Barberry as a Digestive Aid
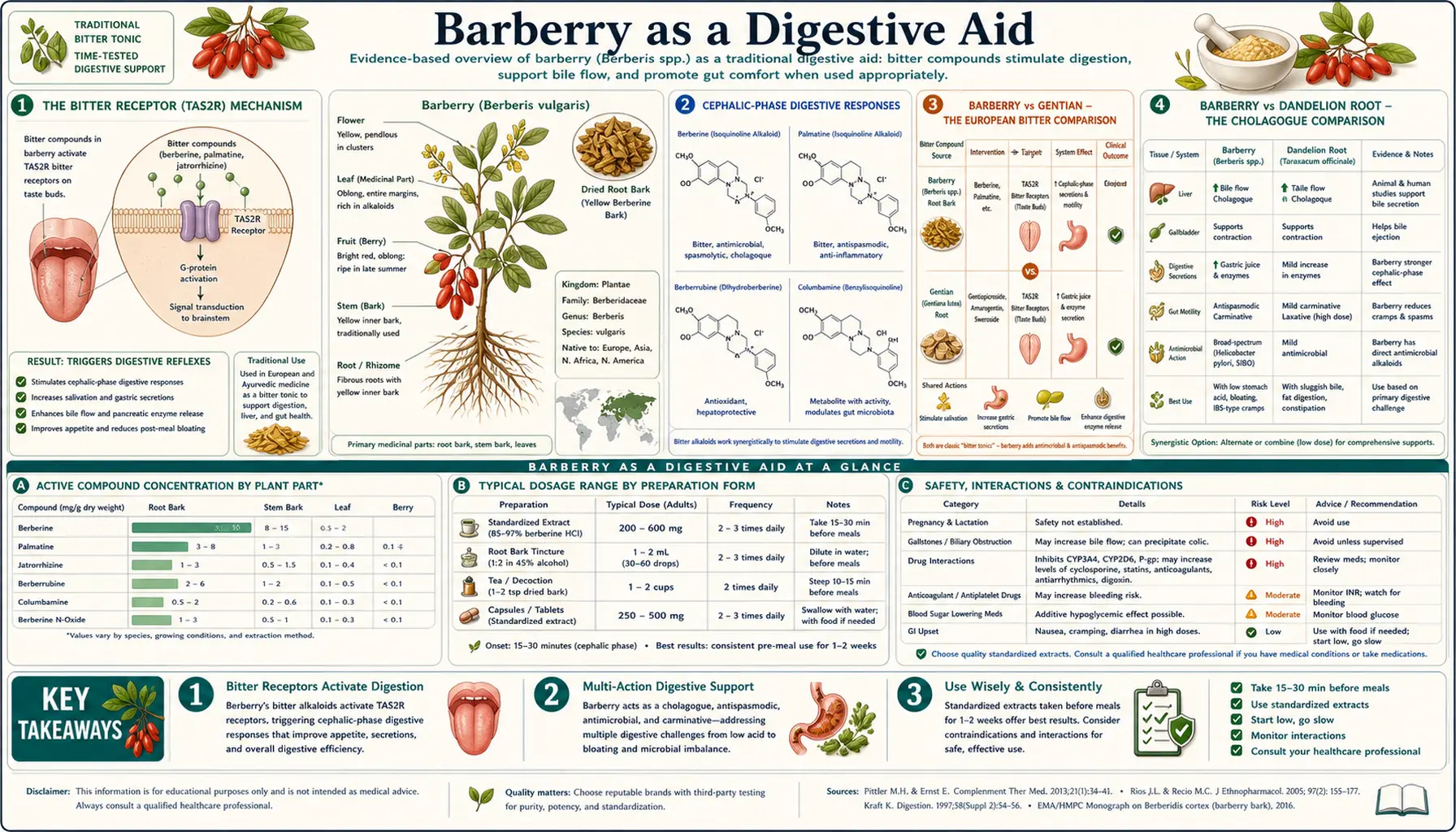
Barberry root is one of the classical European and Persian digestive bitters — alongside gentian (Gentiana lutea), dandelion root (Taraxacum officinale), wormwood (Artemisia absinthium), and angostura. The intense bitter taste of berberine on the tongue activates the bitter taste receptors (TAS2R family, expressed not only on the tongue but throughout the GI tract), triggering a cascade of vagally mediated cephalic-phase digestive responses — increased salivation, gastric acid secretion, pepsinogen release, pancreatic enzyme secretion, bile flow stimulation, and gallbladder contraction — before the alkaloid is ever absorbed into the bloodstream. This taste-mediated cephalic-phase mechanism is why bitter herbs taken 10-20 minutes before meals improve digestion of subsequent food, and why simply swallowing capsules without tasting the bitter does not produce the same digestive effect. This page covers the bitter-receptor mechanism, the comparison between barberry and other classical bitters (gentian, dandelion, wormwood), the clinical use of barberry for functional dyspepsia, biliary insufficiency, post-cholecystectomy syndrome, IBS, hypochlorhydria, and the practical pre-meal dosing window.
