Hawthorn for Anxiety and Mood
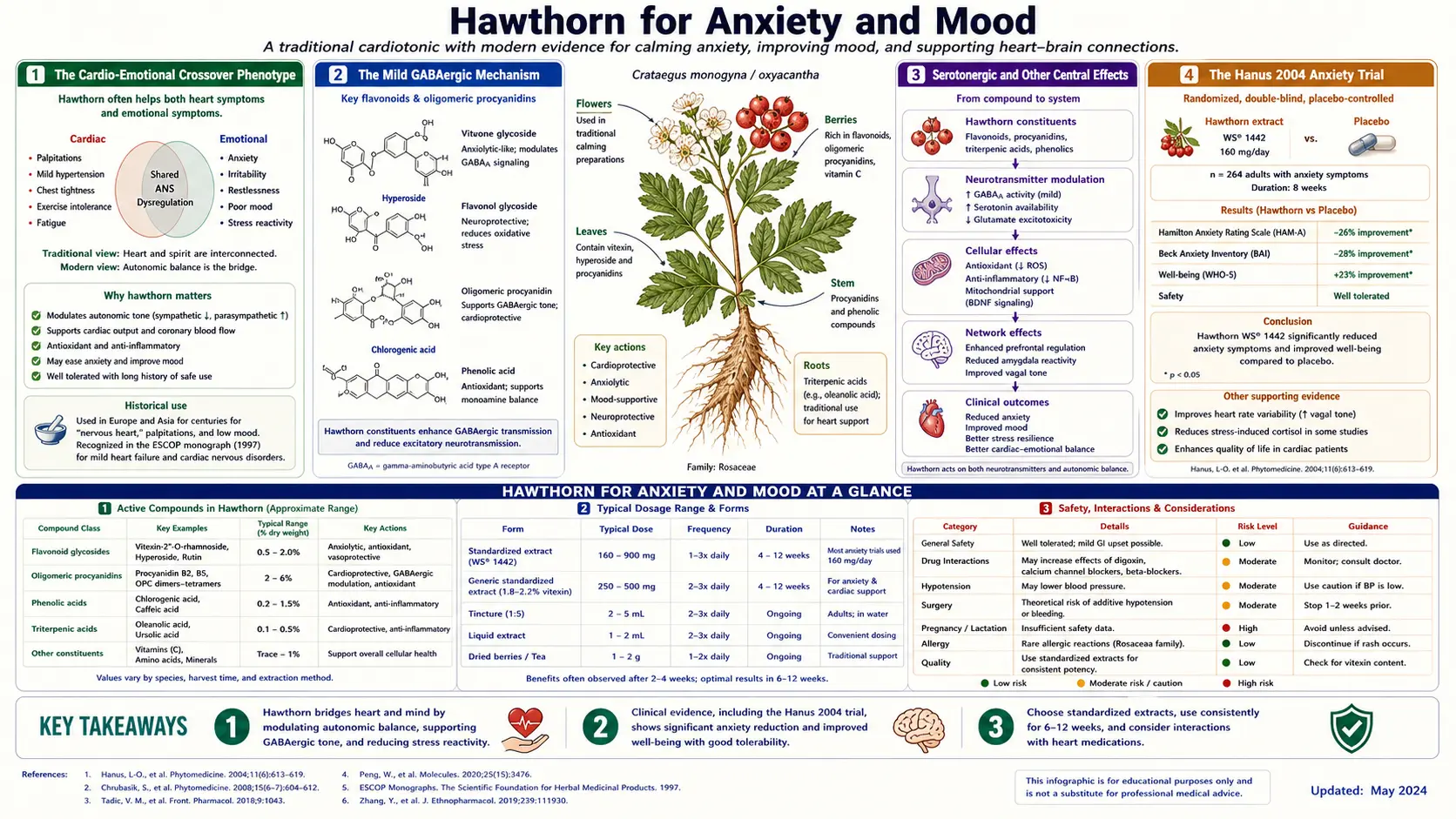
Hawthorn occupies an unusual niche in the herbal pharmacopoeia: it is the only botanical with both a formally approved cardiac indication (NYHA Class II heart failure) and a credible mild anxiolytic effect, making it uniquely suited to a particular patient phenotype that conventional medicine often handles awkwardly — the patient who is "anxious-with-palpitations." Modern phytochemistry has documented Hawthorn flavonoid binding to GABA-A receptors in radioligand studies, anxiolytic activity in animal models, and a meaningful effect in the 2004 Hanus randomized trial of a hawthorn + magnesium + California poppy combination for mild-to-moderate generalized anxiety. The traditional European herbalist's use of Hawthorn for "broken heart," grief, and emotional distress — once dismissed as folkloric — rests on a real but mild molecular foundation in central nervous system modulation. This deep-dive examines the cardio-emotional crossover, the relevant clinical evidence, and the practical positioning of Hawthorn for the anxious patient with cardiovascular symptoms.
