RSV (Respiratory Syncytial Virus)
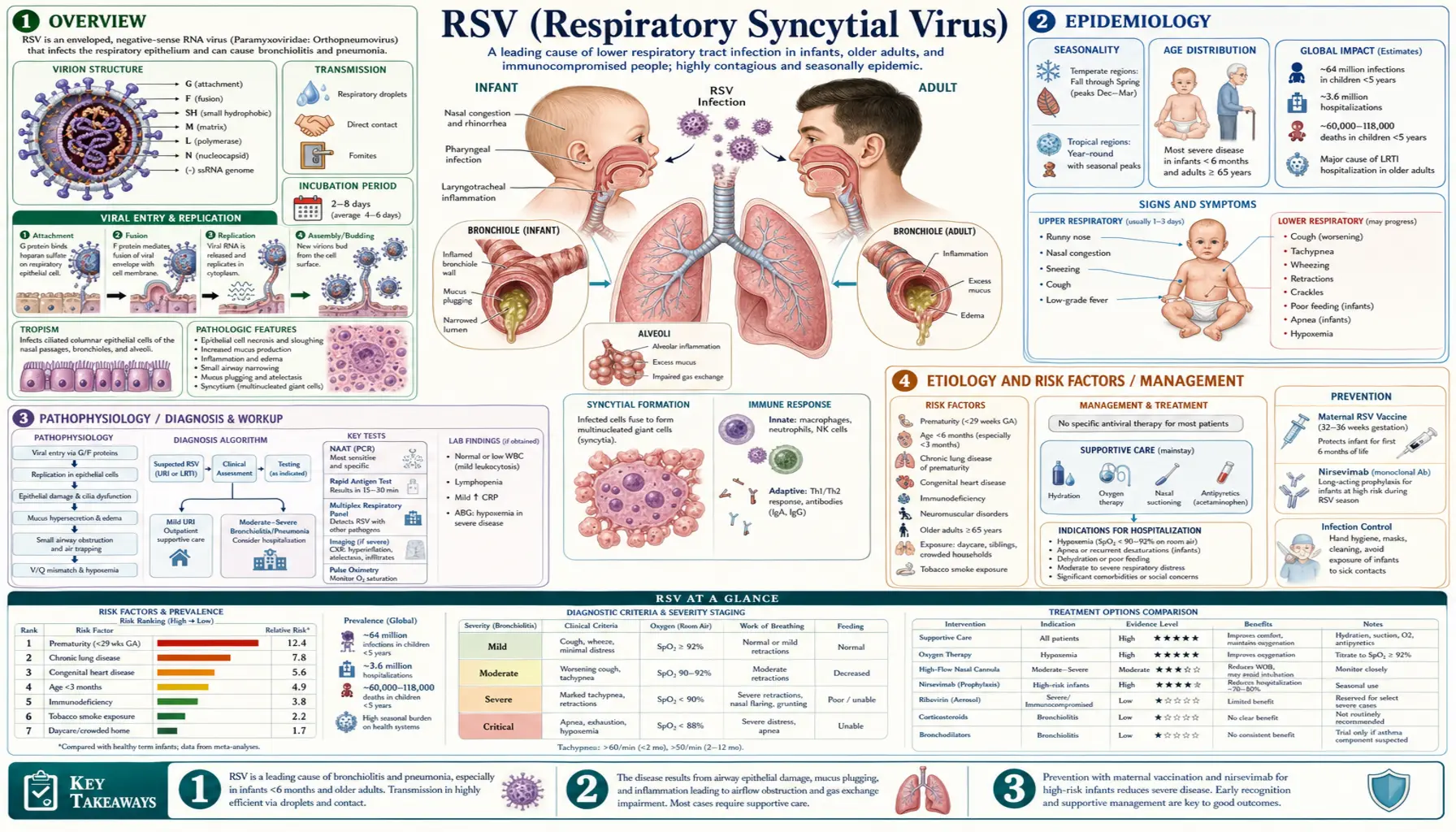
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research and Advances
- Research Papers
- Connections
- Featured Videos
1. Overview
RSV stands for respiratory syncytial virus — a common, contagious virus that infects the lungs and breathing passages. It is so widespread that almost every child catches RSV at least once before their second birthday. For most healthy children and adults, an RSV infection feels like an ordinary head cold: runny nose, cough, mild fever, a few rough days, then recovery. If you have ever had a winter cold that just would not quit, there is a fair chance it was RSV and you never knew it.
