Head and Neck Cancer
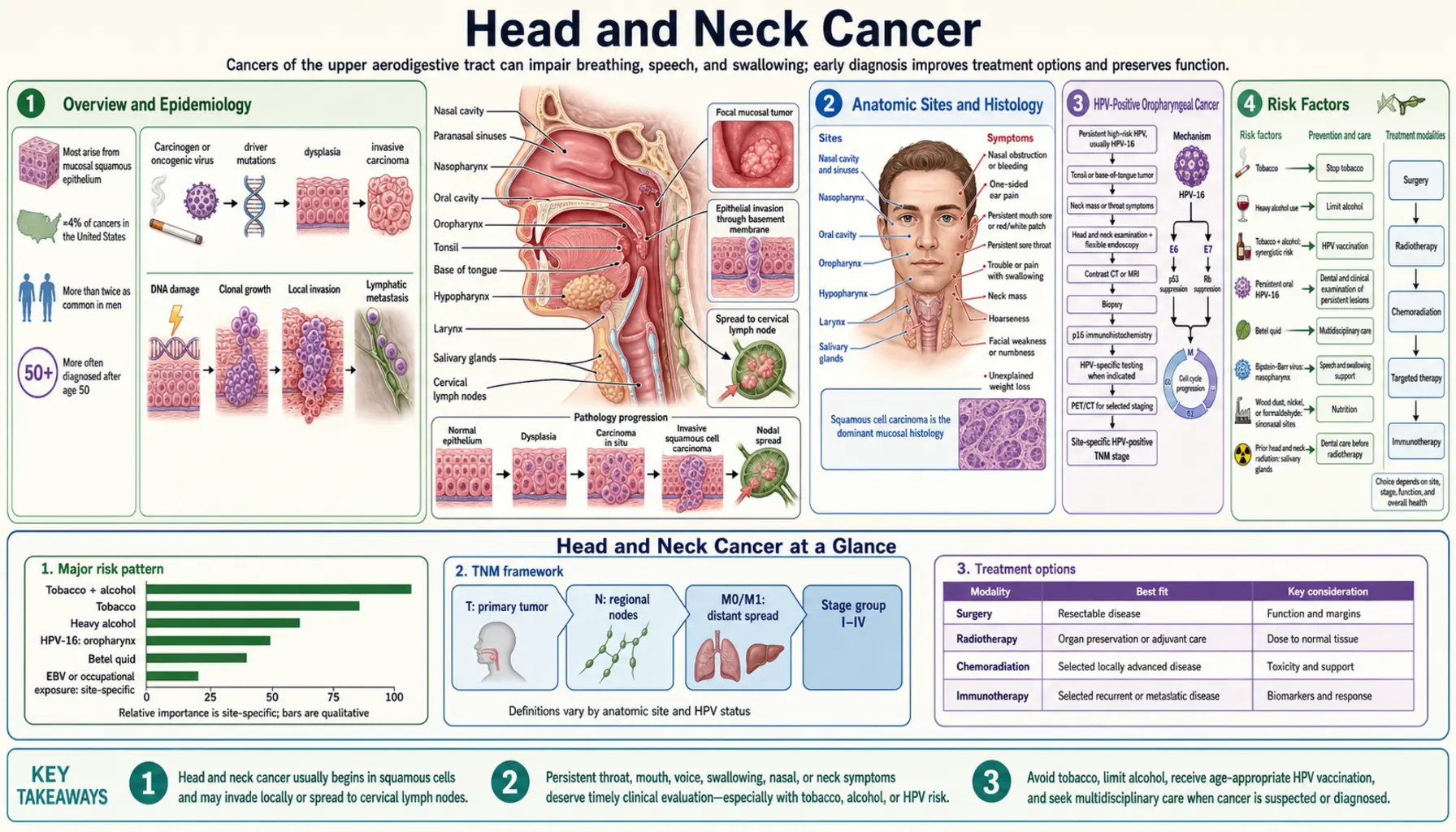
Table of Contents
- Overview and Epidemiology
- Anatomic Sites and Histology
- HPV-Positive Oropharyngeal Cancer
- Risk Factors
- Presentation and Diagnosis
- Staging (AJCC 8th Edition)
- Treatment
- Supportive Care and Quality of Life
- Prevention
- Prognosis
- Key Research Papers
- Connections
- Featured Videos
Overview and Epidemiology
Head and neck cancers (HNCs) are a diverse group of malignancies that arise from the mucosal surfaces lining the oral cavity, pharynx, larynx, and salivary glands. Think of the entire passageway from your lips to your voice box — any cancer arising from the inner lining of those structures falls under this umbrella. In the United States, roughly 68,000 new cases are diagnosed each year and approximately 15,000 people die from head and neck cancer annually (2024 estimates).
Men are affected two to three times more often than women, though that ratio has been shifting. One of the most significant developments in cancer medicine over the past two decades is the HPV revolution in head and neck cancer. Human papillomavirus — particularly HPV type 16, the same virus that causes cervical cancer — now drives roughly 70% of oropharyngeal squamous cell carcinomas in the United States. These tumors are biologically distinct from tobacco-related cancers: they tend to arise in white, middle-aged men, often without a history of heavy smoking or drinking, and they carry a dramatically better prognosis.
