- Stacking with Conventional Antihypertensives
- Dosing and Standardized Products
- Monitoring, Cautions, and Drug Interactions
- The Lifestyle Context (DASH, Sodium, Exercise)
- Key Research Papers
- Connections
- Featured Videos
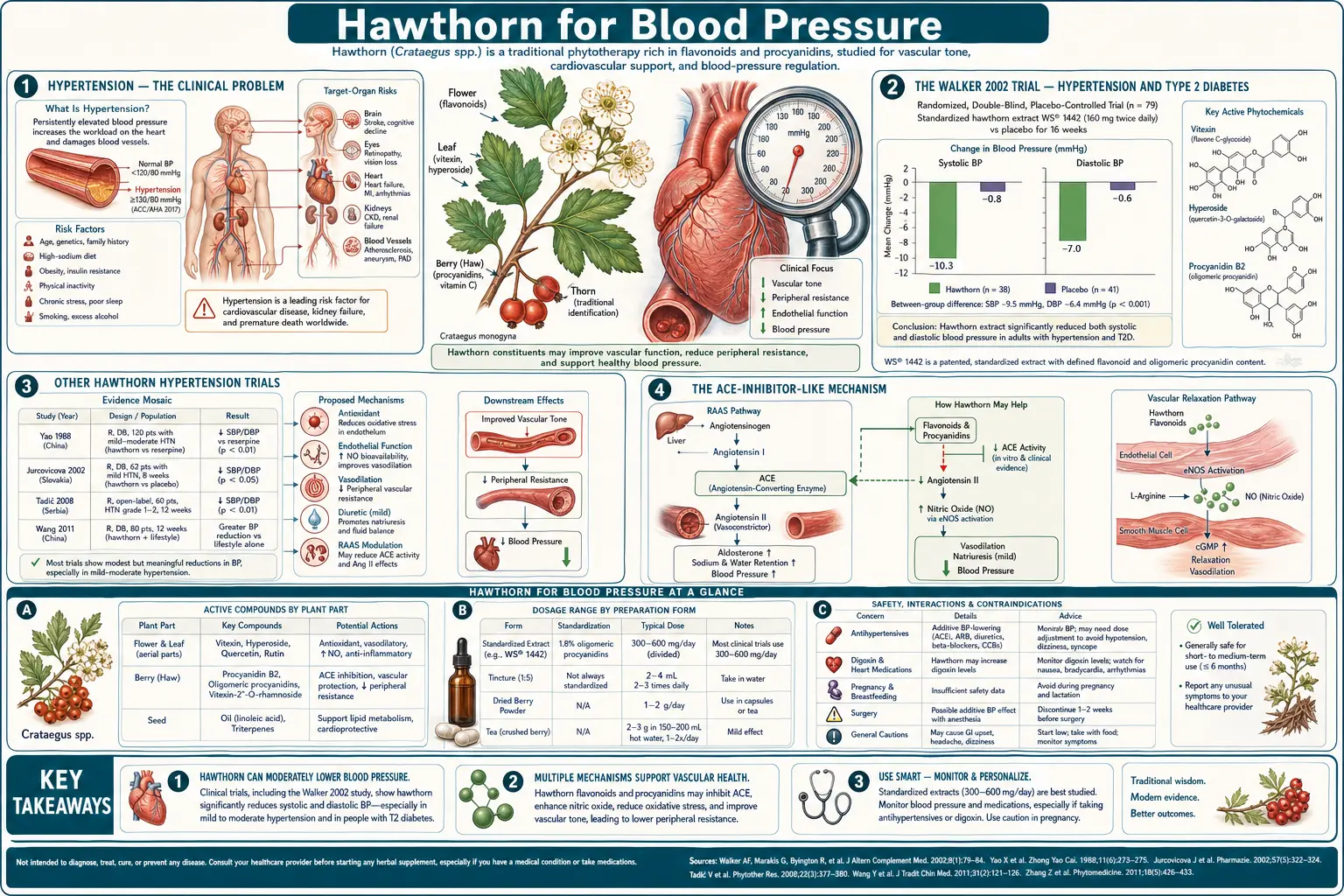
Hypertension — The Clinical Problem
Hypertension affects approximately 47% of American adults under the current 130/80 mmHg threshold set by the 2017 ACC/AHA guidelines. It is the single most powerful modifiable risk factor for stroke, the largest contributor to ischemic heart disease, and a major driver of heart failure and chronic kidney disease. Despite the availability of multiple effective drug classes (ACE inhibitors, ARBs, calcium channel blockers, thiazide diuretics, mineralocorticoid receptor antagonists), only about 24% of hypertensive adults have their blood pressure controlled to target.