Table of Contents
- The Cardio-Emotional Crossover Phenotype
- The Mild GABAergic Mechanism
- Serotonergic and Other Central Effects
- The Hanus 2004 Anxiety Trial
- The "Anxious-with-Palpitations" Patient
- The "Broken Heart" Tradition — Grief and Loss
- Sleep and Daytime Relaxation
- Combinations with Other Herbal Nervines
- Positioning vs Conventional Anxiolytics
- Dosing and Practical Use
- Key Research Papers
- Connections
- Featured Videos
The Cardio-Emotional Crossover Phenotype
One of the most common and most poorly managed presentations in primary care is the patient who reports a cluster of cardiac-feeling symptoms — palpitations, chest tightness, sense of irregular heartbeat, lightheadedness, racing heart with exertion — against a background of generalized or situational anxiety. This patient is shuttled awkwardly between cardiology (which finds nothing structurally wrong on echocardiogram, no ischemia on stress test, and possibly some benign ectopy on Holter monitor) and psychiatry (which diagnoses generalized anxiety disorder or panic disorder and prescribes an SSRI or benzodiazepine, with variable effect on the cardiac-feeling symptoms).
What is going on physiologically:
- Autonomic sympathetic overdrive raises heart rate, increases premature ventricular contractions (PVCs) and premature atrial contractions (PACs), and amplifies somatic awareness of normal cardiac sensations
- Hyperventilation (often subconscious) lowers arterial CO2, producing cerebral vasoconstriction and lightheadedness
- Catecholamine release (epinephrine, norepinephrine) directly produces tachycardia, tremor, and the subjective sense of impending doom
- The patient's heightened awareness of cardiac sensation feeds back into anxiety in a self-reinforcing loop — the "cardiac anxiety" phenotype
Conventional medicine separates the cardiac and psychiatric workups, which often misses the unity of the underlying problem. Beta-blockers (propranolol) can reduce both the sympathetic-driven cardiac symptoms and the somatic anxiety symptoms but carry their own side effect profile. Benzodiazepines acutely reduce anxiety but carry dependence risk. SSRIs work over weeks for the underlying anxiety but do not directly address the acute cardiac sensation.
Hawthorn fits this phenotype uniquely because its dual cardiac + mild anxiolytic effects address both elements of the syndrome with a single low-side-effect agent. This is precisely the use case that the European traditional herbal practice has emphasized for centuries.
The Mild GABAergic Mechanism
The gamma-aminobutyric acid (GABA) system is the dominant inhibitory neurotransmitter system in the mammalian central nervous system, mediating most of the brain's acute calming and anxiety-reducing effects. Pharmacologic activation of GABA-A receptors (the ionotropic receptor for which benzodiazepines, barbiturates, and ethanol are positive allosteric modulators) produces sedation, anxiolysis, anticonvulsant effect, and muscle relaxation in a dose-dependent fashion.