The overall picture in HNC epidemiology is mixed. Incidence of oropharyngeal cancer is rising because of HPV, while laryngeal and hypopharyngeal cancers are declining as smoking rates fall. This creates two almost separate diseases within the same anatomic neighborhood — one driven by viral infection and largely curable, the other driven by tobacco and alcohol with stubbornly poor outcomes. Understanding which type a patient has changes almost everything about their treatment plan and expected outcome.
Anatomic Sites and Histology
Head and neck cancer is not one disease — it is an anatomic category covering several distinct tumor locations, each with its own behavior and treatment approach.
Oral Cavity
The oral cavity includes the lips, the mobile (oral) tongue (the front two-thirds), the floor of the mouth, the hard palate, the inner lining of the cheeks (buccal mucosa), and the retromolar trigone (the small triangle of tissue behind the last lower molar). Oral cavity cancers are strongly tied to tobacco and alcohol use. Surgery is the preferred primary treatment for most oral cavity tumors.
Oropharynx
The oropharynx is the middle part of the throat and includes the base of the tongue (the back one-third, which you cannot easily see), the tonsils, the soft palate, and the posterior pharyngeal wall. This is the HPV epicenter. Because the base of tongue and tonsils have large amounts of lymphoid tissue, HPV-related tumors here tend to be found as a small, often invisible primary tumor that has already spread to a lymph node in the neck — which is frequently the patient's first noticeable symptom.
Hypopharynx
The hypopharynx surrounds the larynx (voice box) and connects the throat to the esophagus. It includes the pyriform sinuses (the two pockets on either side of the larynx), the posterior pharyngeal wall, and the postcricoid region. Hypopharyngeal cancers are often caught late because early symptoms are subtle (a vague throat sensation, difficulty swallowing), leading to the worst prognosis among HNC subsites.
Larynx
The larynx (voice box) has three regions: the supraglottis (above the vocal cords), the glottis (the vocal cords themselves), and the subglottis (below the cords). Glottic cancers are often diagnosed early because even a small tumor on a vocal cord causes hoarseness — the laryngeal equivalent of a canary in a coal mine. Supraglottic and subglottic tumors are caught later and behave more aggressively.
Salivary Glands
The parotid gland (the large gland in front of and below the ear) is the most common site for salivary gland tumors, though most parotid tumors are benign (pleomorphic adenoma, Warthin tumor). Malignant salivary tumors are more commonly high-grade when they arise from the minor salivary glands scattered throughout the mouth and throat. Salivary gland cancers span a wide range of histologic types — mucoepidermoid carcinoma, adenoid cystic carcinoma, acinic cell carcinoma, and more — each with different behavior.
Nasopharynx: A Separate Disease
Nasopharyngeal carcinoma (NPC), which arises from the uppermost part of the throat behind the nasal cavity, is biologically distinct from the other head and neck cancers. NPC is driven by Epstein-Barr virus (EBV), not HPV or tobacco, and is treated as a separate entity. It has its own staging system, its own endemic geography (Southeast Asia, North Africa), and different treatment protocols. It is not covered in depth here.
Histology
Approximately 90% of head and neck cancers are squamous cell carcinomas (SCC) — malignancies arising from the flat, scale-like cells that line the mucosal surfaces. The remaining 10% include adenocarcinomas (mostly from salivary glands), lymphomas (particularly in Waldeyer's ring), melanomas, sarcomas, and others. When an oncologist talks about head and neck cancer treatment protocols, they almost always mean squamous cell carcinoma of the head and neck (HNSCC).
HPV-Positive Oropharyngeal Cancer
HPV-positive oropharyngeal squamous cell carcinoma (OPSCC) has transformed the landscape of head and neck oncology. Understanding it separately from tobacco-related HNC is essential because the staging, prognosis, and even the direction of treatment research differ fundamentally.
The Virus and How It Causes Cancer
HPV type 16 is responsible for the vast majority of HPV-driven oropharyngeal cancers — over 90% of HPV-positive OPSCC cases. The virus is transmitted sexually, primarily through oral-genital contact, and can remain dormant in tonsillar crypts for years or decades before triggering malignant transformation. Unlike cervical HPV, there is no standard screening test to detect oropharyngeal HPV infection before it becomes cancer.
The p16 Marker
In clinical practice, HPV status in oropharyngeal tumors is determined by p16 immunohistochemistry (IHC). p16 is a tumor suppressor protein that is overexpressed when HPV's E7 oncoprotein inactivates the retinoblastoma pathway. Strong, diffuse p16 positivity (staining ≥70% of tumor cells) serves as a reliable surrogate for HPV-driven cancer and is used for staging purposes. Direct HPV DNA testing by in situ hybridization (ISH) or PCR is more specific but p16 IHC is the standard clinical test.
Separate Staging: AJCC 8th Edition (2018)
The 2018 AJCC 8th edition introduced a completely separate staging system for HPV-positive OPSCC, recognizing that the old staging dramatically overstaged these patients (an HPV+ patient staged at "Stage IV" under old criteria might have a better prognosis than an HPV− patient at "Stage II"). Key differences:
- T-stage simplified: T1 (≤2 cm) and T2 (2–4 cm) remain, but the threshold for T3/T4 is set differently; T4 requires invasion of critical structures (masticator space, pterygoid plates, skull base, or internal carotid artery encasement).