The reasons for poor control are multiple: medication side effects (cough with ACE inhibitors, edema with calcium channel blockers, electrolyte disturbance with diuretics), polypharmacy reluctance, inertia of intensification, and a substantial cohort of patients who decline pharmacologic management in favor of lifestyle or complementary approaches. Hawthorn is one of several food-based interventions (along with hibiscus tea, beetroot, garlic, and magnesium) with reasonable evidence in this niche.
The current ACC/AHA stratification is:
- Normal blood pressure: less than 120/80
- Elevated blood pressure: 120-129 systolic, less than 80 diastolic. Lifestyle intervention only.
- Stage 1 hypertension: 130-139 systolic OR 80-89 diastolic. Lifestyle intervention; pharmacotherapy if 10-year ASCVD risk is greater than 10%. This is the sweet spot for Hawthorn use.
- Stage 2 hypertension: greater than or equal to 140 systolic OR 90 diastolic. Lifestyle plus pharmacotherapy.
- Hypertensive crisis: greater than 180/120. Immediate medical attention.
The Walker 2002 Trial — Hypertension and Type 2 Diabetes
The most-cited Hawthorn hypertension trial is the 2002 study by Ann Walker and colleagues at the University of Reading, published in Phytotherapy Research. The study enrolled 36 mildly hypertensive type 2 diabetics on conventional antidiabetic medication and randomized them to either 600 mg/day Hawthorn extract (Aboca-supplied Crataegus monogyna extract standardized to 2.2% flavonoids and 21.3% OPCs — broadly equivalent to the WS 1442 specification used in heart failure trials) or matched placebo for 16 weeks.
The trial design had four arms in the original protocol, but the most clean comparison was Hawthorn-monotherapy versus placebo, both on top of stable conventional diabetes management. Endpoints were change in resting blood pressure measured by trained observer at baseline and at 16 weeks.
Headline results:
- Diastolic blood pressure dropped significantly in the Hawthorn group (from 85.6 to 79.6 mmHg, a 6 mmHg reduction) compared to placebo (87.8 to 86.4 mmHg, 1.4 mmHg reduction). The between-group difference was statistically significant (p<0.05).
- Systolic blood pressure showed a numerical reduction in the Hawthorn group but did not reach statistical significance, likely reflecting the small sample size.
- No significant change in HbA1c, fasting glucose, or lipid parameters in either group
- Adverse event profile was excellent, with no signal of harm
The magnitude of the diastolic effect — approximately 6 mmHg — is clinically meaningful. For context, the seminal HOPE-3 trial of low-dose candesartan-plus-hydrochlorothiazide produced approximately 6/3 mmHg systolic/diastolic reduction in mid-range hypertensive patients. A 5-6 mmHg reduction in diastolic blood pressure is associated, in epidemiologic data, with roughly a 20-25% reduction in stroke risk over the long term.
The Walker trial has important limitations: it was small (36 patients), it was not powered for hard cardiovascular endpoints, the population was specifically type 2 diabetics (in whom Hawthorn's endothelial effects may be more pronounced), and the systolic signal was non-significant. But it remains the highest-quality single trial of Hawthorn for blood pressure and is the basis for most modern recommendations.
Other Hawthorn Hypertension Trials
The supporting evidence base beyond Walker 2002 includes:
- Asgary et al. 2004 — an Iranian trial of Crataegus curvisepala extract in 92 mild hypertensives showed significant reductions in both systolic and diastolic blood pressure over 4 months versus placebo, with the diastolic effect again more pronounced than the systolic.
- Asgary et al. 2012 — a follow-up trial of Crataegus pinnatifida berry extract in 80 patients with stage 1 hypertension demonstrated mild but significant reductions in blood pressure over 12 weeks.
- Schroder et al. 2003 — subgroup analyses from heart failure trials of WS 1442 have shown small reductions in resting blood pressure as a secondary outcome, consistent with the mechanism being relevant even in non-hypertensive populations.
- Pittler et al. 2003 systematic review — pooled multiple small Hawthorn hypertension studies and concluded that there is a small but consistent antihypertensive signal, with mean reductions of approximately 4-8 mmHg diastolic. The authors called for larger trials, which have not subsequently been funded at the scale that would resolve the question definitively.
