Barberry for Blood Sugar Regulation
Berberine — the bright-yellow isoquinoline alkaloid found at 2-3% in Berberis vulgaris root and at higher concentrations in Coptis chinensis and Phellodendron amurense — is one of the most studied botanical compounds in cardiometabolic medicine. The landmark Yin, Xing, and Ye 2008 trial published in Metabolism randomized newly diagnosed type 2 diabetics to 500 mg berberine three times daily or 500 mg metformin three times daily for three months and found the two interventions produced statistically indistinguishable reductions in HbA1c, fasting plasma glucose, and postprandial glucose. The shared upstream mechanism is AMP-activated protein kinase (AMPK) activation — the same cellular energy sensor that metformin activates — with downstream effects on hepatic gluconeogenesis suppression, peripheral glucose uptake enhancement, and insulin sensitivity restoration. This page covers the mechanism, the pivotal head-to-head trial and subsequent confirmatory work, the cardiometabolic effects beyond glycemic control, the comparison between standardized berberine supplements and whole-herb barberry preparations, the bioavailability problem and modern solutions (silymarin co-administration, dihydroberberine, liposomal formulations), and the practical clinical application in prediabetes, type 2 diabetes, metabolic syndrome, and PCOS.
Table of Contents
- The AMPK Mechanism — Cellular Energy Sensing
- The Yin 2008 Metformin Head-to-Head Trial
- Subsequent Meta-Analyses and Confirmatory Trials
- Beyond Glycemic Control: Lipid, Weight, and Inflammation
- Barberry vs Standardized Berberine — Dose Equivalence
- The Bioavailability Problem and Modern Solutions
- Dihydroberberine — the Next-Generation Form
- Prediabetes and Reversal of Insulin Resistance
- Polycystic Ovary Syndrome (PCOS) Applications
- Metabolic Syndrome and NAFLD Connection
- Combining Berberine with Metformin or Other Antidiabetics
- Practical Dosing Protocols
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
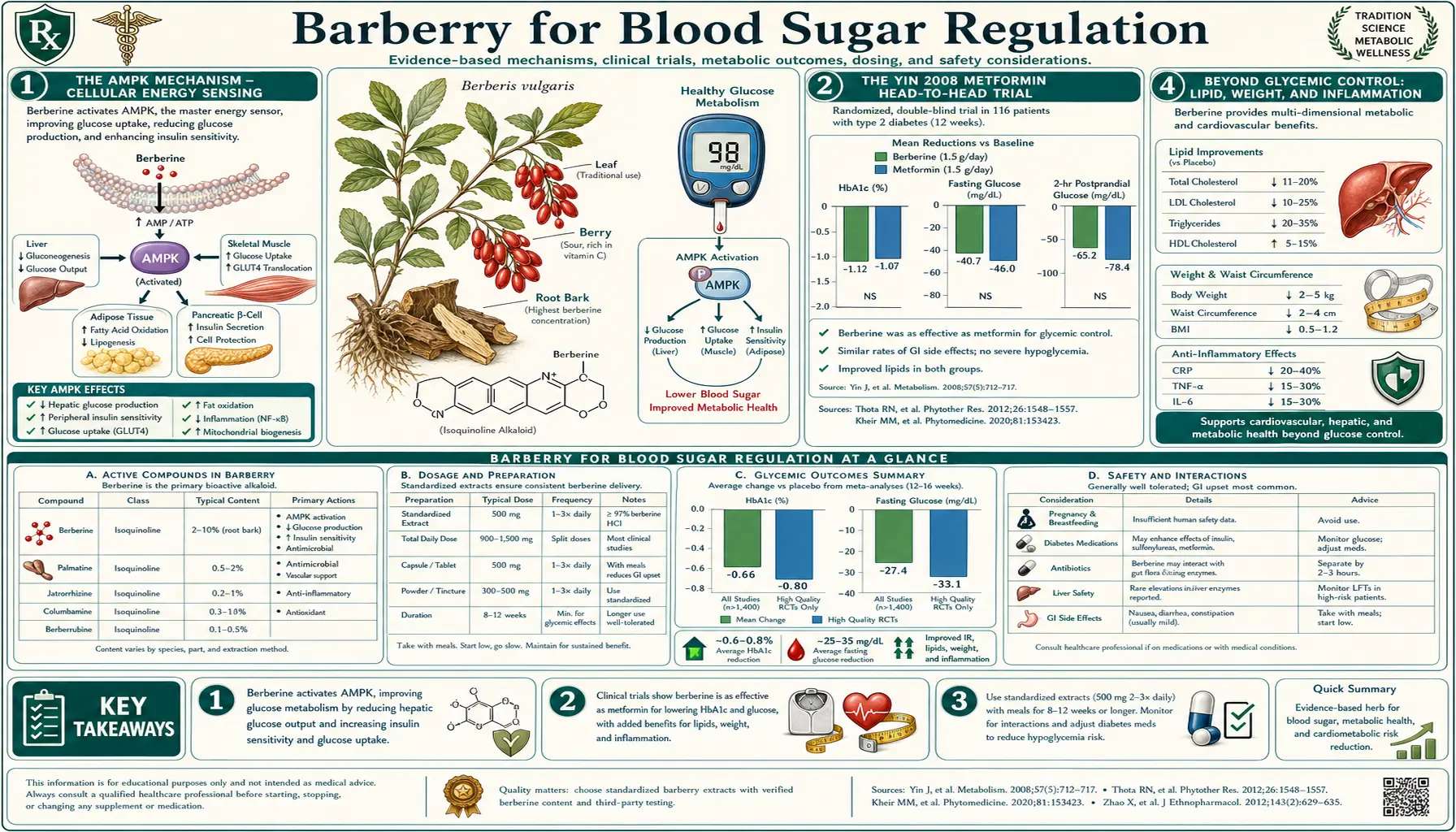
The AMPK Mechanism — Cellular Energy Sensing
