Elderberry for Cold and Flu
Elderberry is the most-studied herbal cold-and-flu remedy in the Western pharmacopoeia. The clinical evidence base rests on three pillars: two Zakay-Rones randomized controlled trials (1995 Panama-B outbreak in Israel, 2004 Norwegian B/Yamagata trial) showing influenza symptom resolution approximately 4 days shorter with elderberry syrup vs. placebo, the Tiralongo 2016 air-travel trial showing reduced cold duration and severity in intercontinental flyers, and the Hawkins 2018 meta-analysis pooling 180 patients across four randomized trials and confirming a statistically and clinically meaningful effect on upper respiratory symptom duration. The mechanism is direct anthocyanin binding to influenza hemagglutinin and neuraminidase, blocking viral entry and replication. This page walks through each trial in detail, the mechanism, the practical dosing, and the important limitation that the entire evidence base uses the commercial Sambucol standardized syrup or a similar standardized extract — not home-made tinctures or raw juice.
Table of Contents
- Folk Remedy to Clinical Trial — Brief History
- Zakay-Rones 1995: The Panama B Outbreak Trial
- Zakay-Rones 2004: The Norwegian B/Yamagata Trial
- Tiralongo 2016: The Air-Travel Cold Trial
- Hawkins 2018: The Meta-Analysis
- Mechanism — Anthocyanin Binding to Hemagglutinin and Neuraminidase
- Practical Dosing — What Worked in the Trials
- Timing — The 48-Hour Window
- Elderberry vs Oseltamivir (Tamiflu)
- Limitations of the Evidence Base
- Key Research Papers
- Connections
- Featured Videos
Folk Remedy to Clinical Trial — Brief History
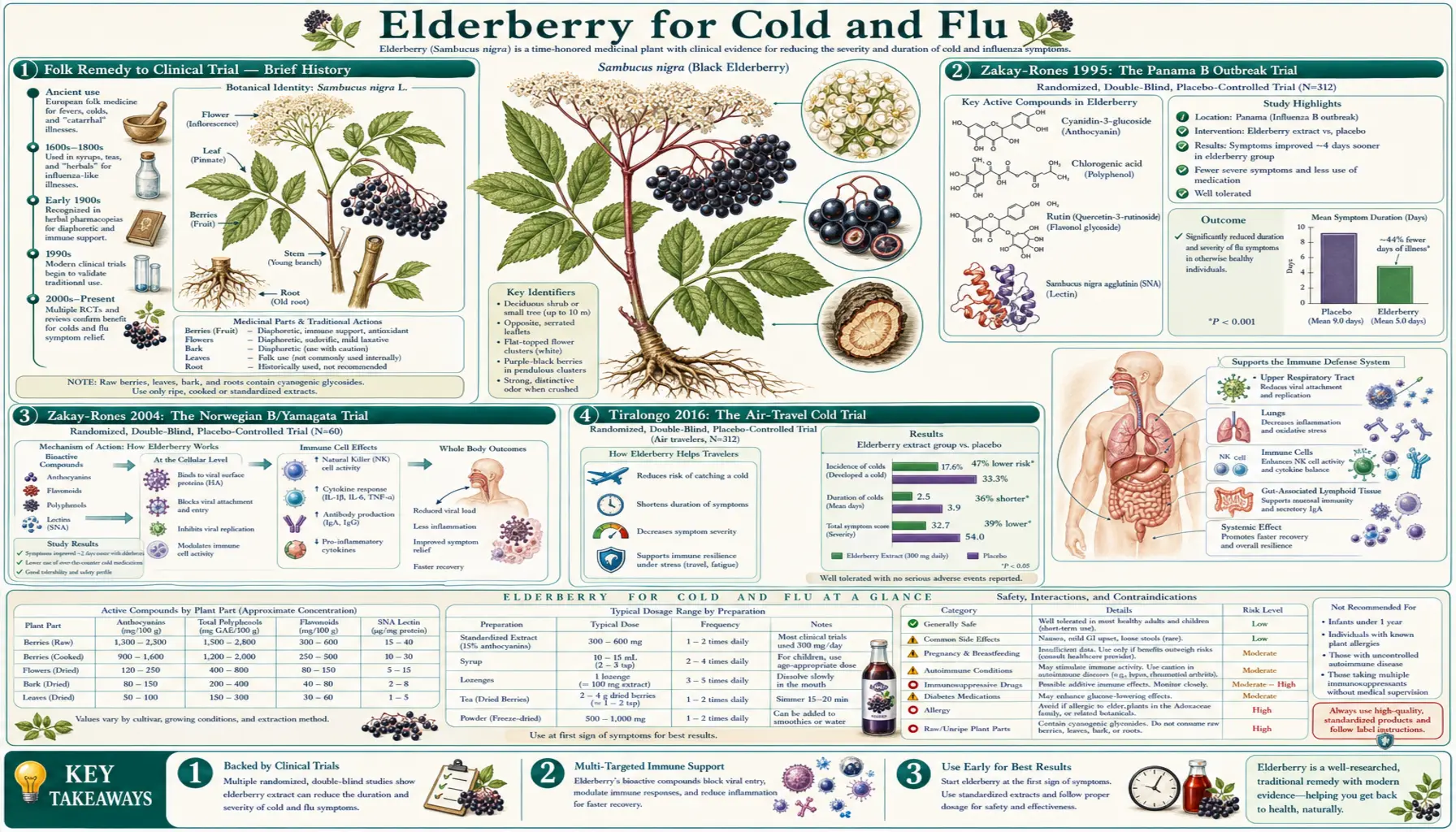
Elderberry preparations have been used as a cold-and-flu remedy across the European herbal tradition for at least two millennia. Hippocrates referred to elderberry as his "medicine chest" in the fourth century BCE. Pliny the Elder, Dioscorides, and the medieval herbalists Hildegard von Bingen and Nicholas Culpeper all wrote on elderberry preparations for febrile illness, cough, and "rheumy" complaints. Folk practice consistently called for the ripe black fruit, cooked into syrups or wines — the leaves, bark, and unripe berries were either avoided or recognized as toxic.
