Barberry for Antimicrobial Action
Barberry root contains 2-3% berberine by dry weight, the bright-yellow isoquinoline alkaloid responsible for nearly all of its broad-spectrum antimicrobial activity. Berberine kills or inhibits a remarkably wide range of pathogens — gram-positive and gram-negative bacteria, mycobacteria, fungi, protozoa (Giardia, Entamoeba, Leishmania, Trypanosoma), and several viruses — through at least four distinct molecular mechanisms simultaneously, making single-mutation resistance nearly impossible to develop. The landmark Khin-Maung-U 1985 trial in Bangladesh established 400 mg berberine sulfate as clinically effective against cholera and enterotoxigenic E. coli dysentery in a controlled inpatient setting. This page covers the mechanism, the pivotal clinical evidence, how barberry compares with its alkaloid-sibling goldenseal, and the practical role of barberry root preparations in giardiasis, traveler's diarrhea, urinary tract infection, skin and mucosal infection, and the question of post-antibiotic gut recolonization.
Table of Contents
- Historical Background — Persian and European Use
- Berberine's Four-Pronged Antimicrobial Mechanism
- The Antimicrobial Spectrum of Barberry / Berberine
- The Khin-Maung-U 1985 Cholera and E. coli Trial
- Barberry vs Goldenseal — the NorA Efflux Pump Question
- Giardiasis and Other Protozoal Infection
- Traveler's Diarrhea and Acute Gastroenteritis
- Urinary Tract Infections
- Skin, Eye, and Mucosal Infection
- Effect on the Commensal Gut Microbiome
- Dosing and Practical Forms (Decoction, Tincture, Capsule)
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
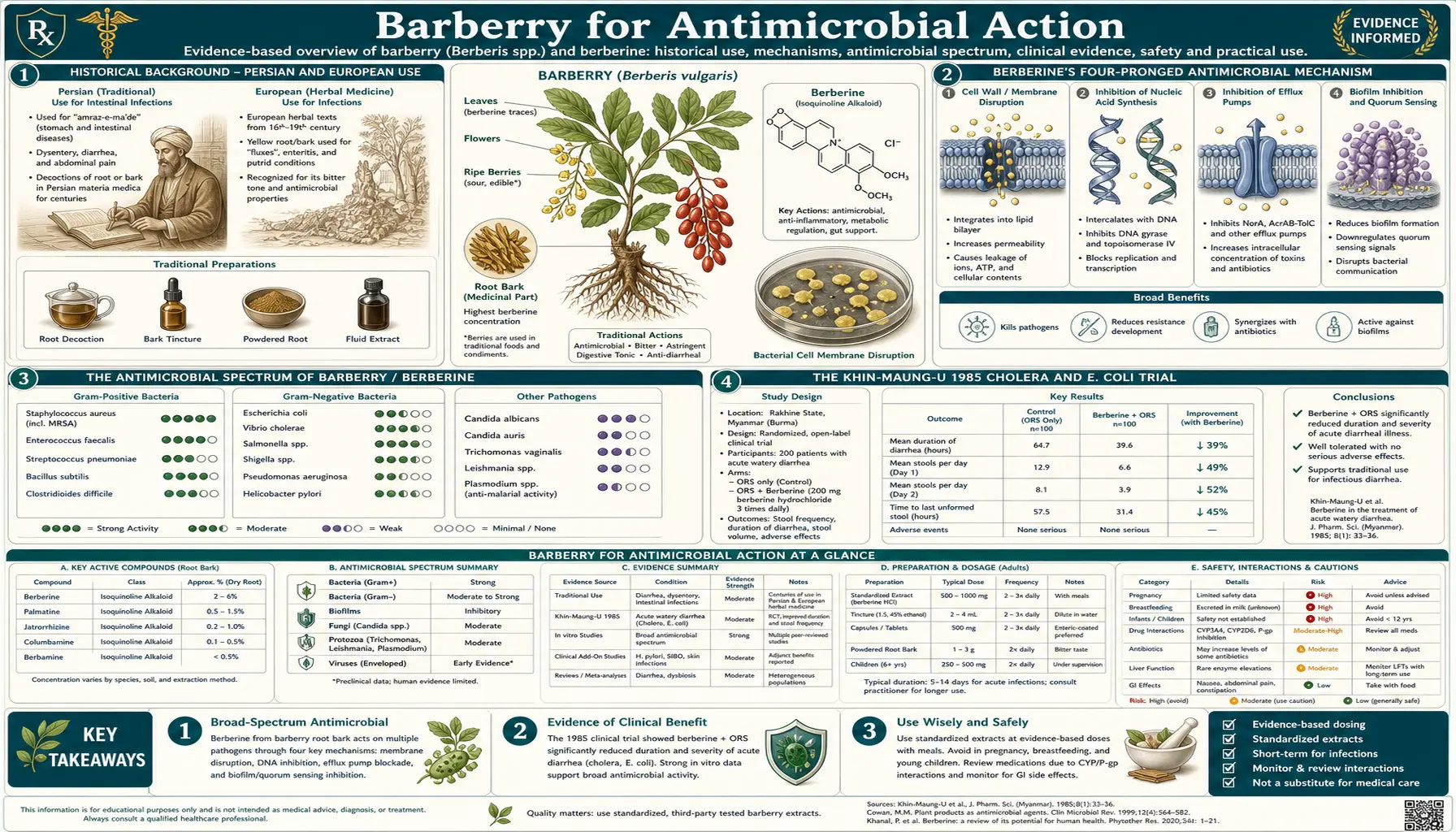
Historical Background — Persian and European Use
The medicinal use of barberry is at least 3,000 years old. Cuneiform tablets from the library of Ashurbanipal (7th century BCE) describe barberry preparations used to "purify the blood" in fever, a description consistent with modern understanding of antimicrobial action against bloodstream and enteric infection. Persian medicine integrated barberry as zereshk root for hepatitis, jaundice, and dysentery, and the dried red berries (also called zereshk) became and remain a staple of Persian cuisine, classically scattered over saffron rice in zereshk polo. The medicinal use of the berry is much milder than the root because berberine is concentrated in the inner bark and root tissue, not the fruit.