AMP-activated protein kinase (AMPK) is the cellular "fuel gauge" — a heterotrimeric serine-threonine kinase that monitors the ratio of AMP to ATP (and ADP to ATP) and activates when energy is low. When activated, AMPK phosphorylates dozens of downstream substrates that collectively shift cellular metabolism from energy-consuming biosynthesis (lipogenesis, gluconeogenesis, protein synthesis) toward energy-producing catabolism (fatty acid oxidation, glucose uptake, glycolysis, mitochondrial biogenesis). It is the master switch that translates "cellular energy state" into "metabolic mode."
Berberine activates AMPK through multiple converging mechanisms:
- Mitochondrial complex I inhibition — berberine, like metformin, weakly inhibits complex I of the electron transport chain. The inhibition reduces ATP synthesis, which increases the cellular AMP:ATP ratio, which directly activates AMPK. This is the dominant mechanism shared with metformin and explains the near-identical glycemic effects.
- Direct AMPK kinase domain interaction — some evidence suggests berberine may also bind to the AMPK kinase domain itself, enhancing activation independent of the AMP:ATP ratio.
- LKB1 upstream activation — berberine may activate LKB1, the upstream kinase that phosphorylates and activates AMPK directly.
Once activated, AMPK produces the following metabolically relevant effects:
- Inhibits hepatic gluconeogenesis — AMPK phosphorylates and inactivates the transcriptional coactivators (CRTC2, FOXO1) that drive transcription of the gluconeogenic enzymes PEPCK and G6Pase. Less gluconeogenesis means less hepatic glucose output, which is the primary mechanism by which both metformin and berberine reduce fasting glucose.
- Enhances GLUT4 translocation in skeletal muscle and adipose tissue — AMPK promotes movement of the GLUT4 glucose transporter from intracellular vesicles to the plasma membrane, increasing insulin-independent glucose uptake. This contributes to postprandial glucose lowering.
- Suppresses lipogenesis — AMPK inhibits acetyl-CoA carboxylase (ACC), the rate-limiting enzyme in fatty acid synthesis, reducing hepatic lipogenesis and de novo lipid synthesis. This is the mechanism behind berberine's hepatic triglyceride reduction and NAFLD improvement.