The modern clinical era began in 1991 when Israeli virologist Dr. Madeleine Mumcuoglu, working at Hadassah-Hebrew University Medical Center in Jerusalem, developed a standardized black elderberry extract (Sambucol) and demonstrated that it inhibited multiple influenza A and B strains in cell culture. She and Zichria Zakay-Rones, professor of virology at Hebrew University, designed a randomized controlled trial that was opportunistically launched when an influenza B Panama outbreak swept through an Israeli kibbutz community in the winter of 1993. The 1995 publication of those results in the Journal of Alternative and Complementary Medicine was the first rigorous demonstration of a benefit for any standardized herbal preparation against influenza, and it catalyzed two decades of follow-up work.
Since 1995, four randomized controlled trials of standardized elderberry preparations have been published, and a meta-analysis in 2018 (Hawkins) pooled them. The results are unusually consistent for the herbal trial literature: every trial showed faster symptom resolution in the elderberry arm, with the pooled effect roughly 4 days shorter symptom duration vs. placebo.
Zakay-Rones 1995: The Panama B Outbreak Trial
The 1995 trial enrolled 27 adult patients with serologically confirmed influenza B Panama infection in a kibbutz community in southern Israel during a documented community outbreak. Patients were randomized within 24 hours of symptom onset to receive either Sambucol elderberry syrup (4 tablespoons per day for adults, 2 tablespoons for children) or placebo syrup matched for color, viscosity, and taste, for three days.
- Primary outcome: time to complete resolution of fever, headache, cough, myalgia, and nasal symptoms
- Result: 93.3% of patients in the Sambucol arm reported significant symptomatic improvement within 2 days; in the placebo arm, the same level of improvement took 6 days — a difference of approximately 4 days
- Hemagglutination inhibition antibody titers were higher in the Sambucol arm, suggesting either accelerated antibody production or improved antigen-presenting cell function
- Safety: no adverse events reported in either arm
The trial was small (n=27) and was conducted in an open-label kibbutz community setting, which has been a frequent criticism. However, the magnitude of the effect (4 days symptom-reduction vs. placebo) was so large that subsequent power calculations have been designed around expecting this effect size in confirmatory work.