- N-stage completely different: For HPV+, it is based on number of nodes and whether extranodal extension (ENE) is present, not on size. N1 = up to 4 ipsilateral lymph nodes ≤6 cm, ENE absent. N2 = contralateral or bilateral nodes ≤6 cm, ENE absent. N3 = any node >6 cm OR any ENE. This reflects the fact that bilateral nodal disease in HPV+ OPSCC does not carry the same dire prognosis as it does in HPV-negative disease.
- Most patients are Stage I or II under the new system despite having bilateral neck nodes, because the disease is so exquisitely sensitive to chemoradiation.
Dramatically Better Prognosis
Landmark data from Ang et al. (NEJM 2010, PMID 20530316) established that HPV status is the single most important prognostic factor in oropharyngeal cancer. The 3-year overall survival for HPV-positive patients was 82% versus 57% for HPV-negative patients. More contemporary series show 5-year overall survival approaching 80–90% for HPV+ OPSCC, compared to roughly 45% for HPV-negative oropharyngeal cancer.
The De-Escalation Movement
Because HPV+ OPSCC is so responsive to treatment, researchers are actively asking: can we achieve the same cure rates with less treatment? Standard concurrent chemoradiation carries significant long-term toxicity — swallowing dysfunction, xerostomia (dry mouth), fibrosis. Several major trials are exploring reduced radiation doses, reduced chemotherapy intensity, or surgery (via transoral robotic surgery, TORS) followed by reduced adjuvant therapy:
- ECOG 3311: TORS resection followed by risk-stratified adjuvant therapy (observation vs. reduced-dose RT 50 Gy vs. standard RT 60 Gy ± cisplatin). Results show that low-risk patients can be managed with observation alone after surgery.
- PATHOS (UK): TORS followed by chemotherapy reduction based on pathologic risk features.
- NRG HN005: Standard chemoRT vs. reduced-dose RT (60 Gy vs. 50 Gy) for low-risk HPV+ OPSCC.
De-escalation is not yet the standard of care outside of a clinical trial. The standard remains concurrent cisplatin-based chemoradiation or TORS in appropriate surgical candidates, followed by risk-stratified adjuvant therapy.
Typical Presentation
Many patients with HPV+ OPSCC present with a painless neck mass as the first symptom. The primary tumor in the tonsil or base of tongue is often small and not visible on routine examination. This can lead to an initial misdiagnosis of "reactive lymphadenopathy" or even a squamous cell carcinoma diagnosis in the neck node before the primary is found. Fine-needle aspiration (FNA) of the neck node should always include p16 testing, because a positive result should prompt careful oropharyngeal examination and directed biopsies even when the primary is not visible.
Risk Factors
Head and neck cancer risk factors vary by anatomic subsite, but the following are the major drivers:
Tobacco
Tobacco use — both smoking (cigarettes, cigars, pipes) and smokeless tobacco (chewing tobacco, snuff) — remains the single most important risk factor for tobacco-related HNC. There is a clear dose-response relationship: the more pack-years of smoking, the higher the risk. Tobacco use dramatically increases the risk of oral cavity, laryngeal, hypopharyngeal, and HPV-negative oropharyngeal cancers. Importantly, smokeless tobacco is specifically linked to oral cavity cancer (buccal mucosa, gingiva) even though it avoids the larynx.
Alcohol
Heavy alcohol consumption acts as both an independent carcinogen and a synergistic co-carcinogen with tobacco. The combination of heavy smoking and heavy drinking multiplies (not merely adds) head and neck cancer risk. Alcohol is metabolized to acetaldehyde, a known carcinogen, by both human cells and oral bacteria. People with genetic variants in the ALDH2 gene (common in East Asian populations) accumulate more acetaldehyde and have amplified risk.
HPV-16 Sexual Exposure
Sexual transmission of HPV-16 through oral-genital contact is the primary driver of oropharyngeal cancer's rising incidence. Having a higher lifetime number of oral sexual partners increases risk. HPV vaccination (Gardasil 9) is the most powerful preventive tool available for this subtype.
Epstein-Barr Virus (EBV)
EBV is specifically linked to nasopharyngeal carcinoma and some salivary gland tumors. It is not a significant risk factor for the other HNC subsites discussed here.
Betel Quid and Areca Nut
Betel quid chewing — a practice widespread in South and Southeast Asia — is a major risk factor for oral cavity cancer in those regions. Areca nut (the seed inside the betel fruit) is independently carcinogenic even without added tobacco. It causes oral submucous fibrosis, a premalignant condition with high rates of malignant transformation.
Radiation Exposure
Prior therapeutic radiation to the head and neck region increases the risk of salivary gland malignancies, including mucoepidermoid carcinoma. This is seen in adults who received radiation therapy for childhood cancers and in survivors of nuclear fallout exposure.
Plummer-Vinson Syndrome
This rare syndrome — characterized by iron-deficiency anemia, esophageal webs, and atrophic oral mucosa — specifically increases the risk of postcricoid carcinoma (a type of hypopharyngeal cancer) and upper esophageal cancer. It predominantly affects middle-aged women.