- Promotes fatty acid oxidation — ACC inhibition reduces malonyl-CoA, which removes the inhibition on CPT1 (carnitine palmitoyltransferase 1), the gateway enzyme for fatty acid entry into mitochondria. Net result: increased fatty acid beta-oxidation.
- Inhibits mTOR signaling — AMPK inhibits the mTOR pathway, reducing protein synthesis and cellular proliferation. This is the mechanism behind the longevity-research interest in both metformin and berberine and the proposed anti-tumor effects of berberine in some cancer models.
The convergence on AMPK explains why berberine and metformin produce such similar clinical effects despite their structural differences — they are essentially two different keys that turn the same lock. It also explains why combining them does not produce additive benefit at maximal doses: both are already pushing the same upstream pathway to near-saturation.
The Yin 2008 Metformin Head-to-Head Trial
The 2008 trial by Yin, Xing, and Ye published in Metabolism remains the single most influential piece of clinical evidence for berberine in type 2 diabetes. The trial was a 3-month, randomized, parallel-group comparison conducted at Beijing Capital Medical University:
- Participants: 36 newly diagnosed adult type 2 diabetics, HbA1c 7.0-11.0%, BMI 22-35
- Intervention arms: berberine 500 mg three times daily with meals, or metformin 500 mg three times daily with meals
- Duration: 13 weeks
- Primary endpoints: HbA1c, fasting plasma glucose, postprandial plasma glucose
The results were striking. Both groups achieved statistically equivalent and clinically meaningful improvements:
- HbA1c — berberine group: 9.5% → 7.5% (-2.0%); metformin group: 9.4% → 7.6% (-1.8%)
- Fasting plasma glucose — berberine: 191 → 124 mg/dL (-67 mg/dL); metformin: 184 → 130 mg/dL (-54 mg/dL)
- Postprandial plasma glucose — berberine: 357 → 200 mg/dL (-157 mg/dL); metformin: 348 → 213 mg/dL (-135 mg/dL)
- HOMA-IR (insulin resistance) — significant reduction in both arms with no difference between them
Both groups also experienced reductions in triglycerides and LDL cholesterol, with berberine producing a numerically larger reduction in triglycerides (Yin's data showed -73 mg/dL on berberine vs -32 mg/dL on metformin, p<0.05). This lipid effect is one of the key differences between the two and the basis of berberine's emerging role in mixed dyslipidemia.
The companion arm of the trial also included 48 patients on existing diabetes medications (metformin and/or sulfonylureas) who added berberine 500 mg three times daily to their existing regimen for 12 weeks. The add-on arm showed further HbA1c reduction of approximately 0.9%, indicating that berberine added to existing antidiabetic therapy produces meaningful additional benefit.
Safety findings:
- The most common adverse effect in the berberine group was transient GI symptoms (mild diarrhea, abdominal distention, constipation), occurring in 34% of participants and typically resolving within 1-2 weeks of continued dosing
- The metformin group had a similar rate of GI side effects (approximately 30%)
- No clinically significant changes in liver function, kidney function, or hematology in either group
- No hypoglycemic events in either group when used as monotherapy
The Yin trial was a small phase-II-style study and has limitations — modest sample size, single-center design, Chinese population only, no placebo arm, no long-term follow-up — but the magnitude of the glycemic effect and its near-perfect parallel with metformin made it an immediate landmark in botanical pharmacology. Subsequent larger trials and meta-analyses have largely confirmed the basic finding.
Subsequent Meta-Analyses and Confirmatory Trials
Several subsequent meta-analyses have synthesized the growing berberine-in-diabetes literature:
- Dong et al. 2012 (Evidence-Based Complementary and Alternative Medicine) — pooled 14 RCTs with 1,068 participants. Berberine reduced HbA1c by 0.71%, fasting glucose by 25 mg/dL, and postprandial glucose by 33 mg/dL versus control. Effects were comparable to metformin and superior to lifestyle intervention alone.
- Lan et al. 2015 (Journal of Ethnopharmacology) — pooled 27 RCTs, 2,569 participants. Berberine demonstrated comparable glycemic efficacy to metformin, glipizide, and rosiglitazone with a more favorable lipid profile. Some studies also showed weight reduction not seen with sulfonylureas.