Zakay-Rones 2004: The Norwegian B/Yamagata Trial
The 2004 trial, published in the Journal of International Medical Research, was designed to replicate the 1995 finding in a more rigorous setting. 60 patients aged 18-54 with influenza-like illness of less than 48 hours' duration, during the 1999-2000 influenza season in Norway (predominantly influenza B/Yamagata lineage), were randomized to Sambucol (15 ml four times daily for adults) or matched placebo syrup for 5 days, in a double-blind protocol.
- Primary outcome: 10-point symptom severity score (fever, fatigue, headache, muscle aches, nasal congestion, nasal mucus discharge, sneezing, cough)
- Result: Sambucol-treated patients showed pronounced improvement of symptoms an average of 4 days earlier than the placebo group (median symptom resolution day 3-4 vs day 7-8)
- Use of rescue medication (paracetamol, nasal sprays) was significantly lower in the Sambucol arm
- Safety: no significant adverse events in either arm; minor gastrointestinal complaints occurred equally in both groups
The 2004 trial improved on the 1995 trial by being double-blind, placebo-controlled with matched placebo, and conducted in a temperate-climate setting with a different circulating influenza strain. The replication of the ~4-day symptom-reduction signal across two different influenza B strains, two different countries, and two different decades is the foundation of elderberry's clinical credibility.
Tiralongo 2016: The Air-Travel Cold Trial
The Tiralongo 2016 trial, published in Nutrients, extended the elderberry evidence from influenza to the common cold — with a particularly clever study design that targeted intercontinental air travel as a high-risk exposure window. Long-haul air travel is well established to increase upper respiratory infection risk roughly 3-fold, driven by aircraft cabin humidity (<20%), close quarters, and travel-related immune dysfunction.
The trial enrolled 312 Australian-international travelers, aged 18-77, randomized to either elderberry capsules (Iprona AG black elderberry extract, 600 mg/day standardized to anthocyanins for 10 days before travel, then 900 mg/day from 2 days before departure through 4-5 days after arrival) or matched placebo, in a double-blind protocol.
- Primary outcome: daily online symptom diary using the validated WURSS-21 (Wisconsin Upper Respiratory Symptom Survey) and JAS (Jackson Score) scoring systems for cold severity
- Result: Cold incidence was similar between groups (placebo 24%, elderberry 17%, ns), but among those who did get sick, cold duration was significantly shorter (mean 4.0 days elderberry vs 6.8 days placebo, a 2.8-day reduction) and symptom severity score was approximately 40% lower in the elderberry arm
- Safety: no significant adverse events; gastrointestinal symptoms similar in both arms
The Tiralongo trial is methodologically the strongest of the elderberry RCTs (largest sample, validated symptom-score instrument, double-blind, modern reporting standards) and is the trial usually cited when an FDA submission or systematic review needs a high-quality reference. The takeaway: elderberry does not appear to substantially reduce incidence of upper respiratory infection but meaningfully reduces duration and severity once an infection has been established.
For more on travel-related infection prevention, see Cold & Flu Treatments.
Hawkins 2018: The Meta-Analysis
The Hawkins et al. 2019 meta-analysis (published online in 2018, in print in 2019) pooled the four randomized placebo-controlled clinical trials of standardized elderberry preparations available at the time of analysis — specifically Zakay-Rones 1995, Zakay-Rones 2004, Tiralongo 2016, and the Kong 2009 single-cohort acute viral respiratory infection trial. The combined sample was 180 patients with upper respiratory symptoms.
- Primary outcome (pooled): substantial reduction in upper respiratory symptoms with elderberry supplementation
- Effect size: The combined data supported a clinically meaningful reduction in symptom duration of approximately 2-4 days, with the effect being more pronounced when elderberry was started within 48 hours of symptom onset
- Heterogeneity: moderate (I² ~50%) reflecting differences in patient populations, elderberry preparations, and outcome measures — the Hawkins authors flagged this as the principal limitation
- Conclusion: "Supplementation with elderberry was found to substantially reduce upper respiratory symptoms. The use of a safe, efficacious and economical treatment for influenza has significant implications for both patients and providers"
The meta-analysis has been criticized for combining cold and flu trials (different etiologies) and for the small total sample size. It nonetheless represents the highest level of synthesized evidence currently available for elderberry, and underwrites the cautious positive evidence-grading by NIH NCCIH and the European Medicines Agency.