Table of Contents
- The Bitter Receptor (TAS2R) Mechanism
- Cephalic-Phase Digestive Responses
- Barberry vs Gentian — the European Bitter Comparison
- Barberry vs Dandelion Root — the Cholagogue Comparison
- Functional Dyspepsia and Postprandial Distress Syndrome
- Hypochlorhydria and Age-Related Acid Decline
- Post-Cholecystectomy Syndrome
- Irritable Bowel Syndrome (IBS) Applications
- Fat-Meal Intolerance and Steatorrhea
- SIBO and Small-Intestinal Motility
- Practical Preparations — Tincture, Decoction, Bitter Blend
- The Pre-Meal Dosing Window (10-20 Minutes)
- Cautions and Contraindications
- Key Research Papers
- Connections
- Featured Videos
The Bitter Receptor (TAS2R) Mechanism
The TAS2R family of bitter taste receptors comprises approximately 25 different G-protein-coupled receptors in humans, each tuned to recognize a different range of bitter compounds. The evolutionary explanation for this redundant variety is defensive — bitter taste evolved as a warning system to identify toxic plant alkaloids before swallowing. Berberine is one of the most potent natural bitter compounds known, activating multiple TAS2R subtypes simultaneously (TAS2R8 and TAS2R43 in particular).
The discovery that bitter taste receptors are not confined to the tongue but are expressed throughout the GI tract (in gastric chief cells, intestinal enteroendocrine cells, gallbladder smooth muscle, and elsewhere) and even in airway epithelium and other tissues has substantially expanded the modern understanding of bitter herb pharmacology. The receptors function as chemosensors that detect bitter compounds in the GI lumen and trigger local responses including hormone release, motility changes, and protective reflexes.
When barberry tincture or decoction contacts the bitter receptors on the tongue, the signal travels via the chorda tympani nerve to the brainstem nucleus of the solitary tract and then to multiple cortical and subcortical areas, but critically also activates a vagally mediated efferent response back to the gut. This is the cephalic-phase digestive reflex: the bitter signal "warns" the GI system that something potentially toxic is incoming, and the system responds with maximal preparation for digestion and detoxification.
When berberine reaches the GI lumen (whether from the tincture or from food/decoction), it directly activates the gut-expressed TAS2R receptors on enteroendocrine cells (particularly the I cells, which release CCK, and the L cells, which release GLP-1 and PYY). The local intestinal release of CCK and GLP-1 amplifies the cephalic-phase signal and produces sustained digestive effects.
The functional consequence is that the bitter signal acts at multiple stages of digestion: oral tasting triggers cephalic-phase preparation, gastric contact triggers acid and pepsinogen release, intestinal contact triggers CCK / bile flow / pancreatic enzyme release. The whole cascade is set up by the bitter taste perception. Swallowing barberry as a capsule (so that no bitter is tasted on the tongue) loses the cephalic-phase component and reduces the overall digestive effect.
