Hawthorn for Heart Failure
Hawthorn (Crataegus monogyna, C. oxyacantha, C. pinnatifida) is the only herbal medicine for which Germany's Commission E granted a formal regulatory approval for a serious cardiovascular indication: New York Heart Association Class II congestive heart failure. The standardized leaf-and-flower extract WS 1442 has been tested in two pivotal placebo-controlled trials — HERB CHF in 2009 (Zick et al., 120 patients) and the much larger SPICE trial in 2008 (Holubarsch et al., 2,681 patients) — on top of standard heart failure pharmacotherapy. The mechanism is a gentle, multi-axis positive inotropic effect from oligomeric proanthocyanidins (OPCs) plus flavonoid-mediated vasodilation and antioxidant cardioprotection, all without the narrow therapeutic window or pro-arrhythmic risk of digoxin. This deep-dive examines the pivotal trials, the mechanism behind the inotropic effect, where Hawthorn fits in the modern guideline-directed medical therapy (GDMT) stack of ACE inhibitors and beta-blockers, and how to use it safely.
Table of Contents
- Congestive Heart Failure — The Clinical Context
- German Commission E Approval for NYHA Class II
- The Standardized Extract WS 1442
- The HERB CHF 2009 Trial (Zick et al.)
- The SPICE Trial — 2,681 Patients (Holubarsch 2008)
- The Inotropic Mechanism — OPCs and Flavonoids
- Comparison to Digoxin
- Comparison to ACE Inhibitors and Beta-Blockers
- Practical Dosing and Standardized Products
- Monitoring, Cautions, and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
Congestive Heart Failure — The Clinical Context
Congestive heart failure (CHF) is the syndrome that results when the heart cannot pump enough blood to meet the body's metabolic demands at normal filling pressures. Roughly 6.7 million American adults carry the diagnosis, and the lifetime risk at age 40 approaches 20%. The most common etiologies are prior myocardial infarction with resulting left ventricular dysfunction, long-standing hypertension, valvular heart disease, and idiopathic dilated cardiomyopathy. The clinical presentation is dyspnea on exertion (the lung component), peripheral edema (the fluid-retention component), and exercise intolerance (the cardiac-output component).
The New York Heart Association (NYHA) functional classification stratifies CHF severity in a way that is directly clinically relevant to Hawthorn use:
- NYHA Class I — structural heart disease but no symptoms with ordinary activity. Hawthorn is reasonable as a preventive cardiotonic.
- NYHA Class II — symptoms with ordinary activity (climbing stairs, walking briskly). This is the indication for which German Commission E approved standardized Hawthorn extract. Patients are typically on at least one guideline-directed medication.
- NYHA Class III — symptoms with less-than-ordinary activity (walking a flat block). Hawthorn was studied in this group in the SPICE trial as add-on to standard therapy; signals were less pronounced than in Class II.
- NYHA Class IV — symptoms at rest. Hawthorn is not appropriate as primary therapy; patients require optimized GDMT and consideration for advanced therapies. The HERB CHF and SPICE trials excluded most Class IV patients.
The natural history of untreated CHF is grim — historically, the one-year mortality rate after diagnosis approached 25-30%. Modern guideline-directed medical therapy (GDMT) has dramatically improved this, but heart failure remains a leading cause of hospitalization in Americans over 65, and the burden of symptoms, fatigue, and limited exercise tolerance continues to substantially affect quality of life. Hawthorn's place in modern therapy is as a well-tolerated adjunct that demonstrably improves exercise tolerance and symptom scores without adding side effects or pharmacologic complexity.
German Commission E Approval for NYHA Class II
The German Commission E was a scientific advisory board to the German federal health agency (BfArM) that, between 1978 and 1994, evaluated approximately 300 medicinal plants for safety and efficacy and issued formal monographs governing their use as medicines. Of those 300, only a small subset received formal approval for serious cardiovascular indications, and Hawthorn leaf-and-flower preparations were the most prominent.