Immunosuppression
Immunocompromised patients — including solid organ transplant recipients and people with HIV — have substantially higher rates of HPV-related oropharyngeal cancer and lip cancer. Impaired immune surveillance allows HPV infection to persist and progress.
Occupational Exposures
Chronic exposure to wood dust, leather dust, nickel compounds, and formaldehyde has been linked to nasal cavity and paranasal sinus cancers (sinonasal cancers), which border the HNC spectrum.
Presentation and Diagnosis
The symptoms of head and neck cancer depend on the anatomic site. Knowing what to look for — and when to seek evaluation — can make the difference between a Stage I and a Stage IV diagnosis.
Warning Signs by Site
- Oral cavity: A sore or ulcer that does not heal within 2–3 weeks is the classic warning sign. Other red flags include a white patch (leukoplakia), a red patch (erythroplakia — which carries a malignant potential of up to 50%), a painless lump or thickening in the cheek, lip, or tongue, difficulty chewing or moving the tongue, and loosening of teeth without dental cause.
- Oropharynx: Persistent sore throat not explained by infection, pain or difficulty swallowing (dysphagia), referred ear pain (otalgia) — because the vagus nerve serves both the throat and the ear, oropharyngeal tumors can cause pain perceived in the ear — and most commonly, a painless neck mass.
- Larynx: Hoarseness lasting more than 3 weeks is the signature symptom of glottic (vocal cord) cancer and should prompt ENT evaluation. Stridor (a high-pitched breathing noise) and difficulty breathing suggest advanced disease with airway compromise.
- Hypopharynx: A persistent globus sensation (feeling something is stuck in the throat), dysphagia, voice changes, and unexplained weight loss. Because these symptoms are vague and overlap with reflux and anxiety, hypopharyngeal cancers are often caught late.
Diagnostic Workup
Panendoscopy — also called triple endoscopy — is a cornerstone of HNC workup. Performed under general anesthesia, it involves direct laryngoscopy (examination of the larynx), esophagoscopy (examination of the esophagus), and bronchoscopy (examination of the airways). This allows the surgeon to inspect the entire upper aerodigestive tract for the primary tumor, assess tumor extent, look for synchronous second primary tumors (which occur in roughly 5% of HNC patients due to "field cancerization" from tobacco exposure), and obtain tissue biopsies.
For a neck mass, the preferred first diagnostic step is fine-needle aspiration (FNA) cytology. If FNA is non-diagnostic, a core needle biopsy under ultrasound guidance is next. Open excisional biopsy of a neck node should be avoided if possible, as it can disrupt lymphatic planes and complicate subsequent neck dissection.
Imaging
- CT neck and chest with contrast: The workhorse imaging study. Maps the primary tumor, identifies lymph node involvement (size, number, ENE), and screens for lung metastases or a synchronous lung primary.
- PET-CT: Essential for patients with lymph node involvement (N+) or when distant metastases are suspected. PET-CT also identifies occult primary tumors in patients who present with neck nodal metastasis from an unknown primary.
- MRI: Superior to CT for soft tissue detail and skull base involvement. Used when perineural spread (PNI) along cranial nerves is suspected, or when evaluating tumor extension into the masticator space or pterygopalatine fossa.
- Ultrasound: Used to guide FNA of neck nodes.
HPV Testing
p16 IHC testing should be performed on all oropharyngeal biopsy specimens. The result drives staging (HPV+ vs. HPV-negative staging systems) and will increasingly determine treatment de-escalation eligibility as those trials mature. For non-oropharyngeal SCC, p16 testing is not routinely required for staging but may have prognostic value.
Dental Evaluation
Before starting radiation therapy, patients should have a comprehensive dental evaluation and any compromised teeth should be extracted at least 2 weeks before RT begins. This is essential to prevent osteoradionecrosis of the jaw (ORN), a severe complication in which irradiated bone dies after dental trauma — a condition that is far harder to treat than to prevent.
Staging (AJCC 8th Edition)
Head and neck cancer staging uses the standard TNM system (Tumor size/extension, Nodal involvement, Metastasis), but with one critical twist introduced in the AJCC 8th edition (2018): oropharyngeal cancer is staged differently depending on HPV (p16) status.
Oropharyngeal Cancer — HPV-Positive (p16+)
The HPV-positive staging system was designed to correct the problem that under the 7th edition, many curable HPV+ patients were being categorized as "Stage IV" alongside genuinely advanced disease. Key features:
- T1: Tumor ≤2 cm. T2: Tumor 2–4 cm. T3: Tumor >4 cm or extension to lingual surface of epiglottis. T4: Moderately advanced or very advanced local disease (masticator space, pterygoid plates, lateral nasopharynx, skull base, or internal carotid encasement).
- N1 (clinical): Up to 4 ipsilateral lymph nodes, none >6 cm, ENE absent. N2: Contralateral or bilateral nodes ≤6 cm, ENE absent. N3: Any node >6 cm or ENE present.
- Most HPV+ OPSCC patients stage as Stage I or II under the new system — even those with bilateral neck nodes.
Oropharyngeal Cancer — HPV-Negative AND All Other HNC Sites
For HPV-negative oropharyngeal SCC and for oral cavity, laryngeal, hypopharyngeal, and salivary gland cancers, the traditional staging applies:
- T1–T4 based on tumor size (2 cm and 4 cm are key cutoffs) and critical structure invasion.
