Iodine for Breast Health
Breast tissue is the body's second most avid iodine-concentrating organ after the thyroid. The mammary gland expresses both the sodium-iodide symporter (NIS) and the pendrin transporter, and the lactating breast actively concentrates iodide to deliver it to the nursing infant at a rate of 75-200 µg per day. But the breast also uses molecular iodine (I₂) for purposes that have nothing to do with infant nutrition — as an antioxidant in lipid-rich ductal epithelium, as a substrate for iodolactone formation that activates PPAR-γ and promotes apoptosis of pre-neoplastic cells, and as a modulator of estrogen receptor expression. The clinical signature of this biology is the long-running observation that women in Japan, where dietary iodine intake from seaweed and seafood ranges from 1,000-3,000 µg/day, have among the lowest breast cancer rates in the world, and that this protection is lost within one to two generations when Japanese families migrate to Western countries and adopt Western iodine intake. The therapeutic evidence is strongest for fibrocystic breast disease, where the 1993 Ghent randomized trial in the Canadian Journal of Surgery established molecular iodine as a safe and effective treatment.
Table of Contents
- Breast Tissue as the Second Iodine-Concentrating Organ
- NIS and Pendrin in the Mammary Gland
- Eskin's Animal Data — Deficiency to Dysplasia to Neoplasia
- Fibrocystic Breast Disease — Clinical Presentation
- The Ghent 1993 Molecular Iodine Trial
- The Aceves Group — Iodolactones and Apoptosis
- The Japan Low-Breast-Cancer-Rate Hypothesis
- The Dosing Controversy — Iodide vs Molecular Iodine
- Practical Clinical Recommendations
- Key Research Papers
- Connections
- Featured Videos
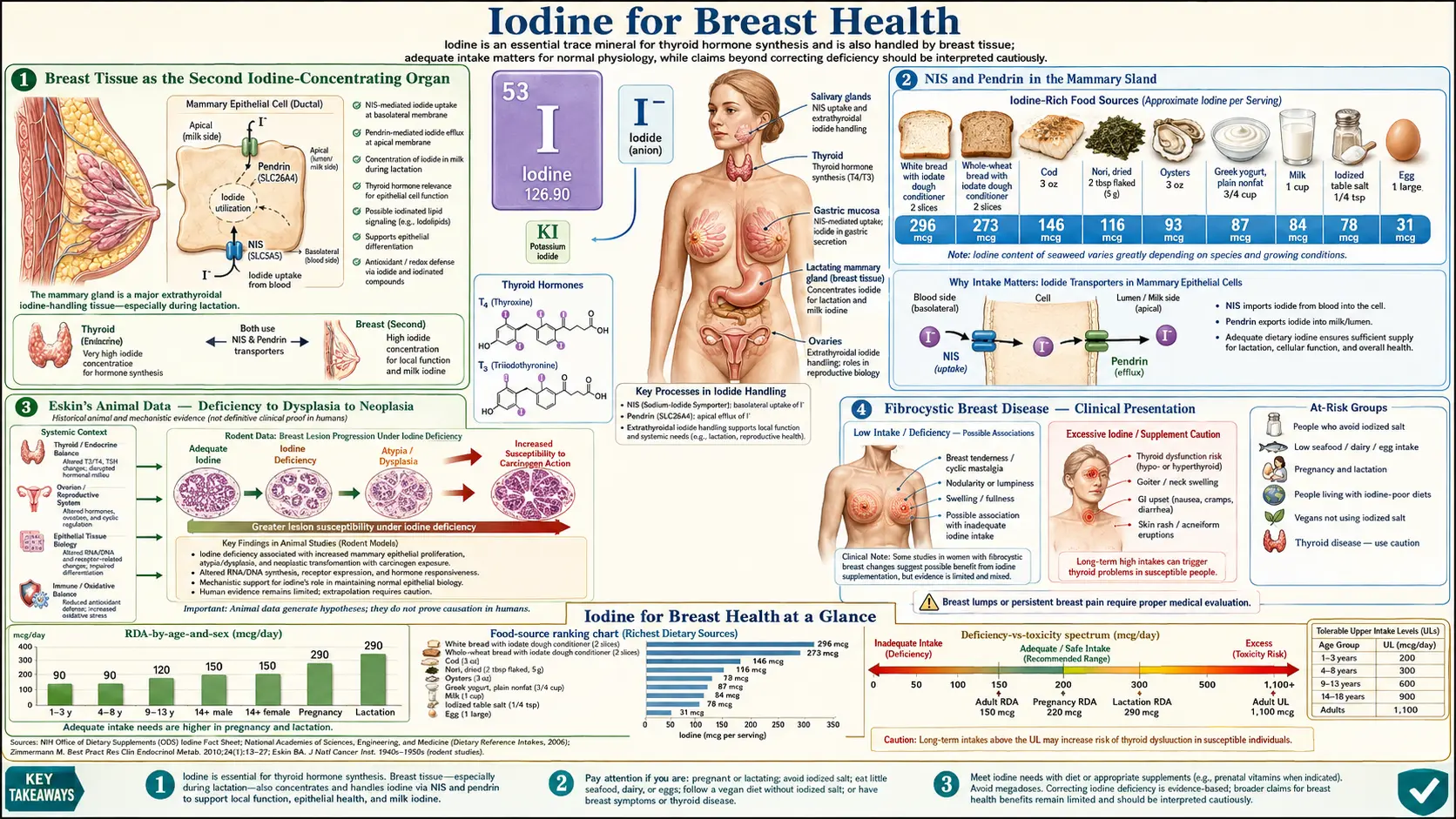
Breast Tissue as the Second Iodine-Concentrating Organ