Greek and Roman herbalists including Dioscorides (1st century CE) described barberry-like preparations for diarrhea and "rotting" mucosal conditions. European medieval and early modern herbalists used barberry root bark in tinctures for jaundice, malaria, and dysentery. The herb was sufficiently important that an English statute in 1660 required eradication of barberry bushes within a certain distance of grain fields because they were correctly identified as the alternate host of the wheat rust fungus (Puccinia graminis) — an early example of plant-pathology epidemiology that has nothing to do with herbal medicine but illustrates the historical ubiquity of the plant.
Native American use of the closely related Berberis aquifolium (Oregon grape) and Berberis canadensis overlapped considerably with Eclectic and Physiomedical use in the 19th century United States. The Eclectic Materia Medica of John King and Harvey Wickes Felter described barberry root as a "stomachic, tonic, and laxative" with particular value in "jaundice, hepatic torpor, indigestion, and chronic dyspepsia" — indications that align well with modern understanding of berberine's cholagogue, AMPK, and antimicrobial actions.
The isolation of berberine itself dates to 1837 (independently by Buchner & Herberger in Germany and Hayman in England, working from Xanthoxylum clava-herculis and other source plants). The compound was named for the Berberis genus where it had first been characterized chemically. The structural assignment as a quaternary ammonium isoquinoline alkaloid was completed in the early 20th century. The mechanism of antimicrobial action was first explored in mid-20th-century pharmacology and progressively elaborated through the 1980s clinical trials and subsequent molecular biology work.
Berberine's Four-Pronged Antimicrobial Mechanism
One of the reasons berberine has retained clinical interest while many other plant antimicrobials have faded is that it works through multiple simultaneous mechanisms, none of which are vulnerable to single-point resistance mutations. The four major mechanisms:
- DNA intercalation and topoisomerase inhibition — the planar tetracyclic aromatic structure of berberine slides between the stacked base pairs of double-stranded DNA, distorting the helix and preventing the action of bacterial topoisomerases. The intercalation is preferential for GC-rich regions. The functional effect is inhibition of bacterial DNA replication and transcription — the same general target class as the fluoroquinolone antibiotics, though by a different specific mechanism.