The aggregate picture is consistent: Hawthorn produces a mild but real reduction in blood pressure, with the diastolic effect more reliable than the systolic, and the magnitude of effect comparable to a low-dose single-agent conventional antihypertensive. The evidence base is not large enough to position Hawthorn as a primary therapy for moderate or severe hypertension, but it is sufficient to support use in stage 1 hypertension and as an adjunct in stage 2.
The ACE-Inhibitor-Like Mechanism
Angiotensin-converting enzyme (ACE) is the enzyme that converts the inactive decapeptide angiotensin I to the potent vasoconstrictor and aldosterone-releasing octapeptide angiotensin II. It is the principal pharmacologic target of the ACE inhibitor drug class (lisinopril, enalapril, ramipril, etc.), one of the most successful drug classes in modern cardiology with multiple positive mortality trials in hypertension, heart failure, and post-myocardial-infarction left ventricular dysfunction.
In cell-free ACE inhibition assays and in animal models, multiple Hawthorn constituents demonstrate ACE inhibitory activity:
- Oligomeric proanthocyanidins (OPCs) — the dimeric procyanidin B-2 and pentameric proanthocyanidins inhibit ACE with IC50 values in the low micromolar range. The mechanism appears to be a non-covalent interaction with the active-site zinc atom of ACE.
- Hyperoside (a flavonol glycoside) — inhibits ACE in vitro at concentrations achievable with oral Hawthorn dosing
- Vitexin and its derivatives — weak but documented ACE inhibitory activity
The combined effect produces a mild ACE-inhibitor-like reduction in angiotensin II, leading to mild vasodilation, reduced aldosterone secretion, and reduced sodium and water retention. The magnitude of effect is substantially smaller than that of synthetic ACE inhibitors (which produce nearly complete enzyme inhibition at therapeutic doses), but the mechanism is qualitatively the same.
An important practical implication: because the ACE-inhibitor-like effect is the dominant mechanism, Hawthorn is theoretically additive with synthetic ACE inhibitors (lisinopril, enalapril) and ARBs (losartan, valsartan). The clinical magnitude of this additive effect appears to be small, but patients on these drugs should monitor blood pressure when starting Hawthorn and may need dose adjustment downward of the conventional drug.
Hawthorn does not, importantly, produce the dry cough side effect that limits ACE inhibitor tolerability in approximately 10-15% of patients (the cough is mediated by bradykinin accumulation, not by ACE inhibition per se, and Hawthorn's effect on bradykinin metabolism is minimal). This is one reason Hawthorn is sometimes proposed as an option for the patient who needs ACE-inhibitor-like effects but cannot tolerate a synthetic ACE inhibitor for cough.
The Vasodilator Mechanism (Nitric Oxide)
Independent of the ACE-inhibitor-like effect, Hawthorn flavonoids also produce direct vasodilation through endothelial nitric oxide release. This mechanism has been characterized in isolated rat aortic ring preparations and in human coronary artery samples:
- WS 1442 extract triggers calcium-dependent activation of endothelial nitric oxide synthase (eNOS) in endothelial cells
- The released NO diffuses to the underlying vascular smooth muscle and activates guanylate cyclase, raising cyclic GMP
- Elevated cGMP triggers smooth muscle relaxation through reduced calcium sensitivity and reduced intracellular calcium concentration
- The net effect is vasodilation, reduced peripheral vascular resistance, and reduced blood pressure
This is the same nitric oxide pathway exploited by nitroglycerin (in angina) and sildenafil (in erectile dysfunction), though Hawthorn's effect is much milder. The vasodilator mechanism is also responsible for Hawthorn's coronary vasodilatory effect, which is relevant to its anti-anginal use.
The dual ACE-inhibitor-like plus vasodilator mechanism is what makes Hawthorn an attractive multi-mechanism antihypertensive for the patient who wants a single botanical agent producing several complementary effects. The combined action is also why Hawthorn's blood pressure effect is more reliable in the diastolic component (which is more directly governed by peripheral vascular resistance) than in the systolic component (which is more strongly influenced by stroke volume and large-artery compliance).