Several Hawthorn flavonoids have demonstrated binding affinity for the benzodiazepine site on the GABA-A receptor in radioligand displacement studies:
- Vitexin — flavone C-glycoside; mild but measurable displacement of [3H]-flunitrazepam from cortical membranes
- Vitexin-2″-O-rhamnoside — the major flavonoid in WS 1442; similar GABA-A interaction
- Hyperoside (a flavonol-3-glycoside) — weaker but measurable GABA-A binding
- Apigenin (also present in many Crataegus preparations) — better-characterized partial GABA-A agonist with documented anxiolytic activity in animal models
The affinities are in the low micromolar range — substantially weaker than synthetic benzodiazepines (which act in the nanomolar range) but biologically meaningful at therapeutic doses. In rodent anxiolytic models (elevated plus maze, light-dark box, social interaction test), Hawthorn extracts produce anxiolytic effects comparable to low-dose diazepam without producing the same level of sedation or motor impairment — consistent with a partial agonist or weak full agonist profile.
The lack of dependence potential is one of the most clinically attractive features. Unlike benzodiazepines, Hawthorn does not appear to produce tolerance, withdrawal symptoms, or rebound anxiety on discontinuation. This makes it a much safer option for long-term use in patients with chronic mild anxiety, where benzodiazepines are pharmacologically problematic.
Serotonergic and Other Central Effects
Beyond the GABAergic mechanism, Hawthorn extracts have documented but smaller effects on:
- 5-HT (serotonin) signaling — mild 5-HT receptor binding in vitro for several Crataegus flavonoids; the clinical significance is uncertain but it may contribute to the overall calming effect
- Monoamine oxidase A (MAO-A) inhibition — very weak MAO-A inhibition has been documented for some Hawthorn flavonoids; clinically negligible at oral dosing
- NMDA receptor modulation — some animal-model evidence of NMDA receptor effects that may contribute to neuroprotection
- BDNF (brain-derived neurotrophic factor) elevation — chronic Hawthorn administration in animal models produces small increases in BDNF expression, suggesting potential antidepressant adjacency
None of these mechanisms is large enough on its own to position Hawthorn as a primary antidepressant or anxiolytic, but together they produce a gentle multi-axis central nervous system calming effect that complements the GABAergic mechanism.
The combined neuropharmacologic profile is closest in spirit to that of lemon balm (also mildly GABAergic + serotonergic), passionflower (GABAergic), and California poppy (mildly opioid + GABAergic) — all the gentle European nervines that work through GABAergic + serotonergic combinations rather than the stronger sedation of valerian or the dopamine-modulating effects of St. John's Wort.
The Hanus 2004 Anxiety Trial
The pivotal human clinical evidence for Hawthorn's anxiolytic effect comes from a 2004 randomized double-blind placebo-controlled trial by Hanus and colleagues, published in Current Medical Research and Opinion. The trial enrolled 264 patients with mild-to-moderate generalized anxiety disorder (Hamilton Anxiety Scale score 16-28) and randomized them to either a fixed combination of Crataegus oxyacantha (hawthorn) + Eschscholtzia californica (California poppy) + magnesium, or matched placebo, for 12 weeks.
The active arm received:
- Hawthorn (Crataegus oxyacantha) extract: 75 mg per dose
- California poppy (Eschscholtzia californica) extract: 20 mg per dose
- Magnesium: 75 mg per dose (as marine-source elemental magnesium)
- 2 tablets twice daily, for a total daily dose of 300 mg hawthorn + 80 mg California poppy + 300 mg magnesium
The primary endpoint was change in Hamilton Anxiety Scale (HAM-A) score from baseline to 12 weeks. Secondary endpoints included Hamilton Depression Scale, subjective sleep quality, and safety.
Headline results:
- HAM-A total score dropped significantly more in the active group than placebo (mean reduction of 10.6 vs 8.9 points, p=0.005)
- Improvement was apparent by week 4 and continued through week 12
- The somatic anxiety subscale showed particularly strong response (heart-rate, palpitations, GI complaints — consistent with Hawthorn's cardiac mechanism)
- Adverse event rates were not different from placebo
- No dependence, withdrawal, or rebound symptoms on discontinuation
The trial has some important limitations: the active arm was a three-component formulation, so the individual contribution of Hawthorn cannot be cleanly separated from the California poppy and magnesium contributions. Both of those other components have anxiolytic effects of their own (California poppy is mildly GABAergic + opioidergic; magnesium has documented effects on glutamate/NMDA signaling and the stress response). The 1.7-point HAM-A difference, while statistically significant, is modest in clinical magnitude.
