Breast Cancer
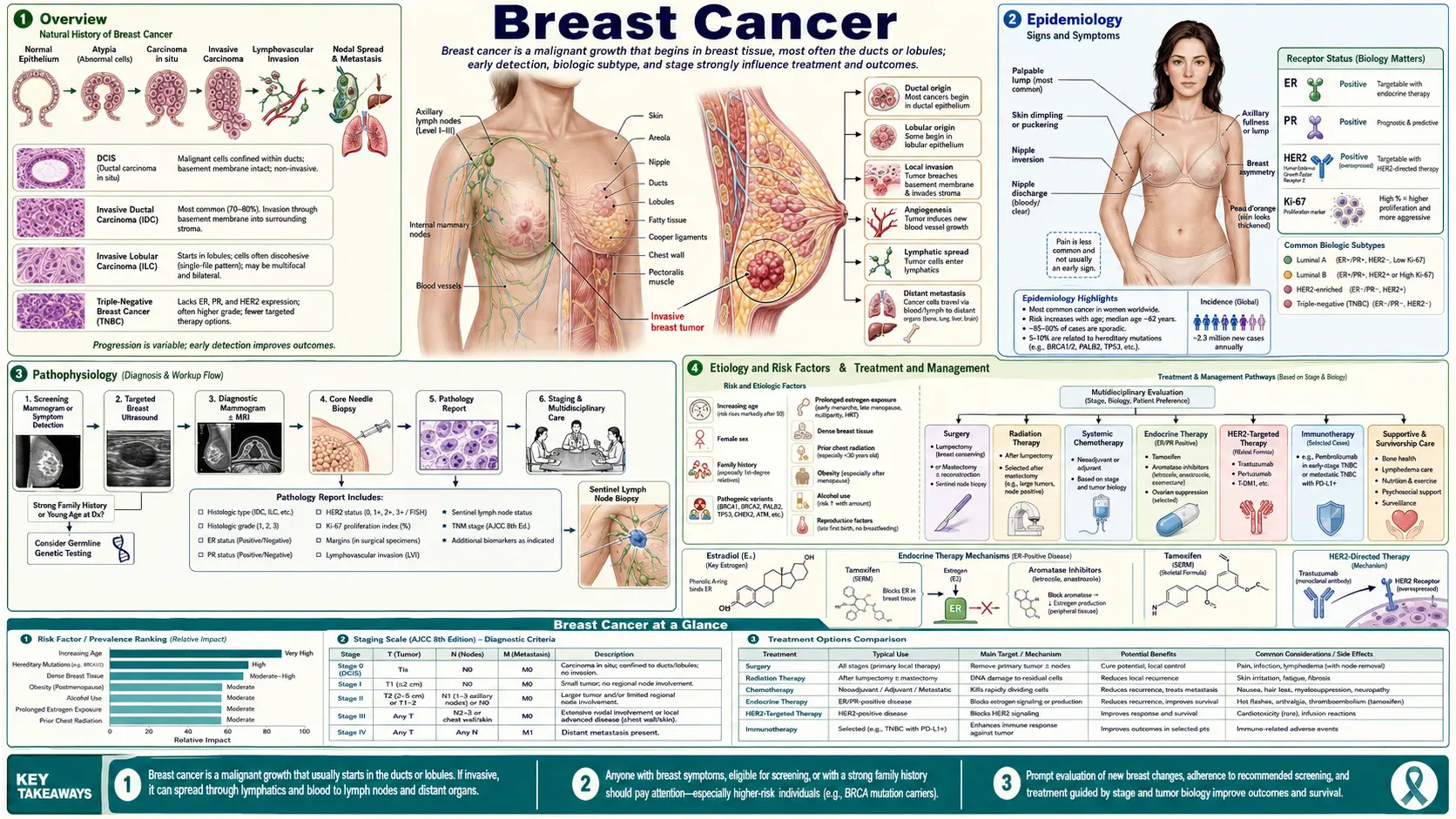
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research and Advances
- Research Papers
- Connections
- Featured Videos
1. Overview
Breast cancer is a malignancy that begins when cells in the breast — most often the cells lining the milk ducts or the milk-producing lobules — start growing and dividing out of control. It is the most common cancer diagnosed in women in the United States (apart from skin cancer), with roughly 310,000 new invasive cases and about 56,000 cases of ductal carcinoma in situ (DCIS) diagnosed each year. About 1 in 8 American women will develop invasive breast cancer at some point in her lifetime. Men get breast cancer too — roughly 2,800 cases a year in the US — though it accounts for under 1% of all breast cancers.