Among extra-thyroidal tissues, breast tissue is the most avid iodine concentrator in the human body. The concentration is dramatically upregulated during pregnancy and lactation, when the breast must transfer iodine to the nursing infant. But the breast continues to express the sodium-iodide symporter (NIS) and the pendrin transporter throughout adulthood, including in non-lactating and post-menopausal women. The biological purpose of this baseline non-lactating expression has been a topic of considerable research, and the emerging consensus is that local iodine concentration serves protective functions in the ductal epithelium independent of any role in infant nutrition.
The mammary ductal-lobular system is uniquely vulnerable to oxidative and proliferative stress. Estrogen drives ductal epithelial proliferation through every menstrual cycle. The epithelium is lipid-rich (because milk is largely lipid by mass) and therefore vulnerable to lipid peroxidation. The terminal ductal-lobular units are the anatomical origin site for most breast cancers, particularly in the hormone-receptor-positive subtypes. Local iodine concentration provides three distinct protective mechanisms in this environment:
- Direct antioxidant scavenging — molecular iodine (I₂) is itself a reducing agent that can neutralize reactive oxygen species and quench lipid peroxidation reactions
- Iodolactone formation — molecular iodine reacts with arachidonic acid to form 6-iodo-5-hydroxy-eicosatrienoic acid (6-IL, an iodolactone) that activates PPAR-γ nuclear receptors and induces apoptosis in pre-neoplastic and neoplastic ductal cells
- Estrogen-pathway modulation — molecular iodine reduces estrogen receptor alpha (ERα) expression and reduces estrogen-responsive gene transcription, effectively dampening the proliferative drive of cyclic estrogen on ductal epithelium
NIS and Pendrin in the Mammary Gland
The mammary gland expresses two iodide transporters with distinct functions:
- Sodium-iodide symporter (NIS, encoded by SLC5A5) — the same active iodide-concentrating transporter expressed in the thyroid. Mammary NIS is strongly upregulated during pregnancy and lactation under prolactin and oxytocin signaling, and is responsible for the active concentration of iodide into milk.
- Pendrin (encoded by SLC26A4) — a chloride-iodide exchanger originally identified in the thyroid (where its mutation causes Pendred syndrome, combined deafness with goiter), also expressed in the mammary gland.