- FtsZ inhibition (blocks cell division) — FtsZ is the bacterial cell-division protein that polymerizes at the future division site (the Z-ring) and recruits the cell-wall synthesis machinery needed to construct the dividing septum. Berberine binds FtsZ and prevents Z-ring assembly, blocking cell division. The bacteria continue to grow as long filaments without dividing, eventually losing membrane integrity. FtsZ has no eukaryotic homolog (animal cell division uses actin/myosin), so the mechanism is selective for bacteria.
- Membrane disruption at higher concentrations — the quaternary nitrogen of berberine carries a permanent positive charge, allowing it to associate with negatively charged bacterial membrane phospholipids (cardiolipin and phosphatidylglycerol in particular, both more abundant in bacterial than mammalian membranes). At concentrations above approximately 50-100 µg/mL, this causes membrane depolarization and increased permeability.
- Inhibition of microbial adhesion — berberine downregulates expression and assembly of bacterial adhesins including type I fimbriae and the FimH adhesin (which mediates E. coli adhesion to bladder uroepithelium), reducing the ability of pathogens to colonize mucosal surfaces in the first place. This is particularly relevant in urinary tract infection prevention.
The combination is synergistic: a bacterium that mutated to evade DNA intercalation would still face FtsZ inhibition and adhesion blockade. The closest pharmaceutical analog is the multi-target antibiotic combinations used in tuberculosis therapy — combining drugs with different mechanisms specifically to prevent resistance emergence. Berberine delivers something approximating that effect in a single molecule.
The flip side is that the multi-target mechanism limits potency at any single target. Berberine's minimum inhibitory concentrations (MICs) are generally in the 25-200 µg/mL range for clinically relevant bacteria — 100-1000× less potent on a weight basis than a frontline antibiotic such as ciprofloxacin. The clinical effectiveness depends on achieving sufficient local concentration at the site of infection, which is easy in the gut lumen (where ingested berberine sees concentrations in the hundreds of µg/mL because absorption is so low) and on the skin or mucosal surface (where topical concentration can be even higher), but harder in systemic infection where plasma berberine after oral dosing typically peaks at 1-10 ng/mL.
The Antimicrobial Spectrum of Barberry / Berberine
Berberine has documented in vitro activity against an unusually broad range of pathogens. The following is a representative selection from the published MIC literature, organized by target class:
Gram-positive bacteria. Staphylococcus aureus (including methicillin-resistant MRSA), Staphylococcus epidermidis, Streptococcus pyogenes, Streptococcus pneumoniae, Enterococcus faecalis, Bacillus subtilis, Listeria monocytogenes. MICs typically 25-100 µg/mL. Gram-positive activity is generally stronger than gram-negative because the lipopolysaccharide outer membrane of gram-negatives slows berberine penetration.
Gram-negative bacteria. Escherichia coli (including enterotoxigenic ETEC and enteroinvasive EIEC strains), Vibrio cholerae, Salmonella enterica, Shigella dysenteriae, Klebsiella pneumoniae, Pseudomonas aeruginosa, Helicobacter pylori, Yersinia enterocolitica. MICs typically 50-200 µg/mL. The intraluminal gut concentrations achieved with oral barberry or berberine are easily sufficient to be bactericidal against these pathogens at the site of infection.
Mycobacteria. Mycobacterium tuberculosis shows modest in vitro susceptibility (MIC around 200 µg/mL); the limited in vivo absorption makes berberine impractical as a TB therapy in modern practice, though it has been used adjunctively in resource-limited settings.
Fungi. Candida albicans (including some azole-resistant strains), Candida glabrata, Candida tropicalis, several dermatophytes including Trichophyton rubrum (athlete's foot) and Microsporum canis. Topical barberry preparations have demonstrated clinical utility in superficial fungal infection.
Protozoa. Giardia lamblia (extensive clinical data — see below), Entamoeba histolytica, Leishmania donovani, Trypanosoma brucei, Trichomonas vaginalis. The protozoal activity is particularly clinically useful because conventional protozoal therapy (metronidazole, tinidazole, paromomycin) often has GI side effects, and berberine offers a relatively well-tolerated alternative.
Viruses. Modest in vitro activity against herpes simplex virus, influenza A, hepatitis B and C, and several other enveloped viruses. The clinical relevance is uncertain; berberine is not a primary antiviral agent.