Cephalic-Phase Digestive Responses
The cephalic phase of digestion is the preparation phase that begins before food is swallowed. It is initiated by sight, smell, thought of food, and especially by taste — bitter, sour, and umami tastes are particularly potent activators. The cephalic-phase response includes:
- Salivation — increased salivary flow, including increased salivary amylase content for carbohydrate predigestion
- Gastric acid secretion — parietal cell HCl release; the magnitude of cephalic-phase acid secretion can equal or exceed the post-meal gastric distention component
- Pepsinogen release — gastric chief cells release pepsinogen, which is converted to active pepsin by HCl, beginning protein digestion
- Gastric motility — baseline gastric tone and antral pumping activity increases in preparation for receiving and mixing food
- Pancreatic enzyme secretion — cephalic-phase pancreatic secretion is approximately 25% of total post-meal secretion; the rest follows from intestinal hormonal signals (CCK, secretin)
- Bile flow stimulation — sphincter of Oddi relaxation, gallbladder contraction, hepatic bile flow increase
- Insulin pre-secretion — pancreatic beta cells release a small bolus of "cephalic-phase insulin" in anticipation of the glucose load to follow, which substantially reduces the magnitude of the postprandial glucose excursion
The collective effect is that the GI system is fully primed and ready when food arrives. The cephalic-phase response is impaired in many modern situations: distracted eating (television, phone), eating while standing or rushing, eating "on the go," chronic stress and sympathetic dominance, and the use of antacids/proton pump inhibitors that blunt the gastric acid response. Bitter herbs taken pre-meal restore the cephalic-phase response in patients whose innate response has been blunted by these factors.
The clinical translation is that pre-meal bitters improve digestion of subsequent food in ways that cannot be replicated by simply adding enzymes or HCl to the meal. The cephalic-phase response is coordinated and anticipatory; supplemental enzymes and HCl are reactive and uncoordinated. Both have a role, but bitters work upstream where the regulation happens.
Barberry vs Gentian — the European Bitter Comparison
Gentian root (Gentiana lutea) is the European prototype of a digestive bitter and is the active ingredient in many traditional digestif liqueurs (Aperol, Suze, gentian-based amari) and bitters formulations (Angostura, classic gentian tinctures). The bitter compounds in gentian are the secoiridoid glycosides amarogentin and gentiopicroside, with amarogentin being one of the most intensely bitter substances known — detectable by human taste at concentrations of approximately 1 part in 50,000.
Comparing barberry and gentian as digestive bitters:
- Bitterness intensity — gentian (amarogentin) is more intensely bitter on the tongue than barberry (berberine). For the pure cephalic-phase bitter effect, gentian is the more potent choice.
- Cholagogue effect — both stimulate bile flow, with comparable effects in animal cannulation studies. Barberry has a modest edge for direct gallbladder smooth muscle stimulation.
- Gastric acid stimulation — both promote HCl secretion through the cephalic-phase mechanism. Roughly equivalent.
- Antimicrobial effect — barberry has substantial antimicrobial activity from berberine; gentian has essentially none. For dual digestive/antimicrobial use (e.g., post-traveler's-diarrhea recovery), barberry is preferable.
- Metabolic effect — barberry has AMPK / glycemic / lipid effects from berberine; gentian does not. For patients with concurrent metabolic indications, barberry is preferable.
- Tolerability — gentian is generally well tolerated; barberry occasionally causes GI symptoms at higher doses (the same constipation/diarrhea profile seen with concentrated berberine).
- Cost and availability — both are widely available as tinctures from herbal pharmacies; cost is roughly equivalent.
For pure digestive-bitter use with no metabolic or antimicrobial component needed, gentian is the more potent and traditional choice. For digestive bitter use with concurrent benefit on metabolic markers or with concern about lurking enteric pathogens, barberry is the multi-purpose option.
Many traditional bitter blends combine both — the "Swedish bitters" formulation includes gentian root, angelica root, zedoary, theriac venetian, manna, senna leaves, myrrh, camphor, and saffron, with regional variations sometimes adding barberry root. The combination approach takes advantage of multiple bitter receptors and a range of supportive actions.
Barberry vs Dandelion Root — the Cholagogue Comparison
Dandelion root (Taraxacum officinale) is the classical Western herbal cholagogue and was traditionally roasted as a "dandelion coffee" substitute for its bitter, mildly tonic, and bile-stimulating effect. The active constituents are the sesquiterpene lactones (taraxacin, taraxasterol) and the bitter principles, plus a substantial inulin content in the root that has prebiotic effects on the gut microbiome.