The pharmacologic question of "iodide vs molecular iodine" in breast health is partially answered by NIS biology. NIS transports iodide (I⁻) and does not transport molecular iodine (I₂) directly. Yet molecular iodine appears to be the species responsible for many of the antioxidant and apoptotic effects observed in breast tissue. The current understanding is that:
- Iodide enters the breast cell via NIS
- Once intracellular, iodide can be oxidized to molecular iodine by local peroxidases (the lactoperoxidase system is particularly relevant in the lactating breast)
- Molecular iodine can also enter the breast cell via passive diffusion (unlike charged iodide, neutral molecular iodine crosses lipid membranes without a transporter)
- The molecular iodine fraction is what reacts with arachidonic acid to form iodolactones
This biology has practical implications for supplementation. Pure potassium iodide (KI) delivers only iodide; the breast must oxidize it locally to produce the molecular iodine that drives the apoptosis-promoting iodolactone pathway. Lugol's solution and Iodoral deliver both iodide and molecular iodine, which is the basis for the integrative-medicine preference for these formulations in breast indications. Sea-vegetable iodine is primarily iodide.
Eskin's Animal Data — Deficiency to Dysplasia to Neoplasia
Bernard Eskin's laboratory at Hahnemann Medical College in Philadelphia produced a series of landmark animal studies from the late 1960s through the 1980s establishing the histological progression of iodine-deficiency-related breast pathology in rat models. The findings:
- Rats fed iodine-deficient diets developed mammary ductal hyperplasia within 6-8 weeks
- Sustained deficiency progressed to atypical ductal hyperplasia (a recognized pre-malignant lesion in human breast pathology)
- Animals exposed to chemical carcinogens (such as 7,12-dimethylbenzanthracene, DMBA) in combination with iodine deficiency developed mammary tumors at substantially higher rates than iodine-replete controls receiving the same carcinogen dose
- Iodine repletion — particularly with molecular iodine rather than iodide alone — reversed early ductal hyperplasia and reduced subsequent tumor incidence
- The histological pattern of iodine-deficient rat mammary dysplasia closely resembled the human pathology of fibrocystic breast disease, suggesting a mechanistic link
Eskin's work established the conceptual framework for thinking about iodine as a breast-tissue protective factor and provided the laboratory rationale for the subsequent human clinical trials of molecular iodine in fibrocystic breast disease.
Fibrocystic Breast Disease — Clinical Presentation
Fibrocystic breast disease (FBD), also called fibrocystic change or benign breast disease, is the most common benign breast condition in women of reproductive age. Estimated prevalence is 50-90% of women at some point in life. The clinical presentation:
- Bilateral breast pain (mastalgia), often cyclic with the menstrual cycle (worse in the week before menses, improves after menses)
- Palpable, often tender, mobile breast nodules — typically rope-like or fine-nodular density rather than discrete dominant masses
- The upper outer quadrants of both breasts are most commonly affected
- Breast swelling and a sensation of heaviness or fullness
- Nipple discharge can occur (usually clear or pale yellow; bloody discharge requires evaluation for malignancy)
- Symptoms typically begin in the early-to-middle reproductive years and persist or worsen through perimenopause, often improving substantially after menopause when estrogen drive declines
The condition is not pre-malignant in the conventional sense — the simple fibrocystic change does not carry meaningfully elevated breast cancer risk on its own. However, certain histological subtypes (particularly proliferative changes with atypia) do confer increased risk, and the persistent inflammation and ductal dilation of long-standing fibrocystic disease may create a tissue environment that is more permissive to malignant transformation.
The conventional medical approach to fibrocystic breast disease has included: caffeine restriction (modest benefit in some women, no benefit in others), evening primrose oil (mixed evidence), oral contraceptives (suppress cyclic hormone fluctuation), danazol (a synthetic androgen that suppresses estrogen, with side effects that limit use), tamoxifen (estrogen receptor antagonist, reserved for severe cases), and reassurance plus symptomatic management with ibuprofen and warm compresses. Iodine has historically been overlooked in conventional management, despite a decades-old evidence base for benefit.