Here is the single most important thing to understand if you or someone you love has just been diagnosed: breast cancer is not one disease. It is a family of diseases that look different under the microscope and, more importantly, are driven by different biology. Two women can have tumors of the exact same size and stage and still need completely different treatments — and have very different outlooks — because their tumors belong to different molecular subtypes. The three receptors that define those subtypes are the estrogen receptor (ER), the progesterone receptor (PR), and a growth-signaling protein called HER2. Whether each one is present or absent is what your pathology report is really telling you, and it is what drives every treatment decision that follows.
The other thing worth holding onto is that breast cancer is, for most people, a highly treatable disease. When it is caught while still confined to the breast, the five-year relative survival is about 99%. Even when it has spread to nearby lymph nodes, five-year survival is around 86%. The numbers are far more sobering when the disease has spread to distant organs — but the great majority of breast cancers are not found at that stage. This page walks through who gets breast cancer, why, how it is found, how each subtype is treated, what survivorship looks like, and what is genuinely known about lowering risk.
2. Epidemiology
Breast cancer is the most frequently diagnosed cancer in women worldwide and, after lung cancer, the leading cause of cancer death in women in the US. The lifetime risk for an average-risk woman is about 13% (the "1 in 8" figure). That risk is not spread evenly across life — it climbs steadily with age. The median age at diagnosis is about 62, and roughly four out of five invasive cases are diagnosed in women aged 50 or older.
There is an important and often-overlooked disparity. Black women in the US are diagnosed with breast cancer at a slightly lower rate than White women but are about 40% more likely to die of it. Several forces drive this gap: Black women are more likely to be diagnosed with aggressive triple-negative tumors, more likely to be diagnosed at a later stage, and more likely to face delays in starting and completing treatment. These are not biological inevitabilities — much of the gap reflects access, and that means it is at least partly fixable.
The good news at the population level: US breast cancer death rates have fallen by roughly 40% since 1989. That decline is credited to a combination of earlier detection through mammography and dramatically better treatment — particularly endocrine therapy and HER2-targeted drugs. Incidence has crept upward slightly in recent years, especially in women under 50, a trend researchers are still working to fully explain.
3. Pathophysiology
Normal breast tissue is organized into lobules (the glands that make milk) connected by ducts (the tubes that carry milk to the nipple). Most breast cancers begin in the cells lining these structures. When those cells accumulate enough genetic damage to escape the normal controls on growth, they begin to multiply and pile up.
A crucial distinction is between in situ and invasive disease. In ductal carcinoma in situ (DCIS), abnormal cells are confined inside the duct and have not broken through its wall. DCIS is sometimes called "stage 0" cancer. It cannot spread or threaten life while it stays in situ — but a meaningful fraction, if untreated, will progress to invasive cancer over years, and we cannot yet reliably tell which ones will. Invasive (or infiltrating) cancer has broken through the duct or lobule wall into surrounding breast tissue, where it can reach lymphatic and blood vessels and travel elsewhere. Invasive ductal carcinoma (now often called invasive carcinoma of no special type) accounts for about 70–80% of invasive cases; invasive lobular carcinoma, which tends to grow in a more diffuse, hard-to-image pattern, makes up about 10–15%.