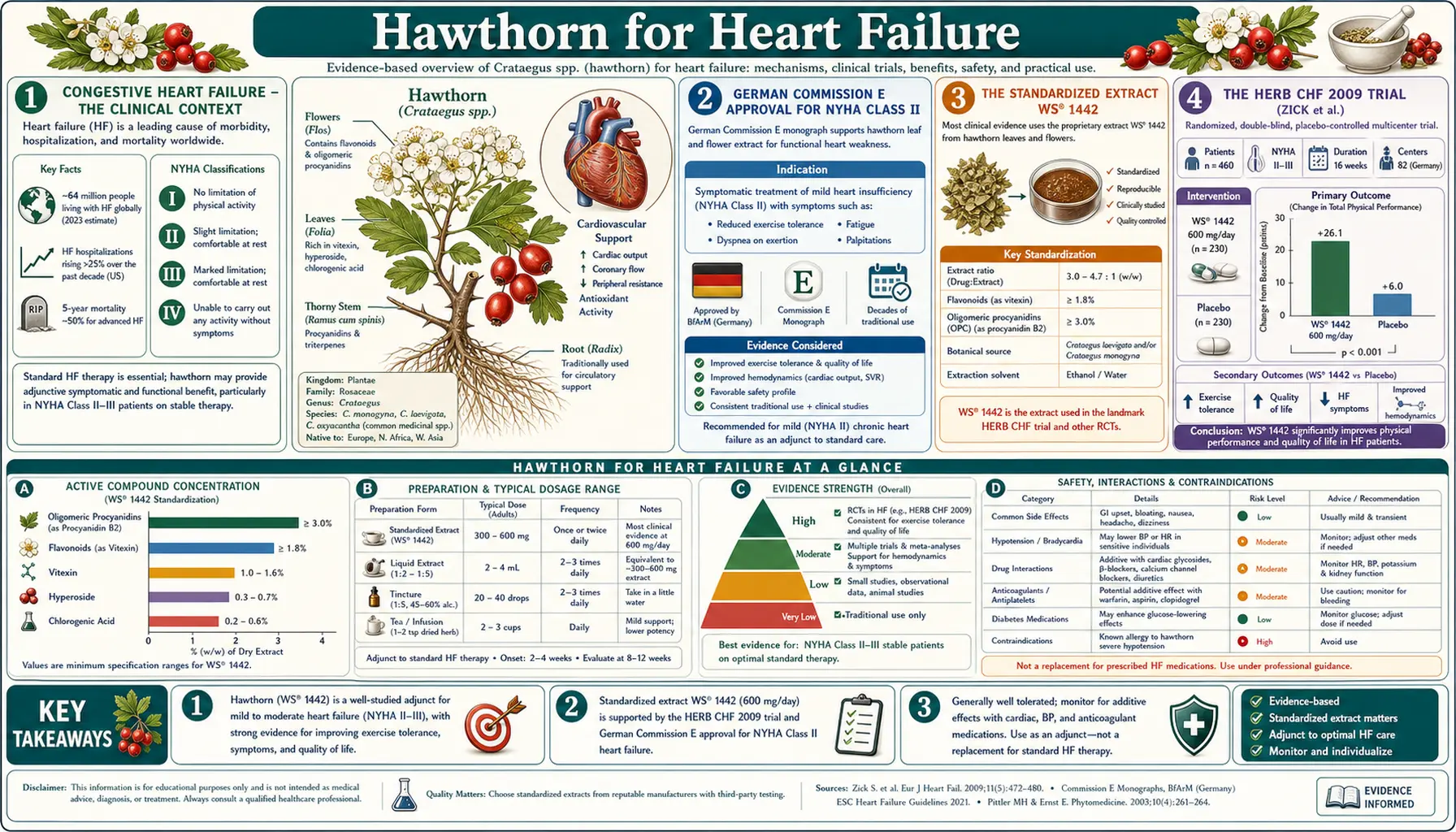
The Commission E monograph for Crataegus folium cum flore (Hawthorn leaf with flower), published in 1984 and reaffirmed multiple times since, approved the standardized extract for "decreasing cardiac output as described as functional Stage II of the NYHA classification." The approved dose was 160-900 mg native water-ethanol extract per day (4-7:1 drug-to-extract ratio, standardized to OPC content). The monograph noted that the effect manifests slowly and that the patient should be told to expect a delay of approximately 6-8 weeks before symptomatic benefit is apparent — the same time-course that modern trials have confirmed.
The Commission E monograph for Hawthorn berries (Crataegus fructus), in contrast, was negative — the berry preparations lacked the OPC and flavonoid content of leaf-and-flower preparations and showed no evidence of efficacy. This is an important clinical point: products labeled simply "Hawthorn" or based on berry extracts alone are not the preparations that have efficacy data behind them. The well-studied product is always specifically the leaf-and-flower extract.