The Ghent 1993 Molecular Iodine Trial
William R. Ghent, a Canadian surgeon, conducted a series of trials of iodine supplementation in fibrocystic breast disease through the 1970s and 1980s. The seminal publication is Ghent et al. (1993) in the Canadian Journal of Surgery, which combined the results of three earlier observational studies with a prospective randomized trial. Findings:
- Three open-label uncontrolled studies (1,365 patients total): clinical improvement (reduction in breast pain and nodularity) in 70%-72% of women treated with molecular iodine; 40%-44% of women treated with sodium iodide; and minimal improvement in placebo-treated controls
- Randomized double-blind controlled trial (56 patients): molecular iodine arm showed statistically significant clinical and ultrasound improvement compared to placebo; placebo response was modest
- Side effects were minimal at doses of 0.07-0.09 mg molecular iodine per kg body weight per day (approximately 5-7 mg for an average adult woman)
- Onset of clinical benefit typically began within 2-3 months of supplementation initiation; full effect at 6-12 months
The Ghent trial established molecular iodine as a clinically validated treatment for fibrocystic breast disease. The trial was small by modern standards and would benefit from replication in larger, longer-duration randomized studies, but the magnitude of the clinical effect and the consistency across the four reported study populations have supported the integrative-medicine adoption of molecular iodine for breast indications.
A subsequent prospective randomized trial by Kessler (2004) tested molecular iodine at 1.5, 3, and 6 mg/day for 6 months in 111 women with documented cyclic mastalgia. The 6 mg/day arm showed statistically significant improvement in pain, nodularity, and tenderness compared to placebo, with mild and self-limiting side effects (mostly transient gastrointestinal symptoms).
The Aceves Group — Iodolactones and Apoptosis
Carmen Aceves and colleagues at the Institute of Neurobiology of the National Autonomous University of Mexico (UNAM) have published the most rigorous mechanistic work on molecular iodine in breast biology over the past two decades. Key findings from this group:
- Molecular iodine (I₂), but not iodide alone, induces apoptosis in human breast cancer cell lines (MCF-7 hormone-receptor-positive, MDA-MB-231 triple-negative) at concentrations achievable with oral supplementation
- The apoptosis is mitochondria-mediated — cytochrome c release, caspase 9 and 3 activation, and Bax/Bcl-2 ratio shift
- The active downstream mediator is 6-iodo-5-hydroxy-8,11,14-eicosatrienoic acid (6-IL, an iodolactone formed when molecular iodine reacts with arachidonic acid)
- 6-IL is a high-affinity ligand for PPAR-γ (peroxisome proliferator-activated receptor gamma), the nuclear receptor known to drive adipocyte differentiation and to promote apoptosis in several cancer cell types
- Pre-treatment with PPAR-γ antagonists blocks the apoptotic effect of molecular iodine on breast cancer cells, confirming PPAR-γ as the principal downstream mediator
- In rat mammary tumor models (DMBA-induced), oral molecular iodine reduces tumor volume and increases tumor cell apoptosis index
- In a 2017 clinical pilot, molecular iodine (5 mg/day for 6 months) reduced Ki-67 proliferation index and increased apoptosis markers in benign breast lesion biopsies
The Aceves group has also explored iodine as an adjunct to standard chemotherapy in breast cancer. In animal models, molecular iodine appears to sensitize breast tumors to doxorubicin while reducing doxorubicin-related cardiotoxicity. A small phase II clinical trial in advanced breast cancer patients receiving standard chemotherapy showed that the molecular-iodine arm had improved disease-free survival and reduced chemotherapy side effects. The work is preliminary but biologically plausible and is the basis for ongoing larger trials.
The Japan Low-Breast-Cancer-Rate Hypothesis
Among industrialized countries, Japan has historically had one of the world's lowest age-adjusted breast cancer incidence rates — roughly one-third the U.S. rate at the time of peak divergence in the 1980s. Multiple dietary and lifestyle factors have been proposed as contributors: higher soy isoflavone intake, lower total fat intake, lower meat consumption, higher omega-3 intake from fish, and notably, much higher iodine intake from seaweed and seafood.