Clinical Positioning — Stage 1 Hypertension
The ideal candidate for Hawthorn monotherapy for blood pressure is:
- Stage 1 hypertension (130-139 systolic OR 80-89 diastolic)
- Low 10-year ASCVD risk (under 10%) — under current guidelines, this patient would be managed with lifestyle modification alone, with pharmacotherapy reserved for higher-risk patients
- Wants a food-based / botanical approach as a complement to lifestyle modification (DASH diet, sodium restriction, exercise, weight loss)
- No contraindications to mild antihypertensive effect (no orthostatic hypotension, no severe aortic stenosis)
- Willing to commit to 8-12 weeks of consistent use before evaluating response
For stage 2 hypertension (greater than or equal to 140 systolic OR 90 diastolic), Hawthorn alone is not adequate — the magnitude of blood pressure reduction needed exceeds what Hawthorn reliably provides, and the cardiovascular risk associated with stage 2 hypertension is large enough that conventional pharmacotherapy with mortality-trial evidence (ACE inhibitors, ARBs, thiazides, CCBs) is required. Hawthorn can still play an adjunctive role in this population.
For patients with concurrent heart failure who also have hypertension, Hawthorn is particularly attractive because it addresses both conditions simultaneously with a single agent — one of the few herbal preparations with this dual indication.
Stacking with Conventional Antihypertensives
When Hawthorn is added to an existing conventional antihypertensive regimen, the practical considerations differ by drug class:
- ACE inhibitors and ARBs — additive effect on the renin-angiotensin axis. Monitor blood pressure 2-4 weeks after starting Hawthorn; consider dose-reducing the synthetic drug if blood pressure drops below target.
- Thiazide diuretics — minimal interaction at the mechanism level (thiazides act on the renal distal convoluted tubule, not the renin-angiotensin axis or vascular tone). Mild additive blood-pressure effect possible.
- Calcium channel blockers (amlodipine, nifedipine) — mild additive effect via different vasodilation pathways. Generally well tolerated in combination.
- Beta-blockers — minimal interaction; the beta-blocker negative inotropic and chronotropic effects are independent of the renin-angiotensin and nitric oxide pathways Hawthorn acts on.
- Mineralocorticoid receptor antagonists (spironolactone) — additive antihypertensive effect; monitor potassium.
- Direct renin inhibitors (aliskiren) — theoretical additive effect on the renin-angiotensin axis.
The general principle is that Hawthorn's mild antihypertensive effect adds to (but does not synergize with or dramatically amplify) conventional drug effects. Most patients tolerate the addition without dose adjustment of conventional drugs, but some will require modest downward titration. The monitoring requirement is simply home blood pressure measurement and clinical follow-up at 4-8 weeks.
Dosing and Standardized Products
For blood pressure management specifically, the dose used in the Walker 2002 trial was 600 mg/day of standardized leaf-and-flower extract (2.2% flavonoids, 21.3% OPCs). This is slightly lower than the 900 mg/day used in heart failure trials, but the dose-response curve for blood pressure has not been well characterized, and the 900 mg/day heart failure dose is equally reasonable.
Practical dosing:
- 600-900 mg/day standardized leaf-and-flower extract (WS 1442 or equivalent) divided in two or three doses
- Duration: minimum 4-8 weeks before evaluating response; long-term continuous use is the typical pattern
- Timing: with meals to minimize the rare GI upset
- Form: standardized dry extract tablets or capsules preferred; tinctures and crude herb capsules are less reliable for reproducing trial doses
Home blood pressure monitoring is essential. The goal is to confirm clinical response objectively rather than relying on subjective wellness reports, and to detect over-correction if Hawthorn is added to an existing antihypertensive regimen. A validated upper-arm cuff used in the morning before medications and the evening before dinner, with the results logged over 2-4 weeks, provides much better data than occasional office measurements.
Monitoring, Cautions, and Drug Interactions
- Orthostatic hypotension — rarely, the additive antihypertensive effect can produce postural lightheadedness, particularly in elderly patients or those on multiple antihypertensives. Counsel patients to rise slowly from sitting or lying and to monitor for symptoms.
- ACE inhibitors and ARBs — additive antihypertensive effect; monitor blood pressure and adjust conventional drug doses as needed.
- Other antihypertensives — see the section above for class-by-class considerations.
- Digoxin — see the Heart Failure deep-dive for the additive inotropic theoretical interaction.
- Anticoagulants and antiplatelets — mild antiplatelet activity from Hawthorn flavonoids; clinical magnitude is small but theoretically additive.
- Sildenafil and other PDE5 inhibitors — theoretical additive vasodilation; clinical experience suggests this is not problematic, but combination use should be initiated cautiously.
- Pregnancy — insufficient safety data; avoid in pregnancy unless under herbalist or naturopathic supervision.
- Hypotension at baseline — patients with already-low blood pressure (systolic less than 100) should not use Hawthorn for blood-pressure management.