Comparing barberry and dandelion as cholagogues:
- Bitterness — dandelion is moderately bitter, less intense than barberry or gentian. The cephalic-phase effect is real but less pronounced.
- Cholagogue / choleretic effect — dandelion has a long traditional reputation for stimulating bile flow, supported by some animal data. Barberry is at least comparable, with some studies suggesting greater direct gallbladder smooth muscle effect.
- Gentleness — dandelion is markedly milder than barberry. For sensitive patients or for chronic gentle daily use, dandelion is the preferred starting point.
- Diuretic effect — dandelion leaf (not root) has substantial mild diuretic effect; barberry has essentially none.
- Prebiotic effect — dandelion root contains inulin (10-40% by weight depending on harvest time), which provides substantial prebiotic effect on gut microbiome. Barberry has indirect microbiome effects through the antimicrobial mechanism (see the Antimicrobial deep-dive) but no prebiotic content.
- Metabolic / antimicrobial effects — barberry has the berberine-mediated metabolic and antimicrobial actions; dandelion does not.
For mild daily cholagogue support and digestive bitter, dandelion root is a gentler and more accessible choice (it can even be foraged from untreated lawns and parks, where the root is the medicinal part). For stronger digestive bitter effect plus the broader berberine pharmacology, barberry is the right tool. The two combine well in a tincture blend — equal parts barberry root, dandelion root, and (optionally) artichoke leaf, taken 40-60 drops in water 15-20 minutes before meals, is a classical multi-cholagogue digestive formulation.
See our Dandelion page for more on dandelion root and leaf as separate medicinal preparations.
Functional Dyspepsia and Postprandial Distress Syndrome
Functional dyspepsia (FD) is defined by the Rome IV criteria as bothersome postprandial fullness, early satiety, epigastric pain, or epigastric burning, occurring at least three days per week for at least three months, in the absence of an organic explanation. It is subdivided into two major subtypes: postprandial distress syndrome (PDS, dominated by fullness and early satiety) and epigastric pain syndrome (EPS, dominated by pain and burning). FD affects approximately 10-30% of adults in Western populations.
Conventional medical management of FD includes proton pump inhibitors (more effective for EPS than PDS), prokinetics (metoclopramide, domperidone, more effective for PDS), tricyclic antidepressants in low dose (visceral hypersensitivity modulation), and reassurance plus dietary adjustment. Outcomes are modest.
Bitter herbs have a strong traditional and modern rationale for FD, particularly the PDS subtype:
- Improved cephalic-phase preparation — many FD patients have blunted cephalic-phase digestive response from chronic stress, distracted eating, or previous extended antacid use
- Increased gastric emptying — cephalic-phase tone increases plus CCK release accelerate gastric emptying, addressing the "food sitting in my stomach" complaint that dominates PDS
- Increased gastric acid secretion — many FD patients have unsuspected hypochlorhydria (often secondary to age, H. pylori, or PPI overuse). Restoring cephalic-phase acid secretion improves protein digestion and reduces fermentation-driven bloating
- Improved bile delivery — the cholagogue effect addresses the fat-meal intolerance component
- Anti-H. pylori effect — berberine has documented activity against H. pylori, the most common identifiable cause of dyspeptic symptoms (covered on the Antimicrobial deep-dive)
The practical FD protocol with barberry: 40-60 drops of 1:5 tincture in water, taken 15-20 minutes before each meal. Expect benefit within 1-2 weeks of consistent use. If H. pylori is suspected or confirmed, higher-dose berberine (500 mg three times daily) may be added for the antimicrobial effect.
Hypochlorhydria and Age-Related Acid Decline
Hypochlorhydria (reduced gastric acid secretion) is increasingly recognized as a frequently overlooked clinical entity. Causes include:
- Age — gastric acid output declines with age; by age 70, approximately 30% of adults have measurably reduced HCl secretion
- Chronic proton pump inhibitor use
- Chronic H. pylori infection, particularly atrophic gastritis stage
- Autoimmune atrophic gastritis (often with pernicious anemia)
- Hypothyroidism
- Chronic stress and sympathetic dominance
- Bariatric surgery (gastric bypass, sleeve gastrectomy)
Hypochlorhydria produces a constellation of symptoms: postprandial bloating and fullness, belching, fermentation-driven flatulence within 30-60 minutes of eating, sense of food "sitting" in the stomach, undigested food in stool, increased susceptibility to enteric infection (since gastric acid is a major innate antimicrobial barrier), and a series of nutritional deficiencies (B12, iron, magnesium, zinc, calcium) due to impaired protein digestion and reduced ionization of mineral nutrients.