- Liang et al. 2019 (Journal of Diabetes Investigation) — pooled 46 RCTs, 4,158 participants. Confirmed the consistent glycemic and lipid benefits and refined the picture: berberine monotherapy is comparable to metformin monotherapy; berberine added to metformin produces additional 0.5-0.8% HbA1c reduction; combination outperforms either alone.
- Yang et al. 2022 (Phytotherapy Research) — the most recent comprehensive meta-analysis. Confirmed approximately 1.0% HbA1c reduction with berberine, with the largest effects in patients with worse baseline control (HbA1c >8.5%).
The consistency across multiple meta-analyses, multiple ethnic populations (China, India, Iran, smaller Western trials), and multiple study designs makes the glycemic efficacy of berberine one of the better-established findings in the entire botanical-cardiometabolic literature. The remaining limitations: most studies are Chinese, the longest follow-up periods are typically 3-6 months, and there is no large multi-year cardiovascular outcomes trial comparable to the UKPDS or LEADER trials for conventional diabetes drugs.
Beyond Glycemic Control: Lipid, Weight, and Inflammation
Berberine's clinical interest extends well beyond pure glycemic control. The AMPK / lipogenesis pathway means berberine has direct effects on lipid metabolism, and the LDL receptor upregulation mechanism described by Kong et al. (Nature Medicine 2004) gives it a meaningful cholesterol-lowering effect that is mechanistically distinct from statins.
Lipid effects. Across the meta-analyses, berberine produces:
- LDL cholesterol reduction of approximately 25-30 mg/dL (similar to a moderate-intensity statin)
- Total cholesterol reduction of approximately 20-30 mg/dL
- Triglyceride reduction of approximately 40-50 mg/dL (often larger than statins; this is a key differentiator)
- Modest HDL cholesterol increase (typically 2-5 mg/dL)
The mechanism differs from statins: statins inhibit hepatic HMG-CoA reductase, reducing cholesterol synthesis upstream and indirectly upregulating LDL receptor expression. Berberine directly upregulates hepatic LDL receptor expression through a JNK/ERK-mediated pathway, without affecting HMG-CoA reductase. Because the two mechanisms are upstream and downstream rather than parallel, statin + berberine combinations are additive rather than redundant, and can sometimes achieve LDL targets that monotherapy cannot.
Weight effects. Modest but consistent. Most trials show 2-5 kg weight reduction over 12-24 weeks of berberine therapy, with the largest effects in patients with elevated baseline BMI. The weight loss appears to be related to the AMPK effects on adipose tissue, the suppression of lipogenesis, and possibly the gut microbiome effects (see the Antimicrobial deep-dive).
Inflammation. Berberine reduces hsCRP, IL-6, TNF-alpha, and other systemic inflammation markers in metabolic syndrome populations. The mechanism is partly direct (NF-κB pathway inhibition) and partly secondary to the improved glycemic and lipid status.
Blood pressure. Modest reduction (typically 5-10 mmHg systolic) through endothelial-dependent vasodilation and reduced sympathetic tone.
The collective picture is that berberine is a true multi-target cardiometabolic agent — not just a glucose-lowering drug. This is why it is increasingly used in metabolic syndrome and prediabetes settings where the goal is not pure glycemic control but global cardiometabolic risk reduction.
Barberry vs Standardized Berberine — Dose Equivalence
An important practical point that is often confused: the impressive clinical data on "berberine" for blood sugar refers almost entirely to standardized berberine HCl supplements at 500 mg three times daily. This is approximately 1,500 mg of pure berberine per day. Modern berberine supplements are almost never extracted from Berberis vulgaris (barberry) — they are extracted from Coptis chinensis (Chinese goldthread, yielding 5-7% berberine by weight) or Phellodendron amurense (Amur cork tree, yielding 3-5% berberine).
The dose-equivalence calculation for barberry root:
- Standardized berberine target dose: 1,500 mg/day
- Barberry root berberine content: approximately 2-3% (so 20-30 mg berberine per gram of dried root)
- Barberry root needed to deliver 1,500 mg berberine: 50-75 g/day
Fifty to seventy-five grams of dried barberry root per day is impractical — that is approximately a quarter cup of dried root daily. Even at the upper end of traditional tincture dosing (4-6 mL of 1:5 tincture, 3×/day, equivalent to approximately 12-18 mL/day), the berberine delivery is only 240-360 mg/day, less than a quarter of the cardiometabolic target dose.