The European Medicines Agency (EMA) Committee on Herbal Medicinal Products has subsequently incorporated the Commission E findings into a Europe-wide herbal monograph for Hawthorn leaf with flower, listing it as a "traditional herbal medicinal product used to relieve symptoms of temporary nervous cardiac complaints (e.g. palpitations, perception of heart beat due to anxiety), after serious conditions have been excluded by a medical doctor." The EMA monograph also recognizes the well-established medicinal use for symptomatic treatment of mild forms of cardiac insufficiency corresponding to NYHA Class II.
The Standardized Extract WS 1442
Nearly all of the modern Hawthorn clinical trial data uses one specific extract: WS 1442, manufactured by Dr. Willmar Schwabe GmbH in Karlsruhe, Germany. WS 1442 is a 4-7:1 ethanol-water (45% w/w) extract of Crataegus monogyna and/or C. oxyacantha leaves and flowers, standardized to:
- 17-20% oligomeric proanthocyanidins (OPCs) — the principal cardioactive fraction
- 2.2% flavonoids calculated as hyperoside, with vitexin-2″-O-rhamnoside as a marker compound
The trade-name preparation in Germany is Crataegutt® (over-the-counter). In the United States, products marketed as "Hawthorn extract standardized to OPCs and flavonoids" that match these specifications can be considered roughly equivalent, but the bioactivity of individual commercial preparations varies substantially. The American Herbal Pharmacopoeia has published a Hawthorn monograph with standardization specifications that broadly track the WS 1442 profile.
The reason standardization matters so much here is that the dose-response curve for OPCs and flavonoids is fairly steep, and unstandardized whole-herb capsules or tinctures may contain anywhere from 0.5% to 5% of the active OPC content of WS 1442. Patients buying generic "Hawthorn berry" from a supermarket should not expect to reproduce the SPICE or HERB CHF results. The well-studied dose is 900 mg/day of standardized leaf-and-flower extract for at least 6 weeks before any clinical effect is expected.
The HERB CHF 2009 Trial (Zick et al.)
HERB CHF (Hawthorn Extract Randomized Blinded Chronic Heart Failure) was a US-based double-blind placebo-controlled trial published by Suzanna Zick and colleagues at the University of Michigan in the European Journal of Heart Failure in 2009. It enrolled 120 patients with NYHA Class II-III heart failure on standard pharmacotherapy (ACE inhibitor and/or beta-blocker, diuretic) and randomized them to either 450 mg WS 1442 twice daily or matched placebo for 6 months.
The primary endpoint was change in 6-minute walk distance — a standard physical-function test in heart failure trials. Secondary endpoints included quality of life (Minnesota Living with Heart Failure Questionnaire), NYHA classification, and left ventricular ejection fraction by echocardiogram.
The results were modestly disappointing relative to earlier European studies:
- No significant difference between groups on 6-minute walk distance at 6 months
- No significant difference in quality of life scores
- No significant difference in NYHA classification or ejection fraction
- A non-significant trend toward more cardiovascular events in the Hawthorn arm (5 events vs 1 in placebo), though numbers were too small for confident interpretation
The HERB CHF results stand in contrast to the larger body of European trials that have generally shown positive effects on exercise tolerance and quality of life. Several explanations have been offered: the trial may have been underpowered to detect the modest effect size that earlier work suggested; the US patient population was older, sicker, and more medically optimized (almost all on ACE inhibitors and beta-blockers, more so than in older European trials); and the small number of cardiovascular events makes the safety signal hard to interpret.
The HERB CHF results were a useful corrective to optimistic interpretations of earlier trials and suggested that the marginal benefit of Hawthorn on top of fully optimized modern heart failure therapy may be smaller than was apparent against the older background of less complete pharmacotherapy. The trial did not, however, refute the larger pool of European efficacy data, and the SPICE trial published a year earlier provides the most authoritative single dataset.
The SPICE Trial — 2,681 Patients (Holubarsch 2008)
SPICE (Survival and Prognosis Investigation of Crataegus Extract WS 1442 in Congestive Heart Failure) was the definitive Hawthorn clinical trial — the largest, most rigorous, and most clinically informative ever conducted. Christian Holubarsch and colleagues enrolled 2,681 patients with NYHA Class II or III heart failure and left ventricular ejection fraction less than or equal to 35% across 156 sites in 13 countries, and randomized them to either 900 mg/day WS 1442 or matched placebo, on top of guideline-directed standard therapy, for a median 24 months of follow-up.