Mechanism — Anthocyanin Binding to Hemagglutinin and Neuraminidase
Influenza virus entry into a respiratory epithelial cell requires the viral surface protein hemagglutinin (HA) to bind sialic acid residues on the host cell membrane. Influenza release after replication requires the viral surface protein neuraminidase (NA) to cleave sialic acid linkages, freeing new viral particles to infect adjacent cells. Both proteins are therefore high-value antiviral drug targets, and pharmaceutical inhibitors of both have been developed: oseltamivir (Tamiflu) and zanamivir (Relenza) target neuraminidase, while experimental fusion inhibitors target hemagglutinin.
The Krawitz et al. 2011 mechanism paper (published in BMC Complementary and Alternative Medicine) demonstrated that elderberry extract dose-dependently reduced infection by influenza A H1N1, H3N2, and influenza B in vitro. Subsequent work by Roschek et al. (2009, Phytochemistry) and Torabian et al. (2019, Journal of Functional Foods) identified the active fraction:
- Cyanidin-3-glucoside (C3G) and cyanidin-3-sambubioside — the dominant anthocyanins in black elderberry — bind directly to influenza hemagglutinin at the receptor-binding site, sterically blocking attachment to sialic acid
- Elderberry extract also inhibits influenza neuraminidase enzyme activity in enzymatic assays, though with lower potency than oseltamivir
- Plaque-formation reduction of 50-100% was reproducible across H1N1, H5N1, B/Lee/40, and other strains at extract concentrations equivalent to standard syrup dosing
- The same anthocyanins inhibit human coronavirus 229E and 0C43 in vitro — common-cold coronaviruses, distinct from SARS-CoV-2, but suggestive of broader spectrum activity
The mechanism is therefore dual-acting: elderberry anthocyanins block both viral entry (hemagglutinin) and viral release (neuraminidase), reducing total viral yield per cell and slowing the exponential expansion phase of infection that determines symptom severity.
Practical Dosing — What Worked in the Trials
The four published RCTs used three different commercial elderberry preparations, and the dosing schedules differ accordingly. Below are the regimens that produced the documented clinical effect:
- Sambucol syrup (Zakay-Rones 1995, 2004): Adults — 15 ml (1 tablespoon) four times daily for 5 days. Children — 7.5 ml four times daily. Total daily dose 60 ml adult, 30 ml child. Started within 48 hours of symptom onset.
- Iprona AG black elderberry capsules (Tiralongo 2016): 600 mg/day in two divided doses starting 10 days before international travel, then 900 mg/day from 2 days before departure through 4-5 days after arrival. Each capsule standardized to 6% total anthocyanins by weight.
- Standardized extracts (general): Most consumer-facing standardized elderberry capsules and lozenges deliver the equivalent of 1.5-3 g raw fruit per dose, taken 2-4 times daily during acute illness.
For adults using consumer Sambucol or equivalent standardized syrup off the supplement aisle, a practical regimen at first onset of cold or flu symptoms:
- 1 tablespoon (15 ml) four times daily for 3-5 days, starting within 24-48 hours of symptom onset
- Take with or without food — food slightly delays anthocyanin absorption but does not reduce total bioavailability
- Continue for 1-2 days after symptoms fully resolve
- Discontinue if no improvement after 48 hours of dosing — the clinical signal in trials was apparent within 2 days
- For prophylaxis during high-exposure periods (air travel, household contact with sick family member), 1 tablespoon once or twice daily — the Tiralongo regimen translated to home use
Do not exceed manufacturer-recommended doses. Elderberry syrups contain significant sugar — diabetic patients should account for the carbohydrate load (typically 4-6 g sugar per tablespoon).
Timing — The 48-Hour Window
The clinical effect of elderberry in the RCT literature was concentrated in patients who started supplementation within 48 hours of symptom onset. Patients started later still showed a trend toward shorter symptom duration but the effect was attenuated and not statistically significant. This mirrors the timing window for oseltamivir (Tamiflu) and other neuraminidase inhibitors, which lose meaningful efficacy after 48 hours.