The molecular subtypes — the heart of modern breast cancer care. Breast cancers are sorted into groups based on three markers measured on the biopsy:
- Hormone-receptor positive, HER2-negative (HR+/HER2−) — by far the most common, about 65–70% of cases. These tumors carry estrogen and/or progesterone receptors, meaning they are fueled by estrogen. They tend to grow more slowly and respond well to endocrine (anti-estrogen) therapy. Their Achilles' heel is also their vulnerability: starve them of estrogen signaling and many of them stall.
- HER2-positive (HER2+) — about 15–20% of cases. These tumors over-produce the HER2 protein, which acts like a stuck accelerator pedal for cell growth. HER2+ disease was historically aggressive, but the arrival of HER2-targeted drugs such as trastuzumab transformed it into one of the more treatable subtypes.
- Triple-negative (TNBC) — about 10–15% of cases. These tumors lack all three receptors, so neither endocrine therapy nor HER2 drugs work against them. TNBC tends to be more aggressive, strikes younger women and Black women disproportionately, and is the subtype most strongly linked to BRCA1 mutations. Chemotherapy and, increasingly, immunotherapy are the mainstays.
This is why "What stage is it?" is only half the question. "What subtype is it?" is the other half — and it is the one that determines which drugs can even be brought to bear.
4. Etiology and Risk Factors
Breast cancer arises from a mix of factors you cannot change and a smaller set you can. It helps to separate the two honestly, because a lot of guilt and fear comes from believing the disease is fully self-inflicted — it usually is not.
Factors you cannot change:
- Age. The single biggest risk factor. Risk rises steadily across adult life.
- Being a woman. Female sex is the dominant risk factor; men are at far lower (but not zero) risk.
- Inherited gene mutations. About 5–10% of breast cancers are hereditary. BRCA1 and BRCA2 are the best known — a woman with a harmful BRCA1 mutation has roughly a 55–72% lifetime risk, and BRCA2 carriers about 45–69%. Other genes (PALB2, TP53, CHEK2, ATM, PTEN, CDH1) also raise risk to varying degrees.
- Family and personal history. A first-degree relative (mother, sister, daughter) with breast cancer roughly doubles risk. A prior breast cancer or certain prior biopsy findings (such as atypical hyperplasia or lobular carcinoma in situ) also raise it.
- Lifetime estrogen exposure. Starting periods early (before 12), reaching menopause late (after 55), and never having been pregnant all modestly increase risk by extending exposure to estrogen.
- Dense breast tissue. Women with dense breasts have a higher risk and, separately, mammograms are harder to read because dense tissue and tumors both appear white.
Factors you can influence:
- Alcohol. One of the clearest modifiable links. Even light drinking raises risk; each daily drink increases relative risk by roughly 7–10%. This is a real, dose-dependent effect, not a rounding error.
- Excess weight after menopause. After menopause, fat tissue becomes a major source of estrogen, so obesity raises risk specifically for postmenopausal, hormone-receptor-positive disease.
- Physical inactivity. Regular exercise lowers risk, partly by influencing hormones, insulin, and body weight.
- Menopausal hormone therapy. Combined estrogen-plus-progestin therapy taken for several years modestly increases risk; estrogen-alone therapy (for women without a uterus) carries a smaller and more complicated effect. This is a genuine trade-off to discuss with a clinician — see Menopause & HRT.
- Reproductive history. Having children, especially earlier in life, and breastfeeding for a longer total duration are associated with somewhat lower risk.
Genetic testing — who should consider it? Testing for BRCA1/2 and related genes is recommended for people with a personal or family history that raises the odds of an inherited mutation. Red flags include: breast cancer diagnosed at age 45 or younger; triple-negative breast cancer at 60 or younger; a personal history of ovarian, pancreatic, or metastatic prostate cancer; multiple relatives with breast, ovarian, pancreatic, or prostate cancer; a known mutation in the family; or Ashkenazi Jewish ancestry with any of these. A positive result changes screening, opens the door to risk-reducing surgery, and unlocks specific drugs (PARP inhibitors). Genetic counseling before and after testing is standard and worth insisting on.