Practical implication: if the goal is the documented cardiometabolic benefit of berberine for type 2 diabetes, prediabetes, NAFLD, or mixed dyslipidemia, use a standardized berberine HCl supplement (extracted from Coptis or Phellodendron). The whole-herb barberry preparation is appropriate for its traditional indications (digestive bitter, cholagogue, mild antimicrobial) but cannot deliver enough berberine for the metabolic indications.
That said, low-dose barberry preparations (decoction or tincture in traditional bitter-tonic doses) do produce some glycemic benefit. The cephalic-phase bitter effect of the alkaloids on the tongue, before any absorption, triggers vagal-mediated increases in insulin sensitivity that are modest but real. For patients who do not want a "supplement" but want some mild glycemic support alongside the digestive effect, barberry tincture pre-meals (40-60 drops, 15 minutes before eating) produces a measurable but modest reduction in postprandial glucose excursion. This is similar to the effect produced by gentian, dandelion, and other bitter herbs through the same vagal cephalic-phase mechanism.
For the full data on standardized berberine including the bioavailability strategies, dosing protocols, and combination protocols, see the Berberine Benefits deep-dive.
The Bioavailability Problem and Modern Solutions
The major pharmacokinetic challenge with berberine is its remarkably poor oral bioavailability — typically less than 1% of an oral dose appears as unchanged berberine in systemic circulation. Three mechanisms combine to limit systemic absorption:
- Self-aggregation in the GI lumen — berberine readily forms cation-anion complexes with bile acids, fatty acids, and other GI contents, reducing the dissolved monomer fraction available for absorption.
- P-glycoprotein efflux — berberine is a P-gp substrate. The P-gp pump in enterocytes actively expels berberine back into the gut lumen, capping absorption.
- Rapid first-pass metabolism — the small fraction that does reach the portal circulation is rapidly metabolized by hepatic CYP2D6 and other enzymes to berberrubine and other less-active metabolites.
Several strategies are used to improve bioavailability:
- Silymarin co-administration — silymarin (the standardized extract of milk thistle, see our Milk Thistle page) inhibits P-gp efflux. Several trials show that combining berberine with silymarin (approximately 100-200 mg silymarin per 500 mg berberine) approximately doubles berberine systemic exposure and produces clinically meaningful improvement in efficacy.
- Piperine co-administration — piperine from black pepper inhibits CYP3A4 first-pass metabolism. Less well-studied than silymarin in the berberine context but used in some commercial formulations.
- Phytosome / liposomal formulations — encapsulating berberine in phospholipid carriers improves absorption by 2-5× in pharmacokinetic studies. Several commercial products use this approach.
- Dihydroberberine — the reduced form of berberine (see next section).
Dihydroberberine — the Next-Generation Form
Dihydroberberine is the reduced (di-hydrogen-added) form of berberine. The reduction is reversible and occurs naturally in vivo by gut bacterial nitroreductase activity — dihydroberberine is actually one of the bacterially generated berberine metabolites in the human gut. Supplementing the reduced form directly has several pharmacokinetic advantages:
- Better intestinal absorption — dihydroberberine is approximately 5× more bioavailable than berberine HCl. The added hydrogens reduce the quaternary nitrogen's interaction with P-gp efflux pumps.
- Re-oxidation to berberine in vivo — once absorbed, dihydroberberine is partly re-oxidized back to active berberine, providing sustained delivery.
- Lower dose requirement — the typical dihydroberberine dose is 100-150 mg twice daily (versus 500 mg three times daily for standard berberine HCl), with similar clinical efficacy.
- Better GI tolerability — the lower total dose reduces GI side effects (constipation, abdominal cramping).
Dihydroberberine is now available as a commercial supplement (often marketed under the brand name GlucoVantage and similar). Cost is somewhat higher per dose than standard berberine HCl, but the lower required dose and better tolerability often justify the price difference for patients with sensitive GI tracts. The clinical efficacy data for dihydroberberine is smaller than for standard berberine HCl but consistent.