The Khin-Maung-U 1985 Cholera and E. coli Trial
The 1985 Khin-Maung-U et al. trial published in the British Medical Journal remains the single most important piece of clinical evidence for the antibacterial use of berberine. Conducted at the International Centre for Diarrhoeal Disease Research in Bangladesh, the trial randomized 165 adult inpatients with acute culture-confirmed cholera or enterotoxigenic E. coli dysentery to one of four treatment arms:
- Berberine sulfate 400 mg single oral dose
- Tetracycline 500 mg (active control)
- Berberine + tetracycline combination
- Placebo
In the cholera subgroup, berberine alone significantly reduced stool volume by 48% over the first 24 hours compared with placebo. Stool volume in the tetracycline and combination arms was reduced more dramatically (tetracycline is highly effective in cholera by inhibiting bacterial protein synthesis and stopping toxin production), but berberine produced a clinically meaningful reduction independent of antibiotic action. The proposed mechanism for the antitoxin effect: berberine binds directly to cholera toxin B subunit and reduces its association with the gut epithelial GM1 ganglioside receptor, blocking the toxin-driven hypersecretion that causes the watery diarrhea.
In the enterotoxigenic E. coli subgroup, the effect was even more pronounced. Berberine 400 mg single dose reduced stool volume by 77% over the first 24 hours, statistically equivalent to tetracycline, and the duration of diarrhea was also shortened. The proposed mechanism is similar: berberine binds the heat-labile toxin (which is structurally similar to cholera toxin) and reduces its receptor binding.
The trial established several practical conclusions that remain valid today:
- Berberine is clinically effective for acute bacterial diarrhea, particularly when the mechanism is toxin-driven hypersecretion.
- A single oral dose of 400 mg berberine sulfate is sufficient for adult cholera/ETEC indications, with no apparent benefit to multi-dose regimens for this acute use.
- Berberine does not appear to interfere with tetracycline activity; combination therapy was at least as effective as tetracycline alone.
- The safety profile of single-dose berberine at this dose was excellent, with no significant adverse effects observed.
The trial design has limitations from a modern perspective — the sample size was modest, the duration of follow-up was short, and the comparator was tetracycline rather than the now-standard azithromycin or fluoroquinolones — but the magnitude of the observed effect leaves little doubt that berberine is biologically active against bacterial toxin-mediated diarrhea in vivo at clinically achievable doses. This is the foundation of modern phytotherapeutic use of berberine in traveler's diarrhea and the rationale for the WHO traditional medicine listing.
Barberry vs Goldenseal — the NorA Efflux Pump Question
Barberry (Berberis vulgaris) and goldenseal (Hydrastis canadensis) both contain berberine as their primary antimicrobial alkaloid. From a pure-berberine standpoint, the two herbs should be roughly interchangeable, with barberry actually offering a higher berberine yield per gram of crude herb than goldenseal in some growing conditions. In practice, however, goldenseal has earned a reputation as the stronger antimicrobial for certain indications, particularly skin and mucosal infections caused by gram-positive bacteria. The explanation comes down to a single additional alkaloid present in goldenseal but absent in barberry: hydrastine.
Hydrastine is a phthalideisoquinoline alkaloid present at 1.5-4% of dried goldenseal root by weight. In isolation, hydrastine is a weaker antimicrobial than berberine. The clinical significance is that hydrastine inhibits the NorA efflux pump — a bacterial multidrug resistance pump found in Staphylococcus aureus and several other gram-positive species. NorA actively expels berberine (among many other compounds) out of the bacterial cytoplasm, dramatically reducing intracellular berberine concentration and limiting its antimicrobial action.
When goldenseal is used as a whole-herb preparation, hydrastine inhibits NorA, berberine accumulates inside the bacterial cell at much higher concentrations than it could achieve alone, and the combined preparation shows substantially stronger anti-staphylococcal action than either alkaloid alone — or than barberry alone. This is one of the cleanest documented examples of botanical synergy ("entourage effect") in the herbal medicine literature, with quantitative in vitro data and a mechanistic explanation.
Practical implications:
- For acute bacterial diarrhea (cholera, ETEC, dysentery) — barberry and goldenseal are roughly interchangeable. The berberine concentration in the gut lumen is high enough that NorA-mediated efflux is not the rate-limiting factor.
- For skin or topical mucosal staph infection — goldenseal is preferred because the hydrastine/berberine synergy meaningfully boosts anti-staph activity.