So why does RSV get so much attention? Because it leads a double life. In the same season that it gives most people a harmless cold, RSV is a leading cause of hospitalization in babies — the single most common reason infants under one year old end up admitted with breathing trouble — and a serious, sometimes deadly threat to older adults, especially those over 65 or living with heart or lung disease. This page tells both halves of that story plainly, because the same virus that is "no big deal" for a healthy 30-year-old can be a genuine emergency for their newborn or their elderly parent.
There is also genuinely good news to report. After more than half a century with almost nothing to offer beyond supportive care, the years 2022–2023 brought a wave of brand-new tools: a long-acting antibody shot that protects infants through their first RSV season, a vaccine given during pregnancy that passes protection to the newborn, and the first RSV vaccines for older adults. These are not hype — they are real, trial-tested products now in routine use. We cover them honestly in the Prevention and Recent Research sections.
2. Epidemiology
RSV is one of the most common infections on earth. Essentially 100% of children have been infected by age two, and reinfections continue throughout life because immunity from one bout is incomplete and short-lived — you can catch RSV again and again, season after season.
In the United States, RSV is responsible for an estimated 58,000–80,000 hospitalizations in children under five each year, with the highest rates in the youngest infants. Globally, RSV caused roughly 33 million lower-respiratory-tract infections and over 100,000 deaths in children under five in 2019, the vast majority in low- and middle-income countries. It is, after malaria, among the leading infectious killers of infants worldwide.
The older-adult burden was underappreciated for years but is now well documented. RSV causes an estimated 60,000–160,000 hospitalizations and 6,000–10,000 deaths annually among U.S. adults aged 65 and older — numbers in the same range as seasonal influenza in some years. Adults with chronic heart or lung disease, and those who are immunocompromised, carry the heaviest risk.
RSV is strongly seasonal. In most temperate regions it arrives in the fall, peaks in winter (roughly December through February), and fades by spring. In warmer and tropical climates the timing shifts or RSV may circulate much of the year. Knowing the season matters: when local RSV activity is high, a wheezing infant or a struggling older adult is more likely to have RSV, and clinicians factor that into testing and care.
3. Pathophysiology
RSV is an enveloped RNA virus that spreads through respiratory droplets (coughs and sneezes) and through contaminated hands and surfaces — the virus can survive for hours on doorknobs, toys, and countertops. It enters through the eyes, nose, or mouth, then infects the cells lining the airways.
The virus gets its name from a microscope finding: infected cells fuse together into giant multi-nucleated clumps called syncytia (hence "syncytial"). As RSV multiplies, it kills these lining cells, and the body's immune response floods the airway with inflammation, mucus, and shed cellular debris.
In an adult or older child, this damage stays mostly in the upper airway — the result is a runny nose and cough. In a baby, the trouble moves deeper. Here is the key idea, in plain terms: an infant's smallest airways (the bronchioles) are about the width of a thin straw. When RSV inflames their lining and fills them with mucus and dead cells, those tiny tubes get partly plugged. Air can squeeze in but struggles to get back out, the airways narrow and twitch, and the baby starts to wheeze, breathe fast, and work hard for every breath. This is bronchiolitis — the classic serious form of RSV in infants. Because babies breathe through their nose and have such narrow passages, even a modest amount of swelling and snot can make feeding and breathing genuinely difficult.