Prediabetes and Reversal of Insulin Resistance
Prediabetes — defined as HbA1c 5.7-6.4% or fasting glucose 100-125 mg/dL or 2-hour OGTT glucose 140-199 mg/dL — affects approximately 100 million American adults. Approximately 30% of prediabetics progress to overt type 2 diabetes within 5 years without intervention. The Diabetes Prevention Program established that intensive lifestyle change (7% weight loss + 150 minutes/week moderate exercise) reduces progression risk by approximately 58%, and metformin 850 mg twice daily reduces progression risk by approximately 31%.
Berberine has not been formally tested in a DPP-equivalent prediabetes prevention trial, but multiple smaller studies suggest it is at least as effective as metformin for progression prevention. The Yin trial included some patients in the prediabetic range and showed normalization of HbA1c and HOMA-IR. Several Chinese studies in prediabetic populations have shown improved insulin sensitivity, reduced fasting glucose, and normalization of postprandial glucose excursions.
The practical prediabetes protocol typically combines:
- Berberine HCl 500 mg three times daily with meals (or dihydroberberine 150 mg twice daily) — the cardiometabolic core
- Lifestyle modification including reduced refined carbohydrate, increased physical activity, and weight optimization
- Continuous glucose monitor (CGM) use to identify which foods and meals cause the largest individual glucose excursions and to confirm the intervention is working — see our CGM page
- Periodic HbA1c monitoring (every 3-6 months) and fasting insulin / HOMA-IR (every 6-12 months)
For more on insulin resistance specifically, see our Insulin Resistance page.
Polycystic Ovary Syndrome (PCOS) Applications
Polycystic ovary syndrome affects 5-10% of reproductive-age women and is fundamentally an insulin-resistance disorder with downstream hyperandrogenic and ovulatory consequences. Metformin has been a mainstay of PCOS therapy for decades, with documented benefit for menstrual regularity, ovulation, hirsutism, and metabolic parameters. Berberine has been studied as a metformin-equivalent in PCOS with results that broadly parallel the type 2 diabetes findings.
The most informative PCOS-specific trial is Wei et al. 2012 (European Journal of Endocrinology), which randomized 89 overweight PCOS patients to one of three arms: berberine 500 mg three times daily, metformin 1500 mg/day, or placebo, for 3 months. Results:
- HOMA-IR and insulin levels: berberine and metformin both significantly reduced versus placebo, with no significant difference between the two active arms
- Waist-to-hip ratio: berberine outperformed metformin (greater reduction), p<0.05
- Lipid profile: berberine outperformed metformin (greater total cholesterol and triglyceride reduction, greater HDL increase)
- Total testosterone and free androgen index: both active arms reduced versus placebo
- SHBG (sex hormone binding globulin): increased in both active arms, indicating reduced bioavailable androgen
Subsequent PCOS trials have replicated the basic findings and added evidence for improved ovulation rates and pregnancy outcomes in berberine-treated subfertile PCOS patients. Berberine is now considered a reasonable alternative to metformin for PCOS, particularly for patients who do not tolerate metformin's GI side effects or for whom the lipid benefit is clinically important.
Metabolic Syndrome and NAFLD Connection
Metabolic syndrome is defined by the simultaneous presence of three or more of: central obesity, hypertension, dyslipidemia (elevated triglycerides, low HDL), elevated fasting glucose, and insulin resistance. Non-alcoholic fatty liver disease (NAFLD) is the hepatic manifestation of metabolic syndrome and is now the most common chronic liver disease in the developed world.