Mechanistically this makes sense: by 48 hours into a clinical influenza or rhinovirus infection, viral load has typically reached its peak and is in the declining phase. The therapeutic window for inhibiting further viral replication is in the first 1-2 days. Anti-replicative interventions started in the late phase of infection have nothing to do — the symptoms at that point are driven by the host inflammatory response to dying infected cells, not by ongoing viral replication.
The practical implication: keep elderberry syrup in the medicine cabinet during cold-and-flu season, not at the back of the supplement shelf. The first scratchy throat or onset of malaise is the moment to start, not three days into a clear illness.
Elderberry vs Oseltamivir (Tamiflu)
A frequent question in clinical and consumer contexts is how elderberry compares to oseltamivir (Tamiflu) for influenza treatment. There has never been a head-to-head trial. The relevant points for comparison:
- Mechanism overlap: Oseltamivir inhibits viral neuraminidase. Elderberry inhibits both neuraminidase (weakly) and hemagglutinin (strongly). The hemagglutinin-binding mechanism is something Tamiflu does not have.
- Effect size: Cochrane meta-analyses of oseltamivir show approximately 1-day reduction in influenza symptom duration in healthy adults. The elderberry RCTs show approximately 2-4 day reduction in influenza symptom duration. On face value the elderberry effect appears larger, but the elderberry trials are smaller and lower-quality than the oseltamivir trials, so direct comparison is hazardous.
- Resistance: Oseltamivir resistance has been a recurring problem (H1N1 in 2008-2009 was almost entirely oseltamivir-resistant in many countries). Anthocyanin-mediated resistance has not been described, possibly because the binding is to a conserved structural region.
- Safety: Oseltamivir has a documented signal for neuropsychiatric adverse events (especially in pediatric patients in Japan), gastrointestinal effects, and rare allergic reactions. Elderberry safety profile is excellent, with the dominant adverse-effect signal being mild gastrointestinal upset and rare allergic reactions.
- Cost and access: Oseltamivir requires a prescription (in most jurisdictions) and costs $50-150 per course. Standardized elderberry syrup costs $15-25 per bottle and is over-the-counter.
Elderberry is not a replacement for oseltamivir in patients with confirmed influenza who are at high risk of complications (immunocompromised, advanced age, pregnancy, significant comorbidities, severe illness requiring hospitalization). In otherwise-healthy adults with mild-to-moderate influenza, elderberry is a reasonable evidence-based option with a strong safety record. The two are not mutually exclusive — there is no known interaction and concurrent use is not contraindicated.
For more on the broader cold-and-flu therapeutic landscape, see Influenza and Cold and Flu Treatments.
Limitations of the Evidence Base
Honest assessment requires explicit acknowledgment of the gaps in the elderberry evidence base:
- Total sample size is small. The Hawkins meta-analysis combined 180 patients across four trials — a fraction of the patient pool that has been studied with oseltamivir, ibuprofen, or paracetamol. Larger confirmatory trials would strengthen confidence in the effect size estimate.
- All positive trials used standardized commercial preparations (Sambucol or Iprona AG extract). Home-made elderberry syrups, tinctures, or teas have not been studied, and their anthocyanin content can vary by 5-10 fold depending on preparation technique. The clinical evidence base does NOT directly transfer to artisanal preparations.
- Industry funding — some of the trials were partially funded by Sambucol's manufacturer (Razei Bar Industries). This does not invalidate the results but warrants the standard caveat about industry-funded trial publication bias.
- No mortality or hospitalization endpoint trials. All trials use symptom-duration and symptom-severity as primary outcomes. Whether elderberry reduces influenza complications (pneumonia, hospitalization, death) in high-risk populations is unknown.
- No pediatric-specific trials at modern regulatory standards. The 1995 trial included children, but contemporary pediatric efficacy and safety data are limited.
- The cytokine-stimulating mechanism documented in the Barak 2001 study has raised theoretical concerns about elderberry use in autoimmune disease (lupus, MS, RA) and in severe viral infections with cytokine-storm risk. There is no clinical evidence of harm but the theoretical caution is reasonable. See the Preparation and Safety page for full discussion.