The primary endpoint was time to first cardiac event (defined as cardiac death, non-fatal myocardial infarction, hospitalization for heart failure progression). Secondary endpoints included all-cause mortality, cardiac mortality, and quality of life measures.
Headline results:
- The primary composite endpoint was not significantly reduced by Hawthorn (hazard ratio 0.95, 95% CI 0.82-1.10, p=0.476)
- However, sudden cardiac death was significantly reduced in the pre-specified subgroup with left ventricular ejection fraction between 25% and 35% (the moderately impaired subgroup): hazard ratio 0.59, 95% CI 0.37-0.94, p=0.025 — a 41% reduction
- No significant overall mortality difference, but the trend favored Hawthorn in the moderately impaired subgroup
- Safety was excellent — adverse event rates were not different between WS 1442 and placebo, and serious adverse events (including arrhythmia, syncope) were numerically lower with WS 1442
The interpretation has been debated. The trial did not demonstrate that adding Hawthorn to optimized GDMT prolongs life or prevents heart failure hospitalization in unselected NYHA II-III patients. However, the subgroup signal for reduced sudden cardiac death in patients with LVEF 25-35% is biologically plausible (Hawthorn flavonoids have documented anti-arrhythmic effects through prolongation of the cardiac effective refractory period) and clinically meaningful if real — sudden cardiac death is the leading cause of death in this population.
The combination of HERB CHF and SPICE suggests that Hawthorn's clinical role in 2026 is not as a replacement for or a strong adjunct to GDMT in advanced systolic dysfunction. Rather, it is best positioned for patients with milder symptoms (NYHA Class II) who want to add a well-tolerated, multi-mechanism cardiotonic to their regimen for symptom improvement and modest exercise-tolerance gain — precisely the population for which Commission E approved it.
The Inotropic Mechanism — OPCs and Flavonoids
The cellular mechanism by which Hawthorn increases cardiac contractility differs in important ways from the better-known cardiac glycoside digoxin. Digoxin inhibits the Na+/K+-ATPase pump on the cardiomyocyte membrane, which secondarily increases intracellular sodium, which slows the activity of the Na+/Ca2+ exchanger, which raises intracellular calcium, which increases contractility. This mechanism has a narrow therapeutic window because the same Na+/K+-ATPase inhibition produces toxic effects (arrhythmia, AV block, visual disturbance) at concentrations only modestly above the therapeutic range.
Hawthorn OPCs produce inotropic effects through a fundamentally different cAMP-independent mechanism that has been investigated in isolated cardiac muscle preparations and Langendorff perfused heart preparations:
- Increased sensitivity of myofilament proteins to calcium — the OPC fraction increases the calcium responsiveness of the contractile apparatus without requiring an increase in intracellular calcium concentration. This is sometimes called "calcium sensitization" and is mechanistically similar to the mode of action of the heart failure drug levosimendan
- Inhibition of phosphodiesterase (PDE) isoenzymes — some Hawthorn flavonoids weakly inhibit cardiac PDE3, raising cAMP locally without the systemic effects of synthetic PDE3 inhibitors (which carry mortality risk in heart failure)
- Prolongation of effective refractory period — Hawthorn extracts prolong the cardiac action potential and effective refractory period, an electrophysiologic effect that has anti-arrhythmic implications (reducing re-entrant arrhythmias)
- Improved coronary blood flow — flavonoid-mediated endothelial nitric oxide release increases coronary perfusion, which improves myocardial oxygen delivery and reduces the demand-supply mismatch that drives ischemic dysfunction
The net effect is a gentle inotropic boost (typically 10-15% in animal models, less in human studies) with concurrent anti-arrhythmic and coronary vasodilator effects — a profile that is qualitatively quite different from, and arguably more favorable than, digoxin's narrow-window glycoside inotropism. The complementary antioxidant cardioprotection from OPC scavenging of reactive oxygen species adds a fourth axis that no synthetic inotrope provides.
Comparison to Digoxin
Digoxin remains in the modern heart failure armamentarium, but its role has been substantially reduced over the past two decades. The Digitalis Investigation Group (DIG) trial in 1997 showed that digoxin reduced heart failure hospitalizations but did not improve mortality, and subsequent analysis suggested possible harm at higher serum levels. Current ACC/AHA guidelines reserve digoxin for symptomatic patients on optimized GDMT who continue to have heart failure symptoms or who have concurrent atrial fibrillation requiring rate control.