- N1: Single ipsilateral node ≤3 cm, ENE absent. N2a: Single ipsilateral node 3–6 cm or ENE+. N2b: Multiple ipsilateral nodes, none >6 cm, ENE absent. N2c: Bilateral or contralateral nodes ≤6 cm, ENE absent. N3a: Any node >6 cm. N3b: Any node, ENE present.
- Extranodal extension (ENE) is an independent adverse prognostic feature that upstages the patient to pN3b and is a mandatory indication for adjuvant chemoradiation in surgically treated patients.
Distant Metastases
M1 (Stage IVC) disease is uncommon at initial diagnosis of HNC (occurring in roughly 5–10% of patients at presentation), but is more common in hypopharyngeal cancer and at recurrence. The lungs are the most frequent site of distant metastasis.
Why Staging Matters for Treatment Planning
Stage largely determines whether a patient is a candidate for single-modality treatment (surgery or radiation alone, for early-stage disease) or requires combined modality therapy (chemoradiation, or surgery plus adjuvant RT/chemoRT). The presence of ENE on pathologic staging triggers mandatory adjuvant cisplatin-based chemoradiation regardless of other features.
Treatment
Treatment of head and neck cancer is highly site-specific and stage-specific. The major treatment modalities are surgery, radiation therapy (RT), chemotherapy, and — increasingly — immunotherapy. Most patients with locally advanced disease receive some combination of these.
Oral Cavity Cancer
Surgery is the preferred primary treatment for oral cavity cancer at all stages where complete resection is feasible. Key principles:
- Wide local excision with ≥1 cm margins for small primaries (T1–T2). For tumors involving or approaching the mandible, marginal mandibulectomy (removing the outer rim of bone) or segmental mandibulectomy (removing a full segment of bone) may be required.
- Reconstruction: Large oral cavity defects require microvascular free flap reconstruction — the most commonly used flaps are the radial forearm free flap (thin, pliable, ideal for tongue and floor of mouth), the fibula free flap (bone-bearing, used when the mandible is resected), and the anterolateral thigh (ALT) free flap (large soft tissue defects).
- Selective neck dissection of levels I–IV is performed even for clinically N0 patients with T2 or greater tumors (occult nodal metastasis rate exceeds 20%), typically simultaneously with the primary resection.
- Adjuvant radiation is given for adverse pathologic features: close or positive margins, perineural invasion (PNI), lymphovascular invasion (LVI), multiple positive nodes, or ENE. Concurrent cisplatin is added to RT when ENE or positive margins are present (the EORTC 22931 and RTOG 9501 trials established this standard).
Larynx and Hypopharynx: Organ Preservation
The landmark RTOG 91-11 trial (Forastiere et al., NEJM 2003, PMID 12594300) established that for locally advanced laryngeal cancer, concurrent cisplatin + radiation achieves better larynx preservation rates than sequential chemotherapy followed by RT or RT alone. This made non-surgical organ preservation the standard for most locally advanced laryngeal cancers:
- Concurrent chemoRT (cisplatin 100 mg/m² every 3 weeks + RT to 70 Gy) for Stage III and most Stage IV laryngeal cancers — preserves the larynx in approximately 80% of patients at 2 years.
- Total laryngectomy (surgical removal of the entire larynx) is reserved for T4a tumors invading through thyroid cartilage, patients with poor pulmonary reserve who cannot tolerate aspiration, or patients who fail chemoRT. Post-laryngectomy, patients breathe through a permanent neck stoma and require voice rehabilitation.
- Hypopharyngeal cancer follows similar principles but is generally considered a more aggressive disease; organ preservation is attempted but surgery is more commonly required.
Oropharyngeal Cancer: Chemoradiation or Surgery
For most patients with oropharyngeal SCC — HPV+ or HPV-negative — the standard definitive treatment is concurrent chemoradiation:
- Cisplatin 100 mg/m² every 3 weeks (3 cycles during RT) or weekly cisplatin 40 mg/m² are both accepted chemotherapy schedules. For patients who cannot tolerate cisplatin (renal insufficiency, neuropathy, hearing loss), weekly carboplatin or cetuximab are alternatives.
- Cetuximab + RT: The BONNER trial (Bonner JA et al., NEJM 2006, PMID 16467544) showed that adding cetuximab (an EGFR inhibitor) to RT improved locoregional control and survival compared to RT alone. However, subsequent trials have not shown cetuximab to be equivalent to cisplatin-based chemoRT, so cisplatin remains preferred when tolerated.
- Transoral robotic surgery (TORS) or transoral laser microsurgery (TLM) allows minimally invasive resection of oropharyngeal tumors through the mouth, avoiding external incisions. In appropriately selected patients (T1–T2, accessible tumors), TORS followed by risk-stratified adjuvant therapy (reduced-dose RT for low-risk pathology) is being evaluated in de-escalation trials as a strategy to reduce long-term treatment toxicity in HPV+ patients.