- For systemic indications (where overall systemic exposure is the goal, not a particular pathogen) — barberry has the advantage of being far more sustainable and far cheaper than goldenseal (the latter is on the United Plant Savers At-Risk list due to historical overharvesting from wild populations).
- For traditional bitter and cholagogue indications — barberry is the classical European/Persian choice and works as well as goldenseal at much lower cost.
For more on goldenseal specifically, including its hydrastine, canadine, and berberastine alkaloid profile, see our Goldenseal page.
Giardiasis and Other Protozoal Infection
Giardia lamblia (also called G. duodenalis or G. intestinalis) is a flagellated protozoan parasite that colonizes the proximal small intestine and causes chronic diarrhea, malabsorption, abdominal cramping, and the classic "rotten egg" sulfurous flatulence. Standard therapy is metronidazole (250 mg three times daily for 5-7 days) or tinidazole (single 2-gram dose), both of which are highly effective but commonly cause GI side effects including a metallic taste, nausea, and disulfiram-like reactions with alcohol. Resistance is also a growing concern.
Berberine has substantial documented activity against Giardia in vitro and in clinical trials. A 1972 trial in Indian children by Choudry and colleagues randomized 137 children with giardiasis to one of four treatments — metronidazole, furazolidone, berberine 5-10 mg/kg/day in three divided doses, or placebo. The metronidazole arm achieved approximately 95% cure rate, the furazolidone arm 90%, and the berberine arm 68% cure rate. Berberine was less effective than metronidazole but substantially better than placebo, and the side-effect profile was much milder than either of the comparator drugs. Subsequent smaller trials have replicated this general pattern: berberine is a second-line or adjunctive option for giardiasis, useful particularly when conventional therapy is contraindicated, has failed, or is poorly tolerated.
Other protozoal applications:
- Amebiasis (Entamoeba histolytica) — berberine has documented activity, used in traditional Asian medicine. Modern first-line is metronidazole + paromomycin; berberine is an adjunct or alternative when conventional therapy is contraindicated.
- Leishmaniasis (visceral and cutaneous) — berberine derivatives have been explored as leishmaniasis therapies, with some promising in vivo data but no widespread clinical adoption.
- Trichomoniasis — modest in vitro activity, no robust clinical evidence.
- Cryptosporidiosis — some in vitro activity reported; clinical evidence is sparse.
For more on parasite protocols generally, see our Parasites page.
Traveler's Diarrhea and Acute Gastroenteritis
Traveler's diarrhea affects 20-50% of international travelers to high-risk destinations and is most commonly caused by enterotoxigenic E. coli (ETEC), enteroaggregative E. coli (EAEC), Campylobacter jejuni, Salmonella enterica, Shigella, or norovirus. The conventional approach is oral rehydration plus, for moderate to severe symptoms, a fluoroquinolone (rapidly losing efficacy due to Campylobacter resistance) or azithromycin (current preferred frontline for Southeast Asia and the Indian subcontinent).
Berberine has a clear evidence-based role as either a preventive or treatment option for traveler's diarrhea, based on the Khin-Maung-U mechanism (antitoxin binding for ETEC) and the broad antibacterial spectrum that covers most other common causes. Practical dosing for travelers:
- Prevention — 400 mg berberine HCl once or twice daily during travel in high-risk regions. Note: this is the standardized supplement, not barberry crude root; achieving the equivalent berberine dose from barberry root would require approximately 40-50 g daily of dried root, which is impractical.
- Acute treatment at symptom onset — 400-500 mg berberine HCl three to four times daily for 3-5 days, ideally taken at the first onset of loose stool. Often combined with oral rehydration salts.
- Barberry tincture for milder cases — 2-3 mL (40-60 drops) of 1:5 tincture every 2-4 hours during acute symptoms. Less potent than standardized berberine but more accessible in some settings and useful for the bitter / digestive effect alongside the antimicrobial action.
The advantage of berberine over antibiotic prophylaxis is the absence of the resistance-pressure problem, the much lower disruption to the commensal microbiome (see below), and the side-effect profile. The disadvantage is somewhat lower efficacy than azithromycin or rifaximin for severe bacterial diarrhea, and the unfortunate fact that berberine is poorly absorbed and cannot treat systemic infection — if traveler's diarrhea progresses to invasive disease with fever and bloody stools, conventional antibiotics are needed.