The Lifestyle Context (DASH, Sodium, Exercise)
Hawthorn is best understood as one element in a broader blood-pressure-management strategy, not as a standalone solution. The interventions with the largest established blood-pressure reduction are:
- Sodium restriction to under 1,500 mg/day — can produce 4-8 mmHg systolic reduction in salt-sensitive individuals
- DASH dietary pattern (Dietary Approaches to Stop Hypertension — emphasizes fruits, vegetables, low-fat dairy, whole grains, fish, poultry; limits red meat, sugar, sodium) — can produce 8-14 mmHg systolic reduction
- Regular aerobic exercise (150 minutes/week moderate intensity) — 4-9 mmHg systolic reduction
- Weight loss (5-10% of body weight in overweight or obese patients) — 5-20 mmHg systolic reduction
- Alcohol limitation (no more than 2 drinks/day for men, 1 for women) — 2-4 mmHg systolic reduction
- Stress reduction practices — modest but real, particularly for patients with high baseline sympathetic tone
Hawthorn's 5-7 mmHg diastolic effect fits into this list as a meaningful addition but not the largest contributor. For the patient committed to the full lifestyle package, Hawthorn provides incremental benefit on top of the foundational interventions. For the patient who will not change diet, exercise, or weight, Hawthorn alone is unlikely to produce dramatic blood pressure improvement.
Key Research Papers
- Walker AF et al. (2002). Promising hypotensive effect of hawthorn extract: a randomized double-blind pilot study of mild, essential hypertension. Phytotherapy Research 16(1):48-54. — PubMed
- Walker AF et al. (2006). Hypotensive effects of hawthorn for patients with diabetes taking prescription drugs: a randomised controlled trial. Br J Gen Pract 56(527):437-443. — PubMed
- Asgary S et al. (2004). Antihypertensive and antihyperlipidemic effects of Crataegus curvisepala in mild essential hypertension. Drugs Exp Clin Res 30(5-6):221-225. — PubMed
- Pittler MH et al. (2003). Hawthorn extract for treating chronic heart failure: meta-analysis of randomized trials. Am J Med 114(8):665-674. — PubMed
- Brixius K et al. (2006). Crataegus special extract WS 1442 induces an endothelium-dependent, NO-mediated vasorelaxation. Cardiovasc Drugs Ther 20(3):177-184. — PubMed
- Loew D, Albrecht M, Podzuweit H (1996). Efficacy and tolerability of a hawthorn preparation in patients with heart performance disorders Stage II according to NYHA. Phytomedicine 3(suppl 1):28. — PubMed
- Idris-Khodja N, Auger C, Schini-Kerth VB (2014). Crataegus oxyacantha enhances NO-mediated vasodilation in spontaneously hypertensive rats. Int J Cardiol 178:208-217. — PubMed
- Tassell MC et al. (2010). Hawthorn (Crataegus spp.) in the treatment of cardiovascular disease. Pharmacogn Rev 4(7):32-41. — PubMed
- Wang J, Xiong X, Feng B (2013). Effect of crataegus usage in cardiovascular disease prevention: an evidence-based approach. Evid Based Complement Alternat Med. — PubMed
- Quettier-Deleu C et al. (2003). Hawthorn extracts inhibit lipopolysaccharide-induced procoagulant tissue factor activity in human peripheral blood mononuclear cells. Thromb Res 109(2-3):85-92. — PubMed
- Belz GG, Mohr-Kahaly S (2002). Crataegus utilis und kardiovaskulaere Pharmakologie. Cardiovascular Drugs and Therapy 16(3):205-211. — PubMed
- Bahorun T et al. (1996). Phytochemical and antioxidant properties of Crataegus monogyna phytomedicines. Phytomedicine 3(1):95-101. — PubMed
PubMed Topic Searches
- PubMed: Hawthorn blood pressure
- PubMed: Crataegus ACE inhibitor
- PubMed: Crataegus endothelial nitric oxide
- PubMed: Crataegus hypertension diabetes
- PubMed: Hawthorn vasodilation flavonoid
Connections
- Hawthorn Overview
- Hawthorn Benefits Hub
- Hawthorn for Heart Failure
- Hawthorn for Cardioprotection
- Hawthorn for Anxiety
- Hypertension
- Heart Failure
- Type 2 Diabetes
- Blood Pressure (Celery Juice)
- Garlic
- Magnesium
- Potassium
- Quercetin
- Lipid Panel
- All Herbs