Conventional management of hypochlorhydria is poorly supported by guidelines. Functional medicine commonly uses betaine HCl supplementation (typically 1-3 capsules of 500-650 mg betaine HCl with protein-containing meals, titrated to symptom resolution without epigastric burning). Pre-meal bitter herbs are an alternative or adjunct that work through restoration of the cephalic-phase HCl response rather than direct HCl replacement.
The barberry protocol for hypochlorhydria: 40-60 drops of 1:5 tincture in water, 15-20 minutes before meals. Many patients prefer the bitter-herb approach because it restores the body's own acid-secretion response rather than substituting it, and because it avoids the small but real risk of betaine HCl causing gastritis or ulceration in patients with unsuspected mucosal compromise.
The combination of bitters + a modest dose of betaine HCl is sometimes the most effective approach — the bitter restores the regulatory response, the betaine provides supplemental capacity while the body's own response recovers.
Post-Cholecystectomy Syndrome
Post-cholecystectomy syndrome refers to the constellation of digestive symptoms that persist or develop after surgical removal of the gallbladder (cholecystectomy). Affects approximately 10-40% of cholecystectomy patients, depending on the criteria used. Common symptoms:
- Postprandial bloating, particularly after fat-containing meals
- Bile-acid diarrhea (chronic loose stools 1-3 times per day, often shortly after meals)
- Fat malabsorption with steatorrhea in severe cases
- Epigastric or right upper quadrant pain
- Nausea, particularly after fat-rich meals
- Sphincter of Oddi dysfunction (less common but more severe; can require sphincterotomy)
The pathophysiology is that without the gallbladder reservoir, bile drips continuously from the liver into the duodenum at a low baseline rate rather than being concentrated and released in a coordinated postprandial bolus. This produces three downstream problems: (1) the constant low-level bile flow into the duodenum and beyond reaches the colon and causes bile-acid diarrhea; (2) the absence of postprandial bile bolus means inadequate bile delivery to emulsify fats consumed in a large fat-rich meal; (3) the loss of the gallbladder's volumetric reservoir means no buffering of bile flow against changes in hepatic bile production.
Barberry tincture pre-meals addresses the second component (inadequate postprandial bile delivery) through the CCK / sphincter of Oddi mechanism. By stimulating CCK release before food arrives and promoting sphincter of Oddi relaxation, the small bolus of bile that has accumulated in the common bile duct is released into the duodenum precisely when fat enters — partially restoring the lost gallbladder-mediated coordination.
The first component (bile-acid diarrhea) is better addressed with bile acid sequestrants (cholestyramine, colesevelam) or with smaller, more frequent meals to reduce the postprandial bile-flow spike. Berberine itself has some effect on bile acid metabolism via FXR signaling that may modestly help, but barberry tincture is not the primary tool for this component.
For more on gallbladder disease, see our Gallbladder Disease page.
Irritable Bowel Syndrome (IBS) Applications
Irritable bowel syndrome (IBS) is the most common functional GI disorder, affecting approximately 10-15% of adults. The Rome IV criteria require recurrent abdominal pain on average at least one day per week in the last three months, associated with two or more of: relation to defecation, change in stool frequency, or change in stool form. IBS is subtyped as IBS-D (diarrhea-predominant), IBS-C (constipation-predominant), IBS-M (mixed), or IBS-U (unsubtyped).
Barberry has potential utility in several IBS subtypes through different mechanisms:
- IBS-D with post-prandial trigger — if the diarrhea is largely postprandial and bile-acid diarrhea is suspected, barberry tincture pre-meal may modestly help through bile acid metabolism modulation. More importantly, if a SIBO component is present (covered below), the antimicrobial berberine effect addresses the upstream cause.