The iodine hypothesis is strengthened by migration studies. When Japanese families migrate to Hawaii or the U.S. mainland and adopt American dietary patterns, breast cancer incidence in the next two generations converges with the host-country rate. Conversely, Japanese-American populations who maintain a traditional Japanese diet retain something closer to the original low rate. The convergence is too rapid (one to two generations) to be primarily genetic; it must be largely environmental.
Average Japanese dietary iodine intake estimates vary by study and by population but typically range from 1,000-3,000 µg/day in the general population, with much higher intakes (up to 13,000 µg/day) in subpopulations that consume large amounts of kelp. These intakes are 10-100× the U.S. RDA of 150 µg/day and well into the range that Brownstein and Abraham would describe as physiologically replete rather than minimally sufficient. Japan has not historically shown high rates of iodine-induced hyperthyroidism or thyroid autoimmunity at these intake levels, though some recent data suggests rising thyroid antibody prevalence in some Japanese subpopulations.
The hypothesis remains correlational rather than causal — no randomized trial has shown that Western women supplementing with seaweed-level iodine doses experience reduced breast cancer incidence over a follow-up period long enough to capture the outcome. The biological plausibility (Eskin animal data, Ghent FBD trial, Aceves mechanism) and the epidemiologic consistency are nonetheless substantial enough to inform clinical recommendations for individual patients with breast-cancer risk factors who choose to supplement.
The Dosing Controversy — Iodide vs Molecular Iodine
The optimal form and dose of iodine for breast-tissue indications remains genuinely contested. The positions:
- Conservative (mainstream) — iodine at the RDA level (150 µg/day) is sufficient for thyroid hormone synthesis; higher doses are unnecessary and potentially harmful (Wolff-Chaikoff effect, Jod-Basedow phenomenon, Hashimoto's trigger). For fibrocystic breast disease, dietary counseling, caffeine restriction, and conventional management are preferred over iodine supplementation.
- Moderate (integrative) — molecular iodine at 3-12.5 mg/day (Lugol's drops or Iodoral tablets) for women with symptomatic fibrocystic breast disease or strong breast-cancer family history. Selenium 200 mcg/day as obligate cofactor. Monitor TSH, free T4, and TPO antibodies at 3-month intervals during titration.
- Brownstein protocol — molecular iodine plus iodide at 25-50 mg/day for both breast and whole-body iodine repletion. Iodine loading test at baseline to document deficiency before high-dose initiation. Selenium 200-400 mcg/day, magnesium, vitamin C, and unrefined salt as full cofactor support. Slower titration (start at 6.25 mg, escalate over weeks).
The pragmatic middle position for most patients: a woman with documented fibrocystic breast disease, no known thyroid autoimmunity, and a strong family history of breast cancer can reasonably consider molecular iodine at 3-12.5 mg/day with selenium 200 mcg/day cofactor support, with TSH monitoring at 3 and 6 months. If the clinical breast symptoms improve and thyroid labs remain stable, the supplementation can be continued long-term. If TSH rises or TPO antibodies appear, the supplementation should be stopped or substantially reduced and re-evaluated.
For a woman without breast-specific indications, the case for high-dose iodine is less compelling and the standard 150-200 µg/day from iodized salt, dairy, eggs, and seafood is generally sufficient. For more on the connection to other iodine-related conditions, see our pages on Hashimoto's Thyroiditis, Cancer, and the related Thyroid Function deep-dive.