Urinary Tract Infections
Acute uncomplicated urinary tract infection in women is most commonly caused by uropathogenic Escherichia coli (UPEC, approximately 80% of cases), with Staphylococcus saprophyticus, Klebsiella, and Proteus mirabilis rounding out the next 15-20%. The classical bladder-infection presentation responds to short-course antibiotics (nitrofurantoin, trimethoprim-sulfamethoxazole, or fosfomycin), but recurrent UTI is increasingly common as antibiotic resistance grows and as the consequences of repeated antibiotic exposure on the vaginal and gut microbiome become better appreciated.
Berberine has two relevant mechanisms for UTI prevention and adjunctive treatment:
- Anti-adhesion effect on FimH — berberine downregulates the type-I fimbriae and the FimH mannose-binding adhesin that UPEC uses to adhere to the bladder uroepithelium. Without adhesion, the bacteria are washed out with urine before they can colonize. This is mechanistically similar to the proanthocyanidin (PAC) action of cranberry but operates through a different molecular target.
- Direct antibacterial action against UPEC — the spectrum and MIC data above. Urinary berberine concentration after oral dosing is meaningful (the absorbed fraction is largely excreted unchanged in urine), and topical concentration on the uroepithelium can be bactericidal.
Clinical evidence for berberine in UTI is more limited than for diarrheal disease. Several small RCTs have demonstrated benefit in recurrent UTI prevention — typically combining berberine 500 mg twice daily with D-mannose 1-2 g twice daily, with the combination showing better prevention efficacy than either agent alone, and approaching the efficacy of low-dose prophylactic nitrofurantoin without the antibiotic resistance and microbiome concerns. For acute symptomatic UTI, berberine is best considered an adjunct to conventional antibiotics rather than a replacement, particularly given the risk of progression to pyelonephritis if undertreated.
For more on UTI, see our Urinary Tract Infections page.
Skin, Eye, and Mucosal Infection
Topical berberine and barberry root preparations have a long history of use in skin infection, conjunctivitis, oral mucosal ulceration, and otitis externa. The advantage of topical use is that concentration at the site of infection can easily reach the bactericidal/fungicidal range without any concern about poor systemic absorption.
- Bacterial skin infections (impetigo, folliculitis, infected eczema) — topical 0.1-0.5% berberine cream or 1:5 barberry tincture diluted 1:5 with water for compress application. Goldenseal salves (which include hydrastine for the NorA-pump effect against Staph aureus) tend to outperform pure barberry preparations for staphylococcal skin infection.
- Fungal skin infection (athlete's foot, ringworm) — topical 0.1-0.5% berberine has documented efficacy against Trichophyton and Microsporum dermatophytes. Often combined with tea tree oil (1-5%) for synergistic effect.
- Bacterial and viral conjunctivitis — sterile 0.2% berberine eye drops have a long history of use for conjunctivitis in traditional Chinese ophthalmology. Modern data is sparse but the topical safety profile is good. Berberine eye drops are commercially available in China as a non-prescription product.
- Oral mucosal ulceration (aphthous stomatitis, post-radiation mucositis) — berberine mouthwashes (50-200 mg berberine in 10 mL water, swished and spat 3-4×/day) have demonstrated benefit in trials of recurrent aphthous ulcers and chemotherapy/radiation-induced mucositis.
- Otitis externa — dilute berberine ear drops (0.1% in glycerin or in propylene glycol vehicle) have traditional use in chronic otitis externa, particularly when caused by Pseudomonas or Staphylococcus. Modern data is limited.
Effect on the Commensal Gut Microbiome
A common and reasonable concern about long-term berberine use is the effect on the commensal gut microbiome. Berberine is, after all, a broad-spectrum antibacterial with high intraluminal gut concentrations. Would chronic berberine use destroy the commensal microbiome the way long-term broad-spectrum antibiotics do?
The answer, surprisingly, appears to be no — or at least, the picture is much more nuanced than a simple equivalence with antibiotic-induced dysbiosis would predict. Multiple human and animal studies have now examined the gut-microbiome impact of berberine, with consistent findings:
- Reduced abundance of pathobionts — berberine reduces relative abundance of opportunistic pathogens including pathogenic E. coli, Clostridium species (including C. difficile), and several other pro-inflammatory taxa.