Berberine's multi-target cardiometabolic profile makes it well-suited to metabolic syndrome treatment because it simultaneously addresses several of the diagnostic components:
- Insulin resistance: AMPK activation, HOMA-IR improvement
- Glycemic control: HbA1c, fasting glucose, postprandial glucose
- Dyslipidemia: LDL receptor upregulation, triglyceride reduction
- Central obesity: modest but consistent weight reduction
- NAFLD: hepatic steatosis reduction (covered in detail on the Liver Health deep-dive)
- Inflammation: hsCRP, IL-6, TNF-alpha reduction
For metabolic syndrome treatment, the practical protocol combines berberine (500 mg three times daily, or dihydroberberine 150 mg twice daily) with comprehensive lifestyle modification — carbohydrate restriction, increased physical activity, weight optimization, sleep optimization, and stress management. Berberine is best thought of as a metabolic accelerant rather than a stand-alone therapy — it works best when combined with lifestyle change rather than as a substitute for it.
Combining Berberine with Metformin or Other Antidiabetics
A common clinical question is whether berberine adds benefit when combined with metformin. The Yin trial's add-on arm showed approximately 0.9% additional HbA1c reduction with berberine added to existing antidiabetic regimens. Subsequent meta-analyses confirm modest but real additive benefit when berberine is combined with metformin, sulfonylureas, or insulin.
The mechanism for the additive effect is not entirely clear — given that both berberine and metformin activate AMPK through the same upstream mitochondrial complex I mechanism, one might predict redundancy rather than additivity. Possible explanations include:
- Berberine has AMPK-independent glucose-lowering mechanisms (LDL receptor upregulation does not affect glucose but the same berberine molecule may have other distinct effects)
- The dosing of metformin and berberine in real clinical practice often leaves AMPK below saturation, leaving room for additional pharmacologic push
- The lipid effects of berberine are largely independent of metformin and add cardiovascular benefit even when glycemic effects are saturated
For patients on metformin who have not reached HbA1c goal, adding berberine 500 mg three times daily is a reasonable next step — often more cost-effective and better tolerated than escalating to a sulfonylurea or DPP-4 inhibitor. The combination requires careful glucose monitoring during the first 2-4 weeks to avoid hypoglycemia, and downward titration of insulin or sulfonylurea doses is sometimes needed as the combination's full effect emerges.
Practical Dosing Protocols
Standardized berberine HCl (the cardiometabolic protocol).
- Starting dose: 500 mg with the largest meal of the day, for 1 week (allows GI adaptation)
- Week 2: 500 mg twice daily with meals
- Week 3 onward: 500 mg three times daily with meals (total 1,500 mg/day)
- Take with food to reduce GI side effects and to take advantage of the cephalic-phase digestive bitter effect
- Expect onset of glycemic improvement within 2-4 weeks; full effect by 12 weeks
- Monitor with periodic HbA1c every 3 months and fasting insulin every 6 months
Dihydroberberine.
- 100-150 mg twice daily with meals
- Equivalent glycemic effect to standard berberine HCl at much lower total dose
- Better tolerated GI-wise, useful for patients who could not tolerate standard berberine
Barberry tincture (mild adjunct dose).
- 40-60 drops (2-3 mL) of 1:5 tincture in water, 15 minutes before each meal
- Provides bitter cephalic-phase effect plus modest berberine systemic delivery
- Not a substitute for standardized berberine for diabetes; appropriate for prediabetes adjunct or for digestive symptom management
Combination considerations.
- Berberine + silymarin (200 mg silymarin per 500 mg berberine) — doubles bioavailability
- Berberine + alpha-lipoic acid (300-600 mg ALA) — additive insulin-sensitizing effect
- Berberine + cinnamon (1-2 g Ceylon cinnamon) — complementary mechanisms (cinnamon affects insulin receptor activation)
- Berberine + magnesium (200-400 mg, glycinate or malate) — magnesium is depleted in insulin resistance and synergizes glycemic improvement
Cautions and Drug Interactions
- Pregnancy and breastfeeding (contraindicated) — berberine crosses the placenta and displaces bilirubin from albumin, risking kernicterus in newborns. Avoid in pregnancy and breastfeeding.
- Hypoglycemia in patients on multiple antidiabetics — berberine added to insulin, sulfonylureas, or meglitinides can produce hypoglycemia. Glucose monitoring is essential, and downward titration of the existing antidiabetics is often required.
- CYP3A4 and P-gp inhibition — berberine inhibits CYP3A4 and P-glycoprotein, with potential for significant interaction with cyclosporine, tacrolimus, statins (atorvastatin, simvastatin, lovastatin), and many other prescription drugs. Pharmacist review is recommended before starting chronic berberine in polypharmacy patients.