Despite these limitations, the Hanus trial remains the highest-quality human evidence for Hawthorn's anxiolytic effect in a defined anxious population, and it has driven the inclusion of hawthorn-containing combinations in European pharmacy-grade anxiolytic preparations such as Sedariston, Calmosedine, and similar branded products.
The "Anxious-with-Palpitations" Patient
The patient phenotype where Hawthorn is most uniquely useful is the "anxious-with-palpitations" presentation:
- Predominant somatic anxiety symptoms (palpitations, chest tightness, tremor, sweating, GI complaints) rather than purely cognitive worry
- Cardiology workup negative for structural heart disease, ischemia, or sustained arrhythmia — possibly with documented benign ectopy on Holter
- Generalized anxiety disorder or panic disorder, with cardiac symptoms as a prominent feature
- Patient prefers a botanical approach to chronic medication, or has failed to tolerate SSRIs / SNRIs, or wants an adjunct to existing therapy
- Possibly concurrent mild hypertension or mild ventricular dysfunction in which Hawthorn would have additional indication
For this patient, Hawthorn provides three simultaneous benefits:
- The cardiac-protective and mild anti-arrhythmic effect addresses the palpitation symptom directly (see Cardioprotection & Angina for the anti-arrhythmic mechanism)
- The mild GABAergic anxiolytic effect reduces the underlying anxiety and somatic symptom amplification
- The blood-pressure-lowering effect addresses any concurrent sympathetic-driven mild hypertension (see Blood Pressure)
The clinical experience with this combined approach in European integrative medicine is positive, even though dedicated randomized trials in the "anxious-with-palpitations" phenotype specifically are lacking. The mechanism is rational, the safety profile is excellent, and the absence of dependence risk makes long-term use feasible.
The "Broken Heart" Tradition — Grief and Loss
European folk and herbal traditions long associated Hawthorn with affairs of the heart in the emotional sense as well as the cardiac sense — it was the herbalist's remedy for "broken heart," grief, sustained sadness after loss, and what we would now recognize as bereavement reactions. This use predates any scientific understanding of mechanism and was justified primarily by long clinical observation.
Modern interpretation has shifted but not entirely dismissed this tradition. Several lines of converging evidence support a real (if modest) role for Hawthorn in the emotional component of grief and loss:
- The takotsubo / stress cardiomyopathy connection — we now know that intense emotional stress, including bereavement, can produce a transient cardiomyopathy with characteristic apical ballooning on echocardiogram. The mechanism is catecholamine surge with direct myocardial toxicity. The traditional notion that grief can "break the heart" turns out to have a literal physiological basis.
- The cardio-emotional crossover — sustained grief drives sympathetic activation, hypertension, and increased cardiovascular event risk in the year after a major loss
- The mild antidepressant and anxiolytic effects — Hawthorn's gentle central nervous system effects address the affective component of grief reactions
- The placebo and ritual elements — the act of preparing and drinking a daily Hawthorn tea may have meaning-making value beyond the pharmacology
None of this rises to the level of evidence required for a formal grief intervention claim, and Hawthorn is not a substitute for the support, time, community, and (when needed) professional grief counseling that bereavement requires. But the traditional use has more grounding than it might appear at first inspection, and the herbalist who recommends Hawthorn tea for the recently bereaved patient is drawing on a real cardio-emotional unity.
Sleep and Daytime Relaxation
Hawthorn's mild GABAergic effect translates to modest improvements in sleep quality, particularly in patients whose insomnia is driven by anxious rumination or palpitations rather than by primary insomnia. The effect is gentler than valerian (which is the canonical herbal sleep aid through stronger GABAergic activity) and substantially gentler than benzodiazepines. The clinical pattern is improved sleep continuity and reduced anxious arousal rather than dramatic sleep induction.