Salivary Gland Cancers
Salivary gland malignancies are treated primarily with surgery — parotidectomy (superficial or total, with facial nerve preservation when possible), submandibular gland excision, or excision of minor salivary gland tumors. Adjuvant radiation is indicated for high-grade histology, positive or close margins, lymph node involvement, PNI, or advanced stage. Specific histologic subtypes may benefit from targeted therapies:
- HER2-amplified salivary duct carcinoma: Trastuzumab-based regimens (analogous to HER2+ breast cancer) have shown activity.
- Androgen receptor (AR)-positive salivary duct carcinoma: Enzalutamide or other anti-androgen therapies.
- Adenoid cystic carcinoma: Notoriously resistant to chemotherapy; multikinase inhibitors and NOTCH pathway inhibitors are under investigation.
Recurrent and Metastatic HNSCC
For patients with recurrent or metastatic (R/M) HNSCC — disease that cannot be cured with local therapy — systemic treatment is the mainstay:
- EXTREME regimen (Vermorken JB et al., NEJM 2008, PMID 18784101): Cetuximab + cisplatin or carboplatin + 5-fluorouracil (5-FU). This was the previous standard first-line regimen for R/M HNSCC, achieving a median overall survival of 10.1 months versus 7.4 months for platinum/5-FU alone.
- Pembrolizumab (KEYNOTE-048, Burtness B et al., NEJM 2019, PMID 31855730): A game-changing trial that established pembrolizumab (a PD-1 immune checkpoint inhibitor) as the new first-line standard. Key findings:
- For patients with PD-L1 combined positive score (CPS) ≥20: pembrolizumab monotherapy was superior to the EXTREME regimen (median OS 14.9 vs 10.7 months).
- For patients with CPS ≥1: pembrolizumab + platinum/5-FU was superior to EXTREME (median OS 13.6 vs 10.4 months).
- For CPS <1 (a minority of patients): the combination was non-inferior; monotherapy was not tested in this group.
- Pembrolizumab ± chemotherapy has replaced EXTREME as the first-line standard across most guidelines.
- Nivolumab (CheckMate 141, Ferris RL et al., NEJM 2016, PMID 27718784): Nivolumab (another PD-1 inhibitor) was the first immunotherapy to demonstrate survival benefit in platinum-refractory R/M HNSCC. It remains a second-line option after progression on platinum-based therapy and first-line immunotherapy.
Supportive Care and Quality of Life
Head and neck cancer treatment — particularly combined chemoradiation — can profoundly affect quality of life. Many of the structures treated are essential for speaking, swallowing, breathing, and basic comfort. Managing these side effects is as important as treating the tumor itself.
Xerostomia (Dry Mouth)
Radiation-induced damage to the salivary glands is one of the most common and disabling long-term side effects of head and neck RT. Intensity-modulated radiation therapy (IMRT) with parotid gland sparing — directing radiation beams around the parotid glands while still treating the tumor adequately — has substantially reduced xerostomia rates (Fu et al., Int J Radiat Oncol Biol Phys). Management includes pilocarpine (a muscarinic agonist that stimulates remaining salivary tissue), artificial saliva products, frequent sips of water, and meticulous dental hygiene (loss of saliva's protective buffering dramatically increases dental decay).
Dysphagia and Swallowing Rehabilitation
Swallowing dysfunction is extremely common after treatment of oropharyngeal and laryngeal cancers. Radiation fibrosis of the pharyngeal constrictors and base of tongue muscles can cause long-term dysphagia severe enough to require a feeding tube. Key approaches:
- Preventive swallowing exercises during RT ("prophylactic swallowing therapy") — patients perform a structured set of swallowing exercises throughout the radiation course even before dysphagia develops. Evidence suggests this preserves swallowing function better than reactive therapy begun after problems emerge.
- Gastrostomy (PEG) tube: Used when patients cannot maintain adequate oral nutrition. The decision to place a prophylactic (pre-treatment) versus reactive (when needed) PEG is individualized — prophylactic PEG may reduce malnutrition during treatment but some evidence suggests it may reduce the drive to swallow and worsen long-term dysphagia. Most centers use a reactive approach.
- Late stricture or fibrosis of the pharynx can occur months to years post-treatment and may require esophageal dilation.
Mucositis
Radiation-induced oral mucositis — painful inflammation and ulceration of the mucous membranes — is nearly universal during chemoradiation for HNC. It typically peaks at weeks 4–6 of RT and can severely limit oral intake. Management includes aggressive pain control (opioids when needed), "magic mouthwash" (mixtures of lidocaine, diphenhydramine, and antacid), bland diet, excellent oral hygiene, and in some cases palifermin (a keratinocyte growth factor) for patients receiving high-dose chemoRT.
Hypothyroidism
Radiation to the neck that includes the thyroid gland causes hypothyroidism in 20–30% of patients within the first 2 years after treatment, and the incidence continues to rise over time. Annual thyroid function testing (TSH) is standard follow-up practice for all patients who received neck irradiation. Hypothyroidism is easily managed with levothyroxine replacement, but missed cases can cause fatigue, weight gain, and cognitive changes that are wrongly attributed to other causes.
Trismus (Jaw Stiffness)
Radiation fibrosis of the masticatory muscles and temporomandibular joint can cause progressive difficulty opening the mouth (trismus). This makes dental hygiene difficult, limits nutritional intake, and can complicate future dental procedures. Jaw-stretching devices (TheraBite, Dynasplint) used preventively during and after RT can slow or prevent trismus progression.