- GI side effects — the most common adverse effect. Constipation in some patients, diarrhea in others, occasionally bitter or metallic taste. Splitting the dose, taking with food, or stepping down the dose typically resolves the symptom. Switching to dihydroberberine is an option for persistent intolerance.
- Anticoagulants — potential for warfarin potentiation. INR monitoring is required.
- Hypotension — mild blood pressure reduction may augment antihypertensives.
- Long-term use — safety data on continuous berberine use beyond 12-24 months in humans is limited. Most clinicians recommend periodic 2-4 week "drug holidays" every 6 months, though this is empirical rather than evidence-based.
Key Research Papers
- Yin J, Xing H, Ye J (2008). Efficacy of berberine in patients with type 2 diabetes mellitus. Metabolism. — PubMed
- Kong W et al. (2004). Berberine is a novel cholesterol-lowering drug working through a unique mechanism distinct from statins. Nature Medicine. — PubMed
- Lee YS et al. (2006). Berberine, a natural plant product, activates AMP-activated protein kinase with beneficial metabolic effects in diabetic and insulin-resistant states. Diabetes. — the foundational AMPK mechanism paper. PubMed
- Dong H et al. (2012). Berberine in the treatment of type 2 diabetes mellitus: A systemic review and meta-analysis. Evidence-Based Complementary and Alternative Medicine. — PubMed
- Lan J et al. (2015). Meta-analysis of the effect and safety of berberine in the treatment of type 2 diabetes mellitus. Journal of Ethnopharmacology. — PubMed
- Liang Y et al. (2019). Effects of berberine on blood glucose in patients with type 2 diabetes mellitus: a systematic literature review and meta-analysis. Journal of Diabetes Investigation. — PubMed
- Wei W et al. (2012). A clinical study on the short-term effect of berberine in comparison to metformin on the metabolic characteristics of women with polycystic ovary syndrome. European Journal of Endocrinology. — PubMed
- Pirillo A, Catapano AL (2015). Berberine, a plant alkaloid with lipid- and glucose-lowering properties: From in vitro evidence to clinical studies. Atherosclerosis. — comprehensive lipid mechanism review. PubMed
- Cicero AFG, Baggioni A (2016). Berberine and its role in chronic disease. Advances in Experimental Medicine and Biology. — comprehensive cardiometabolic review. PubMed
- Zhang H et al. (2010). Berberine lowers blood glucose in type 2 diabetes mellitus patients through increasing insulin receptor expression. Metabolism. — insulin receptor mechanism. PubMed
- Di Pierro F et al. (2012). Pilot study on the additive effects of berberine and oral type 2 diabetes agents for patients with suboptimal glycemic control. Diabetes, Metabolic Syndrome and Obesity. — the silymarin co-administration / add-on study. PubMed
- Turner N et al. (2008). Berberine and its more biologically available derivative, dihydroberberine, inhibit mitochondrial respiratory complex I. Diabetes. — the dihydroberberine bioavailability foundation. PubMed
PubMed Topic Searches
- PubMed: Berberine type 2 diabetes HbA1c
- PubMed: Berberine AMPK glucose
- PubMed: Berberine vs metformin comparison
- PubMed: Berberine LDL receptor
- PubMed: Berberine PCOS
- PubMed: Dihydroberberine bioavailability
Connections
- Barberry Overview
- Barberry Benefits Hub
- Barberry for Antimicrobial Action
- Barberry for Liver Health
- Barberry as a Digestive Aid
- Berberine (Standardized Supplement)
- Berberine Benefits Deep Dive
- Milk Thistle (Silymarin Bioavailability Booster)
- Diabetes
- Insulin Resistance
- Metformin, Berberine, and GLP-1s
- Polycystic Ovary Syndrome
- Blood Sugar
- Continuous Glucose Monitor (CGM)
- Hemoglobin A1C
- Magnesium
- All Herbs
- Metformin — the biguanide that shares the same complex I and AMPK mechanism as berberine and served as the comparator arm in the Yin 2008 trial.