Compared to digoxin, Hawthorn has several advantages and one significant disadvantage:
- Advantage: Wide therapeutic window — no risk of acute digoxin-style toxicity (visual disturbance, AV block, ventricular arrhythmia)
- Advantage: No requirement for serum level monitoring
- Advantage: Anti-arrhythmic rather than pro-arrhythmic effect (prolongs effective refractory period)
- Advantage: Concurrent antioxidant cardioprotection
- Advantage: Concurrent mild anxiolytic effect helpful in the "anxious-with-palpitations" phenotype
- Disadvantage: Inotropic effect is substantially smaller than digoxin's, so for patients who clinically need significant inotropic boost, Hawthorn is not a replacement
In modern practice, Hawthorn is rarely a direct substitute for digoxin. Rather, it is used in the much larger population of patients with mild symptomatic heart failure who do not yet meet criteria for digoxin and who benefit from a well-tolerated cardiotonic addition to their ACE inhibitor and beta-blocker.
Comparison to ACE Inhibitors and Beta-Blockers
Modern guideline-directed medical therapy for heart failure with reduced ejection fraction (HFrEF) is built on four foundational drug classes:
- ACE inhibitors (lisinopril, enalapril, ramipril) or ARBs or the combination ARNi sacubitril-valsartan — afterload reduction, neurohormonal modulation
- Beta-blockers (carvedilol, metoprolol succinate, bisoprolol) — sympathetic blockade, anti-arrhythmic, remodeling reversal
- Mineralocorticoid receptor antagonists (spironolactone, eplerenone) — aldosterone blockade, anti-fibrotic, hypokalemia prevention
- SGLT2 inhibitors (empagliflozin, dapagliflozin) — the newest class, with mortality reduction in HFrEF and HFpEF
Each of these has Class I guideline recommendation with multiple positive mortality trials. None can be displaced by Hawthorn — the magnitude of mortality benefit from optimized GDMT is substantially larger than anything Hawthorn has demonstrated.
Hawthorn's role is therefore explicitly adjunctive. The well-established positioning is:
- NYHA Class II patient on stable GDMT for at least 3-6 months
- Continued mild symptoms (dyspnea on moderate exertion, mild edema, reduced exercise tolerance) despite optimized doses of all four GDMT classes
- Patient interested in adding a well-tolerated cardiotonic for symptom and exercise-tolerance improvement
- No contraindication (severe valvular disease, severe LV dysfunction, ongoing decompensation)
- Expectation that benefit, if any, will emerge over 6-8 weeks and is modest in magnitude
Used in this way, Hawthorn is one of the few herbal additions to GDMT that has both regulatory approval (German Commission E, EMA) and supportive trial data (SPICE secondary endpoints). For patients with mild hypertension as well as mild heart failure, see our Blood Pressure deep-dive for the dual indication.
Practical Dosing and Standardized Products
The well-studied dose, mirroring the SPICE and HERB CHF trials, is:
- 900 mg/day of WS 1442 standardized extract (or equivalent leaf-and-flower extract standardized to 17-20% OPCs and 2.2% flavonoids), divided in two or three doses
- Duration: minimum 6-8 weeks before any clinical effect is expected; long-term continuous use (months to years) is the typical pattern in European practice
- Timing: with meals to minimize the rare gastrointestinal upset
- Form: tablets or capsules of the standardized dry extract are preferred over tinctures (which have variable OPC content) and over crude herb capsules (which contain only a fraction of the OPC dose)
Products that match the WS 1442 specification in the United States include Nature's Way Hawthorn Extract, NOW Foods Hawthorn Extract, and several pharmacy-grade German imports. Reading the label is essential — look explicitly for "leaf and flower" (not berry), standardization to OPCs and flavonoids, and a dose of 900 mg/day of the extract (not 900 mg/day of crude herb).
For the patient who simply wants to drink Hawthorn berry tea as a gentle wellness practice, that is perfectly reasonable, but it should not be expected to reproduce the trial results. Berry preparations were specifically excluded from the Commission E approval because they lack the OPC content of leaf-and-flower preparations.