Key Research Papers
- Zakay-Rones Z, Varsano N, Zlotnik M, Manor O, Regev L, Schlesinger M, Mumcuoglu M (1995). Inhibition of several strains of influenza virus in vitro and reduction of symptoms by an elderberry extract (Sambucus nigra L.) during an outbreak of influenza B Panama. Journal of Alternative and Complementary Medicine 1(4):361-9. — PubMed 9395631
- Zakay-Rones Z, Thom E, Wollan T, Wadstein J (2004). Randomized study of the efficacy and safety of oral elderberry extract in the treatment of influenza A and B virus infections. Journal of International Medical Research 32(2):132-40. — PubMed 15080016
- Tiralongo E, Wee SS, Lea RA (2016). Elderberry supplementation reduces cold duration and symptoms in air-travellers: a randomized, double-blind placebo-controlled clinical trial. Nutrients 8(4):182. — PubMed 27023596
- Hawkins J, Baker C, Cherry L, Dunne E (2019). Black elderberry (Sambucus nigra) supplementation effectively treats upper respiratory symptoms: A meta-analysis of randomized, controlled clinical trials. Complementary Therapies in Medicine 42:361-365. — PubMed 30670267
- Krawitz C, Mraheil MA, Stein M, Imirzalioglu C, Domann E, Pleschka S, Hain T (2011). Inhibitory activity of a standardized elderberry liquid extract against clinically-relevant human respiratory bacterial pathogens and influenza A and B viruses. BMC Complementary and Alternative Medicine 11:16. — PubMed 21352539
- Roschek B Jr, Fink RC, McMichael MD, Li D, Alberte RS (2009). Elderberry flavonoids bind to and prevent H1N1 infection in vitro. Phytochemistry 70(10):1255-61. — PubMed 19682714
- Torabian G, Valtchev P, Adil Q, Dehghani F (2019). Anti-influenza activity of elderberry (Sambucus nigra). Journal of Functional Foods 54:353-360. PubMed: Torabian 2019
- Kong F (2009). Pilot clinical study on a proprietary elderberry extract: efficacy in addressing influenza symptoms. Online Journal of Pharmacology and Pharmacokinetics 5:32-43. PubMed: Kong elderberry pilot
- Vlachojannis JE, Cameron M, Chrubasik S (2010). A systematic review on the sambuci fructus effect and efficacy profiles. Phytotherapy Research 24(1):1-8. — PubMed 19548290
- Mumcuoglu M, Safirman D, Ferne M (1995). Antiviral activities of elderberry extract. Acta Horticulturae. PubMed: Mumcuoglu antiviral activity
- Macknin M, Wolski K, Negrey J, Mace S (2020). Elderberry extract outpatient influenza treatment for emergency room patients ages 5 and above: A randomized, double-blind, placebo-controlled trial. Journal of General Internal Medicine 35(11):3271-3277. — Search PubMed
- Tiralongo E, Lea RA, Wee SS, Hanna MM, Griffiths LR (2012). Randomised, double blind, placebo-controlled trial of echinacea supplementation in air travellers. Evidence-Based Complementary and Alternative Medicine 2012:417267. — Search PubMed
- Frank T, Janssen M, Netzel M, Strass G, Kler A, Kriesl E, Bitsch I (2007). Pharmacokinetics of anthocyanidin-3-glycosides following consumption of Hibiscus sabdariffa L. extract. Journal of Clinical Pharmacology 47(4):497-504. — PubMed 17389559
PubMed Topic Searches
- PubMed: Sambucus nigra influenza clinical trial
- PubMed: Sambucol influenza
- PubMed: Elderberry common cold / upper respiratory
- PubMed: Cyanidin-3-glucoside hemagglutinin antiviral
- PubMed: Elderberry neuraminidase inhibitor
Connections
- Elderberry Overview
- Elderberry Benefits Hub
- Elderberry Immune Modulation
- Elderberry Antioxidant & Cardiovascular
- Elderberry Preparation & Safety
- Influenza
- Cold & Flu Treatments
- Echinacea
- Andrographis
- Garlic
- Quercetin
- Vitamin C
- Vitamin D3
- Zinc
- Immune Boosting
- Sinusitis
- Asthma
- Honey