5. Clinical Presentation
The most common first sign is a new, painless lump in the breast or armpit — typically firm, with irregular edges, and fixed rather than freely mobile. But many breast cancers today are found on screening mammograms before any lump can be felt, which is precisely the point of screening.
Symptoms that warrant prompt evaluation include:
- A new lump or thickening in the breast or underarm.
- Skin changes — dimpling or puckering (sometimes described as an "orange peel" texture), redness, or scaling.
- Nipple changes — a nipple turning inward, or new discharge, especially if bloody and from one duct.
- A change in the size or shape of one breast.
- Persistent breast or nipple pain (less commonly a cancer sign, but worth checking).
Two presentations deserve special mention. Inflammatory breast cancer is a rare, aggressive form that causes the breast to become red, warm, swollen, and tender over days to weeks — often without a discrete lump. It is frequently mistaken for an infection (mastitis); if a presumed breast infection does not clear quickly on antibiotics, it must be re-evaluated. Paget disease of the breast shows up as eczema-like scaling, crusting, or itching of the nipple and can signal an underlying cancer. The reassuring counterpoint: most breast lumps and most breast pain are not cancer. But a new, persistent change should always be checked rather than watched.
6. Diagnosis
Diagnosing breast cancer is a sequence: image it, sample it, then characterize it.
Imaging. A diagnostic mammogram (more detailed than the screening version) is usually first, often paired with ultrasound, which is especially useful for telling fluid-filled cysts from solid masses and for guiding biopsies. Breast MRI is added in selected situations — high-risk patients, dense breasts, lobular cancers, or when surgeons need to map disease extent. Imaging can strongly suggest cancer, but it cannot prove it.
Biopsy — the only way to confirm cancer. A core-needle biopsy, usually guided by ultrasound or mammography, removes small cylinders of tissue for the pathologist. This is an office procedure under local anesthesia, not surgery. The biopsy does two jobs: it confirms whether cancer is present (and whether it is in situ or invasive), and it provides the tissue needed for the all-important receptor testing.
Receptor testing — reading the tumor's biology. On the biopsy tissue, the lab measures:
- ER and PR status — positive or negative, by immunohistochemistry.
- HER2 status — by immunohistochemistry and, when borderline, by FISH to count gene copies.
- Ki-67 — a marker of how fast the tumor is proliferating.
These results define the subtype and therefore the treatment options. Do not be surprised if it takes a week or two for the full panel to come back; the receptor results are worth the wait.
Genomic assays — who can safely skip chemotherapy? For many early-stage, hormone-receptor-positive, HER2-negative cancers, a tumor-gene test such as Oncotype DX (a 21-gene assay) or MammaPrint (70 genes) estimates the risk of recurrence and, crucially, whether adding chemotherapy is likely to help. The landmark TAILORx trial showed that women with a mid-range Oncotype score (11–25) generally gained no benefit from chemotherapy over endocrine therapy alone — sparing tens of thousands of women each year the toxicity of chemo they did not need. This is one of the clearest examples of precision medicine improving lives by doing less.
Staging. Once cancer is confirmed, staging combines tumor size (T), lymph-node involvement (N), and any distant spread (M), now integrated with the receptor results and grade. Lymph nodes are assessed surgically, usually by a sentinel lymph node biopsy — removing just the first node or two that drain the tumor, which spares most women the lymphedema risk of removing all the underarm nodes. For early-stage disease without symptoms, extensive scans (CT, bone scan, PET) are usually not needed and are deliberately avoided.