Lymphedema
Disruption of lymphatic drainage — by surgery, radiation, or both — can cause persistent swelling of the face, neck, and submental region. Head and neck lymphedema (including internal pharyngeal swelling that worsens dysphagia) responds to specialized lymphedema therapy and compression garments.
Voice Rehabilitation After Laryngectomy
Patients who require total laryngectomy lose their natural voice. Three main options for voice rehabilitation exist:
- Tracheoesophageal puncture (TEP) with voice prosthesis: A small one-way valve placed surgically between the trachea and esophagus allows patients to redirect air from the lungs through the esophagus to produce voice. This is the most widely used and typically highest-quality voice rehabilitation method.
- Electrolarynx: A handheld vibrating device held against the neck or cheek that produces a monotone sound, shaped into words by normal articulation. Immediately available, but the robotic-sounding voice can be difficult to understand.
- Esophageal speech: The patient learns to swallow air and expel it in controlled bursts to vibrate the esophagus. No external device required, but requires significant practice and is not achievable by all patients.
Return to Oral Nutrition
After treatment, a multidisciplinary team including speech-language pathologists, dietitians, and oncology nurses guides patients back toward oral nutrition. Modified textures, dietary modifications, and swallowing technique training are standard components of recovery. Some patients will require long-term tube feeding.
Prevention
A significant proportion of head and neck cancers are preventable — both by reducing exposure to known carcinogens and by vaccination against the viral drivers of oropharyngeal cancer.
HPV Vaccination
Gardasil 9 (the current 9-valent HPV vaccine) provides strong protection against HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58. Type 16 — responsible for most HPV-driven oropharyngeal cancer — is covered. The vaccine is recommended for all adolescents (ideally at ages 11–12) and for adults up to age 45 who have not completed the series. Vaccination is most effective before exposure to HPV, but can still provide partial benefit in sexually active adults.
Because oropharyngeal HPV cancer takes decades to develop, the measurable impact of vaccination on HNC incidence rates is not yet visible in population data — but mathematical models and cervical cancer incidence data strongly support the expectation that widespread vaccination will substantially reduce HPV-driven oropharyngeal cancer rates in coming decades.
Tobacco Cessation
Smoking cessation is the single most powerful intervention for reducing HNC risk in current smokers. The excess risk from smoking begins to decline within 5 years of quitting and continues to fall over decades, though it never fully returns to the risk level of a lifelong non-smoker. Resources include FDA-approved pharmacotherapy (varenicline/Chantix, bupropion, nicotine replacement therapy), behavioral counseling, and quitlines (1-800-QUIT-NOW in the US). For smokeless tobacco users, cessation programs targeting chewing tobacco and snuff reduce oral cavity cancer risk.
Alcohol Moderation
Limiting alcohol consumption — particularly in combination with tobacco — substantially reduces head and neck cancer risk. The relative risk reduction from reducing alcohol intake is greatest in heavy drinkers.
Dental Care Before Radiation
Pre-radiation dental extraction of compromised teeth (cracked, severely decayed, or periodontally involved teeth) at least 2 weeks before RT begins is essential to prevent osteoradionecrosis of the jaw (ORN). Once irradiated, jaw bone has diminished ability to heal after dental trauma. Prophylactic fluoride trays help protect teeth from radiation-induced decay.
Oral Cancer Screening
Visual inspection of the oral cavity and palpation of the neck for lymphadenopathy during routine dental and medical visits can detect premalignant lesions and early cancers. Erythroplakia (red, velvety patches) and erythroleukoplakia (mixed red and white patches) carry the highest malignant potential and warrant biopsy. Toluidine blue dye rinse can help highlight suspicious lesions. Any lesion that does not resolve within 2–3 weeks should be biopsied.
Prognosis
Prognosis in head and neck cancer varies enormously depending on primary site, stage, HPV status, and histologic type. The most important determinant of outcome is stage at diagnosis — early-stage cancers are highly curable across all sites, while late-stage cancers carry poor prognoses at most subsites.
Approximate 5-Year Overall Survival by Site
- Oral cavity: 55–65% overall; Stage I approaching 85%, Stage IV as low as 30%.
- Oropharynx, HPV-positive: ~80% with contemporary chemoradiation; Stage I (new AJCC 8th ed.) approaching 90%.
- Oropharynx, HPV-negative: ~45%; outcomes similar to other tobacco-related HNC sites.
- Larynx, glottic: ~60%; early-stage (T1 glottic) approaching 90% with RT alone. The early-symptom (hoarseness) advantage of glottic cancer translates into earlier diagnosis on average.
- Hypopharynx: ~30% — the worst HNC prognosis, largely because most patients present with Stage III or IV disease and because the tumor biology is aggressive.
- Salivary gland (highly variable by histotype):
- Acinic cell carcinoma: ~90% at 5 years (low-grade, excellent prognosis)
- Low-grade mucoepidermoid: ~90%
- High-grade mucoepidermoid: ~50%
- Adenoid cystic carcinoma: 50–60% at 10 years — an important caveat is that adenoid cystic carcinoma follows an indolent but relentless course, with late recurrences common; 5-year survival looks better than 10- or 20-year survival.