In older adults, the same virus can light up the lower airways too, triggering or worsening underlying lung and heart conditions (see Complications). The lungs of an 80-year-old with emphysema have far less reserve than a young adult's, so an infection a younger person would shrug off can tip them into a crisis.
4. Etiology and Risk Factors
The cause is straightforward: infection with respiratory syncytial virus, of which there are two main subgroups (A and B) that co-circulate. Anyone can catch it. What separates a mild cold from a dangerous illness is who gets infected. The groups at highest risk of severe RSV are:
- Young infants, especially those under 6 months, and most of all in the first weeks of life.
- Premature babies, whose lungs and immune systems are underdeveloped.
- Infants with congenital heart disease or chronic lung disease of prematurity.
- Adults aged 65 and older, with risk climbing further past 75.
- Adults of any age with chronic conditions — COPD, asthma, heart failure, diabetes, or kidney disease.
- People who are immunocompromised — from transplant, chemotherapy, or immune-suppressing medication.
- Residents of long-term care facilities, where RSV spreads easily and the population is frail.
Things that raise a child's odds of catching RSV in the first place include attending daycare, having older siblings who bring it home, crowded housing, exposure to tobacco smoke, and not being breastfed. None of these cause severe disease by themselves, but several stack the deck.
5. Clinical Presentation
In healthy older children and adults, RSV usually looks like a common cold: runny or stuffy nose, sore throat, cough, sneezing, sometimes a low fever and headache. It typically peaks around days 3–5 and clears within one to two weeks, though the cough can linger.
RSV in babies — what to watch for
An infant with RSV often starts the same way (congestion, mild cough, fussiness, maybe a fever) for a day or two. The concern is whether it moves into the chest as bronchiolitis. Parents, you do not need to diagnose anything — you just need to recognize when breathing is becoming hard work and get help. Seek urgent care right away if your baby shows any of these red flags:
- Fast or labored breathing — counting more than about 60 breaths a minute, or breathing that looks like a struggle.
- Nasal flaring — the nostrils widening with each breath.
- Retractions — the skin pulling in between the ribs, under the ribcage, or at the base of the neck with each breath, as if the body is sucking inward to drag air in.
- Grunting with breaths, or a head that bobs with each breath in a young infant.
- Poor feeding — too breathless to nurse or take a bottle — and fewer wet diapers (a sign of dehydration).
- Pauses in breathing (apnea) — in very young or premature infants, RSV can cause the baby to simply stop breathing for short stretches. This is an emergency.
- A blue or grayish tint to the lips, tongue, or face — call 911.
Trust your instincts. You know your baby. If something feels wrong — if they are listless, gray, dehydrated, or breathing in a way that scares you — do not wait it out. Have them seen.
RSV in older adults — easy to miss
In an older adult, RSV may not look dramatic at first — congestion, cough, fatigue, sometimes low-grade fever. The danger is what it sets off underneath. RSV frequently triggers a flare of an existing condition: a person with COPD may suddenly become much more short of breath and need their rescue inhalers far more often; a person with heart failure may decompensate, retaining fluid and struggling to breathe. New or worsening shortness of breath, confusion, marked weakness, or a sudden inability to manage daily activities in an older adult during RSV season deserves prompt medical attention.
6. Diagnosis
For most people, RSV is diagnosed clinically — the doctor recognizes the pattern (cold symptoms, the season, a wheezing infant or a struggling older adult) and does not need a lab test to start the right supportive care. In a typical healthy child with a mild cold or classic bronchiolitis, testing usually does not change what gets done, and guidelines specifically discourage routine testing and chest X-rays in that situation.
Testing is reserved for when the result will actually change management — for example, to confirm RSV in a hospitalized patient (so they can be grouped with other RSV patients and not given unnecessary antibiotics), in someone severely ill, or in a high-risk person where knowing the exact virus matters. When testing is done, the main tools are:
- PCR (molecular) tests on a nasal swab — the most accurate, and often run as a panel that checks for several respiratory viruses at once.