7. Treatment
Treatment is built around two questions: how far has it spread (stage) and what is it made of (subtype). Most early breast cancer is treated with some combination of surgery, radiation, and "systemic" drug therapy chosen by subtype. A multidisciplinary team — surgeon, medical oncologist, radiation oncologist, pathologist — typically maps out the sequence together.
Surgery: lumpectomy vs. mastectomy. One of the most reassuring facts in oncology, established by the NSABP B-06 trial led by Bernard Fisher and confirmed at 20 years, is that breast-conserving surgery (lumpectomy) plus radiation gives the same long-term survival as mastectomy for most early breast cancers. The Italian Veronesi trial reached the identical conclusion. This means many women have a genuine choice. Lumpectomy removes the tumor and a rim of normal tissue and is almost always paired with radiation; mastectomy removes the whole breast and may avoid radiation but is bigger surgery. Neither is "more aggressive" in the sense of curing more cancer — the choice rests on tumor size and location, breast size, genetics, and personal preference. For BRCA carriers or those wanting to avoid radiation, mastectomy (often with reconstruction) may be preferred.
Radiation therapy. After lumpectomy, radiation to the remaining breast substantially lowers the chance the cancer comes back in that breast. Large analyses by the Early Breast Cancer Trialists' Collaborative Group show radiation roughly halves the recurrence rate and improves long-term survival. Modern regimens are shorter ("hypofractionated") than the older 5–6 weeks, and partial-breast techniques are options for selected low-risk tumors.
Now the drug therapy — chosen entirely by subtype:
HR+/HER2− (hormone-driven): The cornerstone is endocrine therapy, which blocks estrogen's effect or production, taken for 5 to 10 years:
- Tamoxifen blocks the estrogen receptor and is used in pre- and postmenopausal women.
- Aromatase inhibitors (AIs) — anastrozole, letrozole, exemestane — block estrogen production in tissues and are used in postmenopausal women, where they slightly outperform tamoxifen.
- For higher-risk or metastatic HR+ disease, CDK4/6 inhibitors (palbociclib, ribociclib, abemaciclib) added to endocrine therapy markedly delay progression; the PALOMA-2 trial showed palbociclib plus letrozole roughly doubled the time before the cancer advanced.
Chemotherapy is added selectively — often guided by an Oncotype DX or MammaPrint score rather than given to everyone.
HER2+ : The breakthrough drug is trastuzumab (Herceptin), an antibody that targets the HER2 protein. The pivotal adjuvant trials (including the one reported by Romond and colleagues) showed adding trastuzumab to chemotherapy cut recurrence roughly in half — a result that genuinely rewrote the prognosis of this subtype. Pertuzumab, the antibody-drug conjugate T-DM1, and newer agents like trastuzumab deruxtecan have built further on that foundation.
Triple-negative (TNBC): Without hormone or HER2 targets, chemotherapy remains central. The major recent advance is immunotherapy: adding the checkpoint inhibitor pembrolizumab to chemotherapy before surgery (the KEYNOTE-522 regimen) improves outcomes in early high-risk TNBC, and pembrolizumab plus chemotherapy is standard for many PD-L1-positive metastatic TNBCs. For patients with BRCA mutations, PARP inhibitors (olaparib, talazoparib) exploit the tumor's defective DNA repair.
DCIS (stage 0). Because it cannot spread while in situ, DCIS is treated more conservatively — typically lumpectomy, often with radiation, and endocrine therapy if it is hormone-receptor positive. The honest tension here is overtreatment: some DCIS would never have progressed, but because we cannot yet tell which, most is still treated. Active-monitoring trials are underway to answer this.
8. Complications
Surviving breast cancer is the goal, but survivorship comes with its own challenges that deserve honest attention — and most are manageable once you know to look for them.
- Lymphedema. Removing or irradiating underarm lymph nodes can cause chronic arm swelling. Sentinel node biopsy has greatly reduced this risk, but it still affects a meaningful minority. Early referral to a lymphedema therapist, compression sleeves, and exercise help; it is far easier to manage early than late.