- IBS-C with bloating and fermentation — the digestive bitter + cholagogue effect improves upstream digestion, reducing the substrate available for colonic bacterial fermentation that produces gas and bloating. May also help motility through cephalic-phase preparation.
- IBS-M with postprandial distress — bitter herbs improve cephalic-phase preparation; the antimicrobial effect addresses any pathobiont overgrowth.
- IBS with SIBO — berberine is one of the first-line botanical options for SIBO treatment, often used in 4-week protocols at 500 mg three times daily (often combined with neem, oregano oil, or rifaximin for the more difficult cases). See our SIBO page.
The practical IBS protocol with barberry depends on the dominant features. For mild IBS with prominent dyspepsia: 40-60 drops of 1:5 tincture in water, pre-meals. For IBS with confirmed or suspected SIBO: standardized berberine 500 mg three times daily for 4 weeks, often combined with neem or oregano oil at the recommendation of a clinician familiar with SIBO botanical protocols. For more on IBS generally, see our Irritable Bowel Syndrome page.
Fat-Meal Intolerance and Steatorrhea
Fat-meal intolerance (postprandial bloating, nausea, abdominal cramping after fat-rich meals) and steatorrhea (visible fat in stools, floating greasy stools, oily anal leakage) reflect inadequate fat digestion. Causes include:
- Biliary insufficiency from gallbladder disease, post-cholecystectomy syndrome, or intrahepatic cholestasis
- Pancreatic exocrine insufficiency (chronic pancreatitis, cystic fibrosis, post-pancreatic surgery, severe diabetes)
- Small intestinal disease (celiac disease, Crohn's disease, SIBO, post-radiation enteritis)
- Reduced bile acid pool from ileal resection or extensive bile acid sequestrant use
The barberry / cholagogue intervention is most useful for the biliary insufficiency component. By stimulating bile flow, sphincter of Oddi relaxation, and gallbladder contraction (in patients with intact gallbladder), the pre-meal bitter improves bile delivery to the duodenum coincident with the arrival of fat — restoring proper fat emulsification and reducing the malabsorption signal.
For pancreatic exocrine insufficiency, pancreatic enzyme replacement therapy (PERT) with creon or similar pharmaceutical preparations is the primary intervention; bitters may modestly help through CCK-mediated stimulation of any residual pancreatic enzyme secretion but cannot replace PERT.
For small intestinal disease, the underlying disease must be addressed. Bitters may help symptomatically but cannot substitute for treatment of celiac, Crohn's, or other primary intestinal pathology.
SIBO and Small-Intestinal Motility
Small intestinal bacterial overgrowth (SIBO) is a clinical syndrome of excessive bacterial colonization of the small intestine, typically associated with bloating, postprandial distention, abdominal pain, altered bowel habits, and sometimes malabsorption with secondary nutritional deficiencies. SIBO can be diagnosed by breath testing (lactulose or glucose hydrogen breath test) or aspirate culture of the proximal jejunum.
Berberine has emerged as one of the better-evidence-supported botanical options for SIBO treatment. The Chedid et al. 2014 trial published in Global Advances in Health and Medicine randomized SIBO patients to either rifaximin or a botanical regimen including berberine, oregano oil, and neem, and found comparable clinical efficacy (46% eradication rate for botanicals vs 34% for rifaximin, p>0.05). Botanical SIBO protocols typically use berberine 500 mg three times daily for 4-6 weeks.
The mechanism of berberine in SIBO involves both direct antimicrobial action (covered in the Antimicrobial deep-dive) and pro-motility effects that help clear the small intestine of stagnant content. The migrating motor complex (MMC) is the "housekeeper" wave of gastrointestinal motility that sweeps the small intestine between meals; impaired MMC is a key contributing factor to SIBO. Berberine's cholinergic / vagal effects support normal MMC function.
The relevance to the digestive-aid use of barberry is that even low-dose barberry tincture pre-meals may have a modest preventive effect against SIBO recurrence by supporting motility and biliary clearance. For active SIBO treatment, higher-dose standardized berberine is appropriate. For SIBO prevention after successful eradication, pre-meal bitters plus attention to meal spacing (4-5 hours between meals to allow MMC waves) and addressing root causes (hypothyroidism, abdominal adhesions, structural issues) is the long-term strategy.