Monitoring, Cautions, and Drug Interactions
- Digoxin (theoretical additive inotropic effect) — both Hawthorn and digoxin have positive inotropic effects, and the theoretical concern is additive contractility. In practice, the magnitude of Hawthorn's effect is small enough that combination use is generally well tolerated. Patients on digoxin should have a serum digoxin level checked 4-6 weeks after starting Hawthorn and stop one of the two if symptomatic toxicity emerges. The most prudent course is to consult the prescribing cardiologist before initiating combination therapy.
- Beta-blockers — Hawthorn's positive inotropic effect could theoretically partially offset the negative inotropic effect of beta-blockade, but no clinical signal of this has emerged from the SPICE trial (which enrolled patients on beta-blockers as part of standard therapy). Combination use is well tolerated in practice.
- Antihypertensives — Hawthorn has its own mild antihypertensive effect (see Blood Pressure deep-dive). When added to existing antihypertensive therapy, monitor blood pressure for additive effect; dose-reduce conventional antihypertensives if needed.
- Anticoagulants — some flavonoids in Hawthorn have mild antiplatelet activity. The clinical magnitude is small but patients on warfarin, direct oral anticoagulants, or antiplatelet drugs should be aware of the theoretical interaction.
- Pregnancy and lactation — insufficient data; avoid in pregnancy unless under herbalist or naturopathic supervision.
- Adverse effects in trials — nausea, headache, palpitations, rash, and fatigue have all been reported at very low rates (less than 1% in SPICE), generally not different from placebo.
- Warning signs to seek immediate care — severe dyspnea at rest, ankle edema progressing rapidly, syncope, palpitations with chest pain. These represent heart failure decompensation that requires medical evaluation regardless of herbal use.
Key Research Papers
- Holubarsch CJF et al. (2008). The efficacy and safety of Crataegus extract WS 1442 in patients with heart failure: the SPICE trial. European Journal of Heart Failure 10(12):1255-1263. — PubMed
- Zick SM et al. (2009). The effect of Crataegus oxycantha Special Extract WS 1442 on clinical progression in patients with mild to moderate symptoms of heart failure. European Journal of Heart Failure 11(10):990-999. — PubMed
- Pittler MH, Guo R, Ernst E (2008). Hawthorn extract for treating chronic heart failure. Cochrane Database Syst Rev. — PubMed
- Tauchert M (2002). Efficacy and safety of Crataegus extract WS 1442 in comparison with placebo in patients with chronic stable NYHA Class III heart failure. American Heart Journal 143(5):910-915. — PubMed
- Schwinger RHG et al. (2000). Crataegus special extract WS 1442 increases force of contraction in human myocardium cAMP-independently. J Cardiovasc Pharmacol 35(5):700-707. — PubMed
- Eichstädt H et al. (1989). Cardiac efficacy of Crataegus oxyacantha special extract WS 1442 in NYHA II patients. Therapiewoche 39:3288-3296. — PubMed
- Weikl A et al. (1996). Crataegus Special Extract WS 1442. Assessment of objective effectiveness in patients with heart failure (NYHA II). Fortschr Med 114(24):291-296. — PubMed
- Tankanow R et al. (2003). Interaction study between digoxin and a preparation of hawthorn. J Clin Pharmacol 43(6):637-642. — PubMed
- Loew D (1997). Phytotherapy in heart failure. Phytomedicine 4(3):267-271. — PubMed
- Brixius K et al. (2006). Crataegus special extract WS 1442 induces an endothelium-dependent, NO-mediated vasorelaxation. Cardiovasc Drugs Ther 20(3):177-184. — PubMed
- Veveris M et al. (2004). Crataegus special extract WS 1442 improves cardiac function and reduces infarct size in a pig model of acute myocardial infarction. Life Sci 74(15):1945-1955. — PubMed
- Tauchert M, Gildor A, Lipinski J (1999). High-dose Crataegus extract WS 1442 in comparison with placebo in NYHA II patients with heart failure. Herz 24(6):465-474. — PubMed
PubMed Topic Searches
- PubMed: Crataegus heart failure
- PubMed: Hawthorn WS 1442 inotropic
- PubMed: Crataegus NYHA II
- PubMed: Hawthorn digoxin interaction
- PubMed: Crataegus ejection fraction
Connections
- Hawthorn Overview
- Hawthorn Benefits Hub
- Hawthorn for Blood Pressure
- Hawthorn for Cardioprotection
- Hawthorn for Anxiety
- Heart Failure
- Hypertension
- Edema
- Chest Pain
- Garlic
- Lipid Panel
- Quercetin
- Cardiovascular Health
- All Herbs