- Aromatase-inhibitor joint pain and bone loss. AIs commonly cause aching, stiff joints (arthralgia) — sometimes severe enough that women want to stop the drug. They also accelerate bone loss, so bone-density monitoring and sometimes bone-protective medication are part of care. Exercise, switching among the three AIs, and duloxetine can ease the joint pain; do not suffer silently or quit without telling your oncologist, because there are real options.
- Menopausal symptoms and fertility. Chemotherapy and endocrine therapy can trigger or worsen hot flashes, vaginal dryness, and early menopause. Younger women should discuss fertility preservation before treatment begins — see Infertility.
- Heart effects. Trastuzumab and some chemotherapies can affect heart function, so cardiac monitoring is built into HER2-targeted treatment.
- Cognitive changes ("chemo brain"). Many patients notice memory and concentration difficulties during and after treatment. These are real, usually improve over time, and are not "all in your head."
- Emotional impact. Anxiety, depression, fear of recurrence, and changes in body image and sexuality are common and treatable. Survivorship is not only about the body.
9. Prognosis
Here are the survival numbers stated plainly, because vague reassurance helps no one. US five-year relative survival by how far the cancer has spread at diagnosis:
- Localized (confined to the breast): about 99%.
- Regional (spread to nearby lymph nodes/structures): about 86%.
- Distant (metastatic — spread to bones, liver, lungs, or brain): about 31%.
Two honest caveats sit beside these figures. First, subtype matters enormously — a small HR+ tumor and a triple-negative tumor of the same size do not carry the same outlook, and these averages blur that. Second, survival statistics are several years old by the time they are published and therefore understate the benefit of the newest drugs; a woman diagnosed with metastatic disease today has more options than the "31%" cohort did. Metastatic breast cancer is generally not curable, but for many people it has become a chronic, treatable condition managed over years — see Metastatic Cancers.
Male breast cancer. Men account for under 1% of cases and are usually diagnosed at an older age and, unfortunately, a later stage — partly because neither men nor clinicians expect it. The great majority of male breast cancers are hormone-receptor positive, so tamoxifen is a mainstay. Stage for stage, men and women have broadly similar outcomes; the survival gap in men largely reflects later diagnosis. Any new breast lump in a man should be evaluated, not dismissed.
10. Prevention
No habit guarantees you will not get breast cancer — much of the risk is age and genetics, which no lifestyle can erase. But several measures genuinely lower the odds, and it is worth being honest about how strong the evidence is for each.
- Limit alcohol. This is the modifiable factor with the clearest, most consistent evidence. Risk rises with each daily drink, and there is no clearly "safe" threshold. Cutting back lowers risk in a dose-dependent way.
- Be physically active. Regular exercise is associated with roughly a 10–20% lower risk and benefits both prevention and recovery. See Exercise.
- Maintain a healthy weight, especially after menopause. Because fat tissue produces estrogen after menopause, avoiding excess weight specifically lowers postmenopausal HR+ risk. See Obesity.
- Breastfeed if you can. Longer total breastfeeding is associated with modestly lower risk — a real but small effect.
- Be thoughtful about menopausal hormone therapy. If used, the lowest effective dose for the shortest needed time is the standard approach; discuss the trade-offs individually.
For high-risk women, prevention goes further. Risk-reducing medication — tamoxifen or raloxifene before menopause, an AI after — can cut risk substantially in women at elevated risk, as the NSABP P-1 prevention trial first demonstrated for tamoxifen. For BRCA carriers, risk-reducing mastectomy lowers breast cancer risk by about 90%, and risk-reducing removal of the ovaries and tubes lowers both ovarian and breast cancer risk. These are major decisions made with genetic counseling and a high-risk clinic.