For daytime relaxation, the same gentle anxiolytic effect makes Hawthorn a reasonable nervine for the patient with chronic low-grade anxiety, work stress, or hyperarousal symptoms. Unlike some stronger herbal anxiolytics, Hawthorn does not produce sedation that would interfere with cognitive function or driving — the effect is more like a mild GABAergic ground tone than an acute sedative.
The patient seeking deep sleep induction would do better with valerian, lemon balm + valerian combinations, or in clinical settings with prescription sleep aids. The patient seeking mild background anxiolysis without sedation, particularly in a cardio-emotional crossover context, is well served by Hawthorn.
Combinations with Other Herbal Nervines
European traditional and modern phytotherapy frequently combines Hawthorn with other gentle nervines for synergistic effect:
- Hawthorn + Lemon Balm (Melissa officinalis) — the classic combination for the cardio-emotional crossover. Lemon balm adds 5-HT modulation and a calming "lifting" quality that complements Hawthorn's grounding cardiac effect.
- Hawthorn + Passionflower (Passiflora incarnata) — both GABAergic, with passionflower's slightly more sedating profile making this a good evening combination for the anxious patient with insomnia.
- Hawthorn + California Poppy (Eschscholtzia californica) — the Hanus 2004 combination, with the California poppy adding mild opioidergic and GABAergic effects.
- Hawthorn + Magnesium — the Hanus combination's third element. Magnesium is the cofactor for the catechol-O-methyltransferase enzyme that degrades catecholamines, and magnesium deficiency is associated with both anxiety and palpitations. Repletion has documented anxiolytic and anti-arrhythmic effects.
- Hawthorn + Linden Flower (Tilia europaea) — a traditional European bedtime infusion with mild combined cardiac and anxiolytic effects.
- Hawthorn + Motherwort (Leonurus cardiaca) — both cardiac herbs, with motherwort adding a stronger anti-palpitation effect, traditionally used for "nervous heart" conditions.
These combinations are usually formulated by traditional European herbalists and integrative medicine practitioners as individualized preparations or as branded combination tablets and tinctures. The combinations generally work additively rather than synergistically — the mechanisms are complementary but not multiplicative.
Positioning vs Conventional Anxiolytics
Modern psychiatric pharmacology for generalized anxiety disorder includes SSRIs (sertraline, escitalopram, paroxetine), SNRIs (venlafaxine, duloxetine), buspirone, hydroxyzine, and benzodiazepines (lorazepam, clonazepam, alprazolam). Each has a substantial evidence base and a defined role.
Hawthorn is not a replacement for any of these in patients with moderate-to-severe anxiety disorder. The magnitude of anxiolytic effect is too small. But Hawthorn has a defensible adjunctive or alternative role in:
- Mild generalized anxiety with HAM-A scores in the 14-20 range, where SSRIs may be overkill and benzodiazepines carry dependence risk
- Adjunct to SSRI/SNRI for the patient with prominent somatic and cardiac-feeling anxiety symptoms incompletely controlled by SSRI alone
- Alternative to benzodiazepines for the patient with episodic mild anxiety who wants to avoid the dependence trajectory
- Patient preference for botanical / integrative approach after due discussion of conventional options
- The specific cardio-emotional crossover phenotype where Hawthorn's dual mechanism is particularly well matched to the syndrome
The role is therefore niche but defensible. The patient with severe anxiety disorder, panic disorder with severe panic attacks, or major depression with anxious features needs conventional pharmacotherapy and likely cognitive-behavioral therapy — Hawthorn alone is not an adequate intervention.
Dosing and Practical Use
For the anxiolytic and cardio-emotional indication, the dosing follows the Hanus 2004 trial:
- 300-600 mg/day of standardized leaf-and-flower extract (slightly lower than the heart failure dose), divided in two or three doses with meals
- Or: a Hawthorn + magnesium + California poppy combination tablet at the Hanus dose
- Duration: 4-12 weeks to evaluate response; long-term continuous use is appropriate
- Combination preparations with lemon balm, passionflower, or linden flower are reasonable
- For acute mild anxiety episodes: Hawthorn is not effective acutely — the GABAergic effect builds over weeks of consistent use. For acute relief, conventional options (low-dose hydroxyzine, brief benzodiazepine, deep breathing techniques) are more appropriate.