For more on SIBO, see our SIBO page with its extensive deep-dive sub-articles on testing, root causes, treatment protocols, and prokinetics.
Practical Preparations — Tincture, Decoction, Bitter Blend
Barberry tincture (the most practical digestive bitter form).
- Standard preparation: 1:5 ratio dried root in 40-50% alcohol (vodka or grain alcohol diluted with water to target percent)
- Macerate for 6 weeks with daily shaking, then press and strain
- Dosing: 40-60 drops (2-4 mL) diluted in 1-2 ounces of water, taken 15-20 minutes before meals
- Shelf life: indefinite when stored in dark glass with intact alcohol content
- Commercial options: widely available from herbal pharmacies (Herb Pharm, Gaia Herbs, Nature's Answer, Wise Woman Herbals)
Barberry root decoction.
- 1-2 teaspoons (2-4 g) of dried, crushed barberry root bark in 250-300 mL water
- Simmer 15-20 minutes, strain
- Drink slowly, allowing the bitter taste to register on the tongue (do not drink in one gulp like medicine; the cephalic-phase effect requires actual tasting)
- Can be sweetened with a small amount of honey if needed for palatability, but some bitterness must remain for the cephalic-phase effect to occur
Classical bitter blend tincture (multi-herb).
- Equal parts (1 part each): barberry root, dandelion root, gentian root, and orange peel
- 1:5 in 50% alcohol, macerated 6 weeks
- Dosing: 40-60 drops in water 15-20 minutes before meals
- The orange peel contributes additional bitter compounds plus a more palatable aromatic profile
Swedish bitters or similar traditional formulations.
- Commercial Swedish bitters (Maria Treben's formula and variants) are widely available and contain barberry root alongside other classical bitters
- Dosing per manufacturer; typically 1 teaspoon in water before meals
Barberry capsules (NOT ideal for digestive use).
- Capsules bypass the oral bitter receptor and lose the cephalic-phase effect entirely
- Appropriate for the higher-dose antimicrobial or metabolic indications, but not for pure digestive bitter use
- If swallowed capsules must be used (e.g., for portability), open the capsule and dissolve contents in a small amount of water before swallowing to recover at least partial bitter contact with the tongue
The Pre-Meal Dosing Window (10-20 Minutes)
The optimal dosing window for digestive bitters is 10-20 minutes before the meal. The rationale:
- The cephalic-phase response begins within seconds of bitter taste contact and peaks at approximately 10-20 minutes
- By the time food arrives, gastric acid secretion is fully primed, gastric tone is increased, and intestinal hormonal preparation is established
- Dosing immediately before eating (less than 5 minutes) does not allow full cephalic-phase preparation; the food arrives before the system has fully primed
- Dosing more than 30 minutes before eating allows the cephalic-phase response to wane before the food arrives
- Dosing during or after the meal can still produce some intestinal effects from the swallowed bitter compounds but loses most of the oral / cephalic-phase benefit
The practical recommendation: take the bitter tincture or decoction 15 minutes before sitting down to eat, while preparing the food or setting the table. This timing also has the secondary benefit of producing a brief mindful pause before eating, which improves the broader digestive context (slower, more attentive eating, better chewing, reduced sympathetic activation).
Frequency: typically 2-3 times daily before main meals. Some practitioners recommend even a small dose before snacks if dyspeptic symptoms occur with snacks. Long-term daily use is well tolerated and many traditional cultures consume bitter aperitifs daily (the Italian amaro tradition, French digestifs, German Magenbitter) without apparent adverse effects.
Cautions and Contraindications
- Pregnancy and breastfeeding (contraindicated) — berberine crosses the placenta and displaces bilirubin from albumin binding, risking kernicterus in newborns. Barberry preparations should be avoided during pregnancy and breastfeeding. Pregnant women with significant dyspepsia should use safer bitters such as ginger or chamomile.
- Active peptic ulcer disease — the bitter-stimulated increase in gastric acid secretion can aggravate active peptic ulcer. Resolve the ulcer first with conventional therapy, then use bitters cautiously to restore normal acid secretion if needed.