Screening is not prevention, but it is how lives are saved. Mammography does not stop cancer from forming; it finds it earlier, when treatment is gentler and survival far higher. Current US guidance has converged: the USPSTF now recommends screening mammography every other year starting at age 40 for average-risk women (its 2024 update lowered the start age from 50). Other groups suggest annual screening or starting at 40–45; the practical takeaway is that screening should begin by 40 for most women, with timing individualized for those at higher risk (who may start earlier and add MRI).
The honest part about overdiagnosis. Screening has a real downside that is too rarely explained: it finds some cancers — particularly some DCIS and slow-growing tumors — that would never have caused harm in a person's lifetime. Because we cannot reliably tell those apart from dangerous ones, they get treated anyway. This overdiagnosis means some women undergo surgery, radiation, or endocrine therapy for a "cancer" that would never have hurt them. Screening also produces false alarms that lead to extra imaging and biopsies. None of this means screening is not worth it — for the population it clearly reduces deaths — but you deserve to know that the benefit comes with genuine trade-offs, so you can make an informed choice rather than a reflexive one.
11. Recent Research and Advances
Breast cancer research is moving quickly, and several advances have already changed everyday care:
- De-escalation — doing less, safely. The TAILORx and RxPONDER trials used the Oncotype DX gene test to identify large groups of HR+ women who can skip chemotherapy with no loss of survival. The trend across the field is toward giving each patient exactly as much treatment as her tumor's biology requires — and no more.
- Antibody-drug conjugates (ADCs). These "smart bombs" link a targeting antibody to a potent chemotherapy payload. Trastuzumab deruxtecan has shown striking results, including in tumors with only low levels of HER2 — creating a brand-new "HER2-low" category that didn't exist a few years ago. Sacituzumab govitecan has improved outcomes in metastatic triple-negative and HR+ disease.
- Immunotherapy for TNBC. Adding checkpoint inhibitors such as pembrolizumab to chemotherapy (the KEYNOTE-522 approach before surgery; first-line combinations in PD-L1-positive metastatic disease) has improved outcomes in the subtype that most needed new options.
- PARP inhibitors and targeted pills for HR+ disease. PARP inhibitors help BRCA-mutated cancers, and drugs targeting the PIK3CA and AKT pathways (and oral SERDs like elacestrant for ESR1-mutated disease) extend options when standard endocrine therapy stops working.
- Liquid biopsies. Blood tests that detect circulating tumor DNA are being studied to catch recurrence earlier and to guide whether and when to change therapy — potentially before scans show anything.
The throughline of all of this is precision: matching the right drug to the specific molecular machinery of an individual tumor, while sparing people treatment they don't need.
12. References & Research
Historical Background
For most of the twentieth century, breast cancer surgery was governed by the Halsted radical mastectomy — a disfiguring operation removing the breast, chest muscles, and underarm nodes, built on the belief that more extensive surgery meant more cures. That doctrine was overturned by the careful randomized trials of Bernard Fisher and the National Surgical Adjuvant Breast and Bowel Project (NSABP), whose B-06 trial proved that lumpectomy plus radiation matched mastectomy for survival — a finding confirmed at 20 years and mirrored by Umberto Veronesi's parallel Italian work, sparing millions of women the larger operation. The same era established the power of systemic therapy: tamoxifen brought hormone blockade into routine use, and the NSABP P-1 trial later showed it could even prevent breast cancer in high-risk women. The discovery of the BRCA1 (1994) and BRCA2 (1995) genes opened the door to hereditary risk testing, and the 1998 approval of trastuzumab ushered in the targeted-therapy era, transforming HER2-positive disease from one of the worst prognoses to one of the most treatable.
Key Research Papers
- Fisher B, Anderson S, Bryant J, et al. Twenty-Year Follow-up of a Randomized Trial Comparing Total Mastectomy, Lumpectomy, and Lumpectomy plus Irradiation for the Treatment of Invasive Breast Cancer. New England Journal of Medicine. 2002;347(16):1233-1241.