- Salivary duct carcinoma / high-grade adenocarcinoma: <30%
Key Prognostic Factors
Beyond stage, the factors most strongly associated with prognosis include: HPV/p16 status (positive = substantially better for oropharynx), extranodal extension (ENE — its presence on pathology dramatically worsens prognosis), surgical margin status (positive margins increase recurrence risk), performance status (ability to tolerate full-dose concurrent chemotherapy), and continued tobacco use during and after treatment (smokers who continue during chemoRT have significantly worse outcomes — cessation is a therapeutic intervention, not just a lifestyle preference).
Recurrence Patterns
Most recurrences occur within the first 2–3 years after treatment. Locoregional recurrence (recurrence at the original site or regional nodes) can sometimes be treated with salvage surgery if the patient was initially treated with radiation, or with re-irradiation (reirradiation) in highly selected cases. Distant metastases (most commonly lung) are usually treated with systemic therapy (pembrolizumab, platinum-based chemotherapy) with palliative intent.
Key Research Papers
- Ang KK, Harris J, Wheeler R, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med. 2010;363(1):24–35. PMID 20530316 — Landmark study establishing HPV as the dominant prognostic factor in oropharyngeal cancer; defined low-, intermediate-, and high-risk groups.
- Forastiere AA, Zhang Q, Weber RS, et al. Long-term results of RTOG 91-11: a comparison of three nonsurgical treatment strategies to preserve the larynx in patients with locally advanced larynx cancer. J Clin Oncol. 2013;31(7):845–852. (Original NEJM publication 2003.) — Search PubMed — Established concurrent cisplatin + radiation as superior to sequential chemotherapy or RT alone for larynx preservation.
- Burtness B, Harrington KJ, Greil R, et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): a randomised, open-label, phase 3 study. Lancet. 2019;394(10212):1915–1928. — Search PubMed — Established pembrolizumab as new first-line standard for recurrent/metastatic HNSCC based on PD-L1 CPS score.
- Ferris RL, Blumenschein G Jr, Fayette J, et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N Engl J Med. 2016;375(19):1856–1867. — Search PubMed — CheckMate 141: first immunotherapy to show OS benefit in platinum-refractory R/M HNSCC.
- Vermorken JB, Mesia R, Rivera F, et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N Engl J Med. 2008;359(11):1116–1127. PMID 18784101 — EXTREME trial: established cetuximab + platinum/5-FU as previous first-line standard for R/M HNSCC.
- Bonner JA, Harari PM, Giralt J, et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N Engl J Med. 2006;354(6):567–578. PMID 16467544 — Demonstrated improved locoregional control and OS with cetuximab added to RT vs RT alone in locally advanced HNSCC.
- Mehanna H, Beech T, Nicholson T, et al. Prevalence of human papillomavirus in oropharyngeal and nonoropharyngeal head and neck cancer — systematic review and meta-analysis of trends by time and region. Head Neck. 2013;35(5):747–755. PMID 22267298 — Comprehensive meta-analysis of HPV prevalence and temporal trends in oropharyngeal cancer.
- Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74(1):12–49. — Search PubMed — Current US incidence and mortality data for all cancers including head and neck.
- O'Sullivan B, Huang SH, Su J, et al. Development and validation of a staging system for HPV-related oropharyngeal cancer by the International Collaboration on Oropharyngeal cancer Network for Staging (ICON-S). Lancet Oncol. 2016;17(4):440–451. PMID 26936027 — Foundation work for the separate AJCC 8th edition HPV+ oropharyngeal staging system.
- Fu KK, Pajak TF, Trotti A, et al. A Radiation Therapy Oncology Group (RTOG) phase III randomized study to compare hyperfractionation and two variants of accelerated fractionation to standard fractionation radiotherapy for head and neck squamous cell carcinomas: first report of RTOG 9003. Int J Radiat Oncol Biol Phys. 2000;48(1):7–16. PMID 10924966 — RTOG 9003; key fractionation data for HNC; basis for accelerated RT schedules and parotid-sparing IMRT research.
- Cognetti DM, Weber RS, Lai SY. Head and neck cancer: an evolving treatment paradigm. Cancer. 2008;113(7 Suppl):1911–1932. — Search PubMed — Comprehensive review of evolving HNC treatment paradigms including organ preservation and molecular targeted therapy.
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology: Head and Neck Cancers. Version 2.2024. NCCN Guidelines — Head and Neck Cancers — The definitive US clinical guideline covering all subsites, staging, treatment algorithms, and supportive care (free registration required).
PubMed Topic Searches
- Head and neck squamous cell carcinoma treatment — PubMed
- HPV oropharyngeal cancer prognosis — PubMed
- Larynx preservation chemoradiation — PubMed
- Pembrolizumab head neck cancer immunotherapy — PubMed
- IMRT xerostomia salivary gland sparing — PubMed
Connections
- Oncology
- All Conditions
- Cancer Overview
- Oral Cancer
- Thyroid Cancer
- Lung Cancer
- Lymphoma
- Skin Cancer
- Cervical Cancer
- Esophageal Cancer
- Turmeric
- Vitamin D3
- Vitamin C
- Selenium and Cancer Prevention
- Zinc
- Glutamine