- Increased abundance of short-chain-fatty-acid producers — counterintuitively, berberine appears to increase the abundance of beneficial SCFA-producing taxa including Akkermansia muciniphila, Faecalibacterium prausnitzii, Roseburia, and Bifidobacterium. The proposed mechanism is partly direct (some of these taxa appear to be relatively resistant to berberine compared with pathobionts) and partly indirect via the removal of competitive pressure from pathogen overgrowth.
- Increased microbiome diversity — alpha-diversity metrics typically increase, not decrease, on chronic berberine therapy — the opposite of what happens with conventional antibiotics.
- Restored bile-acid metabolism — berberine appears to shift the secondary bile acid profile in a direction associated with improved insulin sensitivity and reduced hepatic steatosis.
The mechanism by which a broad-spectrum antibacterial alkaloid manages to selectively suppress pathobionts while sparing or enhancing beneficial taxa is not entirely understood. One hypothesis is that the SCFA-producing commensals are intrinsically less susceptible to berberine because they rely less on the FtsZ-dependent cell-division machinery (some have alternative septum-formation mechanisms). Another is that berberine's anti-inflammatory effect on the host gut epithelium restores conditions favorable to commensal growth. Whatever the mechanism, the net effect for long-term berberine use is favorable in terms of microbiome composition, and this is a significant advantage over conventional antibiotic prophylaxis.
For more on gut health generally, see our Gut Healing page.
Dosing and Practical Forms (Decoction, Tincture, Capsule)
Barberry root decoction. 1-2 teaspoons (2-4 g) of dried, crushed barberry root bark simmered in 250-300 mL water for 15-20 minutes, strained, and consumed 2-3× daily. The tea has a strong bitter taste that is part of the cholagogue / digestive effect. Approximate berberine delivery: 50-100 mg per cup. This is the classical preparation for digestive bitter and mild antimicrobial use.
Barberry tincture (1:5, 40-50% alcohol). 30-60 drops (2-4 mL) diluted in water, 2-3× daily before meals for digestive use; up to 4×/day for acute antimicrobial use. The alcohol vehicle enhances berberine extraction and improves shelf life. Tinctures are convenient and dose-titratable.
Barberry capsules (standardized). Commercial barberry capsules are typically standardized to 5-10% berberine and dosed at 400-500 mg of dried root extract, 2-3×/day. Approximate berberine delivery: 20-50 mg per capsule. This is far less berberine than the standardized berberine HCl supplements typically deliver (500 mg berberine per capsule).
Standardized berberine HCl supplements (extracted from Coptis or Phellodendron). The form used in the Yin 2008 metformin-comparison trial and most modern cardiometabolic protocols. Typically 500 mg three times daily with meals. Not "barberry" per se but the same active alkaloid.
Topical preparations. 0.1-0.5% berberine in cream, ointment, gel, or compress for skin infection. Eye drops at 0.2%, mouthwash at 50-200 mg per 10 mL water, ear drops at 0.1% in glycerin vehicle.
For acute use (e.g., traveler's diarrhea, acute giardiasis, acute bacterial gastroenteritis), the higher-dose standardized berberine HCl is more practical than the whole-herb barberry preparations because the dose required to achieve clinical effect is impractical to deliver as crude root. For chronic, lower-dose use (digestive bitter, mild antimicrobial maintenance, cholagogue), the whole-herb tincture or decoction is appropriate and provides the additional benefit of the bitter cephalic-phase digestive effect.
Cautions and Drug Interactions
- Pregnancy and breastfeeding (contraindicated) — berberine crosses the placenta and is found in breast milk. It can displace bilirubin from albumin binding, increasing free bilirubin levels and risking kernicterus in newborns. Barberry preparations are also uterine stimulants in some animal models. Pregnant and breastfeeding women should avoid barberry and standardized berberine.
- Infants (contraindicated) — same kernicterus / bilirubin-displacement concern. Berberine should not be administered to infants.
- CYP3A4 inhibition (significant drug interaction) — berberine is a potent inhibitor of cytochrome P450 3A4, the enzyme responsible for metabolism of approximately half of all prescription drugs. Significant interactions are well-documented with cyclosporine (greatly increased cyclosporine levels), tacrolimus, several statins (atorvastatin, simvastatin, lovastatin), some calcium channel blockers, and many others. Patients on multiple prescription medications should consult a pharmacist before starting chronic berberine use.