- Veronesi U, Cascinelli N, Mariani L, et al. Twenty-Year Follow-up of a Randomized Study Comparing Breast-Conserving Surgery with Radical Mastectomy for Early Breast Cancer. New England Journal of Medicine. 2002;347(16):1227-1232.
- Early Breast Cancer Trialists' Collaborative Group (EBCTCG). Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women. The Lancet. 2012;379(9814):432-444.
- Early Breast Cancer Trialists' Collaborative Group (EBCTCG). Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: patient-level meta-analysis of randomised trials. The Lancet. 2011;378(9793):771-784.
- Romond EH, Perez EA, Bryant J, et al. Trastuzumab plus Adjuvant Chemotherapy for Operable HER2-Positive Breast Cancer. New England Journal of Medicine. 2005;353(16):1673-1684.
- Cameron D, Piccart-Gebhart MJ, Gelber RD, et al. 11 years' follow-up of trastuzumab after adjuvant chemotherapy in HER2-positive early breast cancer (HERA trial). The Lancet. 2017;389(10075):1195-1205.
- Sparano JA, Gray RJ, Makower DF, et al. Adjuvant Chemotherapy Guided by a 21-Gene Expression Assay in Breast Cancer (TAILORx). New England Journal of Medicine. 2018;379(2):111-121.
- Kalinsky K, Barlow WE, Gralow JR, et al. 21-Gene Assay to Inform Chemotherapy Benefit in Node-Positive Breast Cancer (RxPONDER). New England Journal of Medicine. 2021;385(25):2336-2347.
- Finn RS, Martin M, Rugo HS, et al. Palbociclib and Letrozole in Advanced Breast Cancer (PALOMA-2). New England Journal of Medicine. 2016;375(20):1925-1936.
- Schmid P, Adams S, Rugo HS, et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer (IMpassion130). New England Journal of Medicine. 2018;379(22):2108-2121.
- Schmid P, Cortes J, Dent R, et al. Event-free Survival with Pembrolizumab in Early Triple-Negative Breast Cancer (KEYNOTE-522). New England Journal of Medicine. 2022;386(6):556-567.
- Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for Prevention of Breast Cancer: Report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. Journal of the National Cancer Institute. 1998;90(18):1371-1388.
- US Preventive Services Task Force. Screening for Breast Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2024;331(22):1918-1930.
Research Papers
The links below open live PubMed searches so you can read the most recent peer-reviewed studies on each aspect of breast cancer. Searches are updated continuously as new research is published.
- Breast cancer molecular subtypes
- Triple-negative breast cancer immunotherapy
- HER2-positive breast cancer and trastuzumab
- BRCA1/BRCA2 and breast cancer risk
- CDK4/6 inhibitors in breast cancer
- Aromatase inhibitors as adjuvant therapy
- Oncotype DX recurrence score
- Mammography screening and overdiagnosis
- Ductal carcinoma in situ management
- Breast cancer survivorship and lymphedema
- Alcohol and breast cancer risk
- Antibody-drug conjugates in breast cancer
Connections
- How Cancer Spreads (Metastasis) — interactive animation
- How Genes Are Switched On and Off — interactive animation
- Mitosis: How One Cell Becomes Two — interactive animation
- How Your DNA Is Repaired — and Why It Fails in Cancer — interactive animation
- The Cell Cycle & How Cancer Hijacks It — interactive animation
- Cancer — Overview
- Metastatic Cancers
- Lymphoma
- Menopause & HRT
- HRT Risks: Breast Cancer, Clots, and Stroke
- Non-Hormonal Options for Hot Flashes (SSRIs, Gabapentin, Fezolinetant)
- Perimenopause
- Uterine Fibroids
- Infertility
- Obesity
- Insulin Resistance
- Vitamin D3
- Exercise
- Sulforaphane
- Resveratrol
- Broccoli
- Iodine for Breast Health — mammary iodine concentration, fibrocystic disease, and the Japan incidence hypothesis.