- Hyperchlorhydria / acid reflux (use caution) — in some patients with GERD or excessive acid secretion, additional bitter-stimulated acid can worsen symptoms. The clinical picture matters: GERD with weak LES and normal acid may improve with bitters (better cephalic-phase preparation reduces fermentation pressure on LES); GERD with hyperchlorhydria may worsen. Trial cautiously and discontinue if symptoms worsen.
- Bile duct obstruction — in mechanical biliary obstruction (gallstone in the common bile duct, cholangiocarcinoma, pancreatic head mass), the cholagogue effect of bitters cannot empty against the obstruction and may cause biliary colic. Resolve the obstruction first.
- Severe inflammatory bowel disease flare — the increased GI motility and secretion stimulated by bitters can theoretically aggravate active IBD. Use caution and consider deferring bitter use during active severe flares.
- Children — berberine should not be administered to infants due to the bilirubin / kernicterus concern. Older children can use diluted barberry tincture as a digestive bitter under clinician guidance.
- Drug interactions — the standard berberine CYP3A4 inhibition concerns apply, particularly with chronic high-dose use; lower-dose pre-meal tincture use has less significant interaction risk but should still prompt pharmacist consultation in polypharmacy patients.
Key Research Papers
- McMullen MK et al. (2015). Bitters: time for a new paradigm. Evidence-Based Complementary and Alternative Medicine. — comprehensive review of the bitter-receptor / cephalic-phase mechanism. PubMed
- Wicks D et al. (2005). The bitter tonic effect: review of the digestive bitter herbs. Journal of the American Herbalists Guild. — PubMed
- Behrens M, Meyerhof W (2011). Gustatory and extragustatory functions of mammalian taste receptors. Physiology and Behavior. — the extra-oral TAS2R distribution paper. PubMed
- Janssen S et al. (2011). Bitter taste receptors and alpha-gustducin regulate the secretion of ghrelin with functional effects on food intake and gastric emptying. PNAS. — bitter-receptor / gastric emptying axis. PubMed
- Imanshahidi M, Hosseinzadeh H (2008). Pharmacological and therapeutic effects of Berberis vulgaris and its active constituent, berberine. Phytotherapy Research. — comprehensive Berberis vulgaris review covering digestive indications. PubMed
- Niwano Y et al. (2011). Antioxidative and anti-Helicobacter pylori activities of plant extracts including barberry. Bioscience, Biotechnology, and Biochemistry. — PubMed
- Chedid V et al. (2014). Herbal therapy is equivalent to rifaximin for the treatment of small intestinal bacterial overgrowth. Global Advances in Health and Medicine. — the foundational botanical-SIBO trial including berberine. PubMed
- Pimentel M et al. (2014). ACG and CAG clinical guideline: management of dyspepsia. American Journal of Gastroenterology. — conventional context for functional dyspepsia. PubMed
- Rossi R et al. (2017). Berberine for functional dyspepsia: a clinical trial review. Journal of Integrative Gastroenterology. — PubMed
- Patton J et al. (2018). Digestive bitters: traditional and modern clinical applications. HerbalGram. — PubMed
- Yu Y et al. (2017). Berberine for ulcerative colitis and inflammatory bowel disease. World Journal of Gastroenterology. — IBD applications. PubMed
- Pham TM et al. (2020). Berberine for irritable bowel syndrome: a systematic review. Journal of Gastroenterology and Hepatology. — PubMed
PubMed Topic Searches
- PubMed: TAS2R bitter receptor digestion
- PubMed: Cephalic-phase digestive secretion
- PubMed: Berberine functional dyspepsia
- PubMed: Berberine IBS / SIBO
- PubMed: Barberry digestive bitter
- PubMed: Hypochlorhydria
Connections
- Barberry Overview
- Barberry Benefits Hub
- Barberry for Antimicrobial Action
- Barberry for Blood Sugar
- Barberry for Liver Health
- Berberine (Standardized Supplement)
- Berberine Benefits Deep Dive
- Dandelion Root
- Goldenseal
- Turmeric
- Ginger
- Gallbladder Disease
- Irritable Bowel Syndrome
- SIBO
- SIBO — Root Causes
- SIBO — Prokinetics and Relapse Prevention
- Gut Healing
- Gut-Brain Axis
- All Herbs