Practical Clinical Recommendations
- Symptomatic fibrocystic breast disease, otherwise healthy — molecular iodine 3-12.5 mg/day (Iodoral 12.5 mg tablet or equivalent Lugol's solution) plus selenium 200 mcg/day; expect clinical improvement at 2-6 months; continue indefinitely if effective and labs remain stable
- Strong family history of breast cancer, otherwise healthy — iodized salt plus dairy, eggs, seafood for population-level RDA sufficiency; consider supplemental molecular iodine 3-6 mg/day with selenium 200 mcg/day after baseline TSH and TPO antibody check
- Active breast cancer in treatment — molecular iodine is being investigated as an adjunct but should be coordinated with the treating oncologist; the Aceves data suggesting reduced doxorubicin cardiotoxicity is promising but not yet standard of care
- Pregnancy or lactation — 150-290 µg/day total iodine intake per American Thyroid Association guidance; do not use high-dose Brownstein protocols in pregnancy — the immature fetal thyroid is vulnerable to Wolff-Chaikoff effect from excess maternal iodine
- Documented Hashimoto's thyroiditis — address selenium status first (200-400 mcg/day); reintroduce iodine cautiously at low doses (a few hundred mcg/day) with antibody monitoring at 3-month intervals; do not jump to high-dose protocols without supervision
- Newly diagnosed thyroid nodules — defer high-dose iodine until thyroid imaging and biochemistry are clarified; autonomous nodules can produce iodine-induced hyperthyroidism (Jod-Basedow) on sudden high-dose exposure
- Bromide exposure history — women exposed to commercial baked goods (potassium bromate), brominated flame retardants, brominated vegetable oils, or hot-tub bromine sanitizers may have higher tissue bromide stores that compete with breast iodine uptake; iodine supplementation may produce transient "bromide detox" symptoms (skin rash, metallic taste, headache) that resolve over weeks
Key Research Papers
- Eskin BA et al. (1967). Mammary gland dysplasia in iodine deficiency. JAMA. — PubMed
- Eskin BA (1978). Iodine and mammary cancer. Adv Exp Med Biol. — PubMed
- Ghent WR et al. (1993). Iodine replacement in fibrocystic disease of the breast. Can J Surg. — PubMed
- Kessler JH (2004). The effect of supraphysiologic levels of iodine on patients with cyclic mastalgia. Breast J. — PubMed
- Aceves C, Anguiano B, Delgado G (2005). Is iodine a gatekeeper of the integrity of the mammary gland? J Mammary Gland Biol Neoplasia. — PubMed
- Arroyo-Helguera O et al. (2008). Molecular iodine has extrathyroidal effects as an antioxidant, differentiator, and apoptotic inducer in human breast cancer cells. Endocr Relat Cancer. — PubMed
- Nunez-Anita RE et al. (2009). Iodine modifies the genomic profile of human breast cancer cells. Endocr Relat Cancer. — PubMed
- Smyth PP (2003). The thyroid, iodine and breast cancer. Breast Cancer Res. — PubMed
- Cann SA, van Netten JP, van Netten C (2000). Hypothesis: iodine, selenium and the development of breast cancer. Cancer Causes Control. — PubMed
- Stoddard FR et al. (2008). Iodine alters gene expression in the MCF-7 breast cancer cell line. Int J Med Sci. — PubMed
- Garcia-Solis P et al. (2005). Inhibition of N-methyl-N-nitrosourea-induced mammary carcinogenesis by molecular iodine. Mol Carcinog. — PubMed
- Moreno-Vega A et al. (2019). Adjuvant effect of molecular iodine in conventional chemotherapy for breast cancer. Nutrients. — PubMed
PubMed Topic Searches
- PubMed: Fibrocystic breast disease and iodine
- PubMed: Molecular iodine and breast cancer apoptosis
- PubMed: Iodolactones and PPAR-gamma
- PubMed: Japan seaweed and breast cancer
- PubMed: NIS in breast and lactation
Connections
- Iodine Benefits Hub
- Iodine Overview
- Iodine for Thyroid Function
- Iodine for Brain Development
- Iodine for Metabolism & Energy
- Selenium (cofactor)
- Cancer
- Hashimoto's Thyroiditis
- Thyroid Disorders
- Infertility
- Vitamin D3
- Omega-3 Fatty Acids
- Heavy Metals
- Fluoride
- All Minerals
- Breast Cancer — the malignancy behind the Japan low-incidence and molecular-iodine apoptosis research.