- Hypoglycemia with diabetes medications — the AMPK / glucose-lowering action of berberine adds to the effect of metformin, sulfonylureas, insulin, and other antidiabetics. Glucose monitoring is essential when berberine is added to an existing diabetes regimen, and downward dose adjustment of conventional medications is often required.
- GI tolerability — the most common adverse effect is constipation (for some patients) or diarrhea (for others) at higher doses. Splitting the dose, taking with food, or stepping down the dose typically resolves the symptom. Some patients report bitter or metallic taste, which is the cephalic-phase bitter effect and not a true adverse reaction.
- Anticoagulants — berberine may potentiate warfarin and other anticoagulants. INR monitoring is required when berberine is added or removed from a regimen.
- Hypotension — berberine has mild vasodilator effects and may augment antihypertensive drugs. Blood pressure monitoring is appropriate in patients on multiple antihypertensives.
Key Research Papers
- Khin-Maung-U et al. (1985). Clinical trial of berberine in acute watery diarrhoea. British Medical Journal. — PubMed
- Rabbani GH et al. (1987). Randomized controlled trial of berberine sulfate therapy for diarrhea due to enterotoxigenic E. coli and Vibrio cholerae. Journal of Infectious Diseases. — PubMed
- Choudry VP et al. (1972). Berberine in giardiasis. Indian Pediatrics. — the classical comparison of berberine, metronidazole, and furazolidone in pediatric giardiasis. PubMed
- Cernakova M, Kostalova D (2002). Antimicrobial activity of berberine — a constituent of Mahonia aquifolium. Folia Microbiologica. — comprehensive MIC tabulation across pathogen classes. PubMed
- Stermitz FR et al. (2000). Synergy in a medicinal plant: antimicrobial action of berberine potentiated by 5'-methoxyhydnocarpin, a multidrug pump inhibitor. PNAS. — the foundational NorA-pump synergy paper that explains the goldenseal-versus-barberry difference. PubMed
- Imanshahidi M, Hosseinzadeh H (2008). Pharmacological and therapeutic effects of Berberis vulgaris and its active constituent, berberine. Phytotherapy Research. — PubMed
- Sun D et al. (1988). Berberine sulfate blocks adherence of Streptococcus pyogenes to epithelial cells, fibronectin, and hexadecane. Antimicrobial Agents and Chemotherapy. — foundational anti-adhesion mechanism paper. PubMed
- Wultanska D et al. (2020). Effect of berberine on Clostridioides difficile growth, toxin production, and adherence to human intestinal cells. Anaerobe. — PubMed
- Sack RB, Froehlich JL (1982). Berberine inhibits intestinal secretory response of Vibrio cholerae and E. coli enterotoxins. Infection and Immunity. — the antitoxin mechanism foundation. PubMed
- Domadia PN et al. (2008). Berberine targets assembly of Escherichia coli cell division protein FtsZ. Biochemistry. — mechanism paper for FtsZ inhibition. PubMed
- Liu CS et al. (2015). Research progress on berberine with a special focus on its oral bioavailability. Fitoterapia. — covers the absorption / efflux pump issues. PubMed
- Cao H et al. (2022). Berberine and the gut microbiome: a systematic review of human studies. Frontiers in Pharmacology. — the modern picture on microbiome effects. PubMed
PubMed Topic Searches
- PubMed: Berberine antimicrobial mechanism
- PubMed: Berberine cholera / ETEC
- PubMed: Berberine and Giardia
- PubMed: Berberine and MRSA
- PubMed: Berberine FtsZ mechanism
- PubMed: Berberine gut microbiome
Connections
- Barberry Overview
- Barberry Benefits Hub
- Barberry for Blood Sugar
- Barberry for Liver Health
- Barberry as a Digestive Aid
- Berberine (Standardized Supplement)
- Berberine Benefits Deep Dive
- Goldenseal (Hydrastine + NorA Synergy)
- Oregano
- Parasites
- Gut Healing
- Escherichia Coli
- Staphylococcus Aureus
- Klebsiella Pneumoniae
- Urinary Tract Infections
- Irritable Bowel Syndrome
- All Herbs