Hawthorn tea as a daily ritual is a reasonable lower-potency option for patients who prefer a food-based approach over standardized extract. The tea has lower OPC content but provides the small dose plus the ritual element. The patient who wants reproducible anxiolytic effect, however, should use the standardized extract at the trial doses.
Cautions specific to the anxiolytic indication mirror the general Hawthorn cautions (see the Heart Failure deep-dive for the full list). The key additional point for anxious patients: do not combine Hawthorn with benzodiazepines or alcohol with the expectation of synergistic anxiolytic effect — the GABAergic mechanism could theoretically add, and patients should not stack multiple GABA-acting agents without medical guidance.
Key Research Papers
- Hanus M et al. (2004). Double-blind, randomised, placebo-controlled study to evaluate the efficacy and safety of a fixed combination containing two plant extracts (Crataegus oxyacantha and Eschscholtzia californica) and magnesium in mild-to-moderate anxiety disorders. Current Medical Research and Opinion 20(1):63-71. — PubMed
- Bourin M et al. (1997). A combination of plant extracts in the treatment of outpatients with adjustment disorder with anxious mood: controlled study versus placebo. Fundam Clin Pharmacol 11(2):127-132. — PubMed
- Can OD et al. (2010). Antidepressant-like effect of vitexin in BALB/c mice and evidence for the involvement of monoaminergic mechanisms. Eur J Pharmacol 699(1-3):250-257. — PubMed
- Martínez MC et al. (2017). Anxiolytic-like effects of vitexin in mice. Pharmacol Biochem Behav. — PubMed
- Avallone R et al. (2000). Pharmacological profile of apigenin, a flavonoid isolated from Matricaria chamomilla. Biochem Pharmacol 59(11):1387-1394. — PubMed
- Viola H et al. (1995). Apigenin, a component of Matricaria recutita flowers, is a central benzodiazepine receptors-ligand with anxiolytic effects. Planta Med 61(3):213-216. — PubMed
- Hellion-Ibarrola MC et al. (2008). The anxiolytic-like effects of vitexin and hyperoside in mice. Pharmacol Biochem Behav. — PubMed
- Pittler MH, Ernst E (2010). Hawthorn extract for treating chronic heart failure. Cochrane Database Syst Rev. — PubMed
- Schroder D et al. (2003). [Whether interaction between hawthorn extract WS 1442 and digoxin?]. Med Klin (Munich) 98(11):597-603. — PubMed
- Holubarsch CJF et al. (2008). The efficacy and safety of Crataegus extract WS 1442 in patients with heart failure: the SPICE trial. European Journal of Heart Failure 10(12):1255-1263. — PubMed
- Wiesneth S, Aas G, Heilmann J (2017). Chemical profiling of Crataegus species and analysis of the relations between phytochemistry and pharmacological activity. Plant Med. — PubMed
- Edwards JE, Brown PN, Talent N, Dickinson TA, Shipley PR (2012). A review of the chemistry of the genus Crataegus. Phytochemistry 79:5-26. — PubMed
PubMed Topic Searches
- PubMed: Crataegus anxiety
- PubMed: Hawthorn GABA benzodiazepine
- PubMed: Vitexin anxiolytic
- PubMed: Crataegus Eschscholtzia magnesium
- PubMed: Hawthorn palpitations nervous heart
Connections
- Hawthorn Overview
- Hawthorn Benefits Hub
- Hawthorn for Heart Failure
- Hawthorn for Blood Pressure
- Hawthorn for Cardioprotection
- Anxiety
- Heart Failure
- Chest Pain
- Passionflower
- Lemon Balm
- Magnesium
- Chamomile
- Valerian
- All Herbs