- Rapid antigen tests — faster and cheaper, very useful in young children (who shed a lot of virus), though less sensitive in adults.
A chest X-ray is not routine; it is used selectively when pneumonia or another complication is suspected. Pulse oximetry — the painless clip on a finger or toe that reads the blood-oxygen level — is one of the most useful bedside measures, helping decide whether a patient needs supplemental oxygen or hospital admission.
7. Treatment
Here is the honest truth that surprises many families: there is no antiviral pill that cures RSV, and for the vast majority of people none is needed. Treatment is supportive — you help the body do its job comfortably while the infection runs its course. For a child or adult recovering at home, that means:
- Plenty of fluids to stay hydrated — small, frequent feeds for babies; sips throughout the day for everyone else.
- Nasal suctioning and saline drops for infants — gently clearing a baby's nose before feeds and sleep can make a real difference, because babies breathe through their nose.
- Rest, fever control with acetaminophen or ibuprofen (ibuprofen only over 6 months), and a humidified or upright environment for comfort.
- Watching the breathing and returning for care if the red flags above appear.
What does NOT help — and why that is okay
It is natural to want a medicine that fixes things. But for typical RSV bronchiolitis, several treatments that seem like they should help have been studied carefully and shown not to work — so good doctors deliberately skip them rather than expose a child to side effects for no benefit:
- Bronchodilators (albuterol and similar inhalers) are not routinely recommended for bronchiolitis. The wheeze in a baby comes from plugged, swollen tiny airways, not the muscle-tightening that these drugs relax — so on average they do not improve the illness.
- Steroids (oral or inhaled) do not shorten or improve typical RSV bronchiolitis in otherwise-healthy infants and are not recommended for it.
- Antibiotics do nothing against a virus. They are withheld unless there is a specific bacterial complication, both to avoid side effects and to keep antibiotics working when they are truly needed.
If your clinician chooses not to prescribe these, that is not them doing less — it is them following the best evidence and protecting your child. (Individual cases, such as a child with known asthma, are judged on their own merits.)
Hospital care, when it is needed
A minority of patients — mostly young infants and frail older adults — need hospital support. Honestly, even in the hospital the care is still mostly supportive but more intensive: supplemental oxygen (and sometimes high-flow nasal oxygen or other breathing support) to keep blood-oxygen levels safe, IV or tube fluids if a baby is too breathless to feed, careful monitoring of breathing and oxygen, and suctioning. Most hospitalized children turn the corner within a few days. The antiviral drug ribavirin exists but is used only rarely, in select severely immunocompromised patients, because its benefit is limited and it is difficult to administer.
8. Complications
Most RSV infections resolve without lasting trouble. When complications do occur, they cluster in the vulnerable groups:
- Severe bronchiolitis and respiratory failure in infants — the airways become so obstructed that the baby cannot maintain oxygen levels and needs hospital breathing support.
- Apnea — dangerous pauses in breathing, particularly in premature and very young infants.
- Pneumonia — RSV can cause viral pneumonia directly, or set the stage for a secondary bacterial infection.
- Dehydration — from poor feeding plus increased fluid loss through fast breathing.
- Ear infections — a common companion to RSV in young children.
- Flares of chronic disease in older adults — RSV is a well-recognized trigger of COPD exacerbations and heart-failure decompensation, which can themselves be life-threatening.
- Possible link to later wheezing/asthma — children who have severe RSV bronchiolitis in infancy have higher rates of recurrent wheezing later in childhood, though whether RSV causes this or simply reveals children already prone to it is still being studied.
9. Prognosis
The outlook for the great majority of people with RSV is excellent. Healthy children and adults recover fully within one to two weeks, often without ever needing to see a doctor. Even most infants hospitalized with bronchiolitis do very well and go home within a few days with no lasting harm.
The serious outcomes — respiratory failure, ICU admission, death — are concentrated in the highest-risk groups: the youngest and most premature infants, and the oldest and sickest adults. For them, RSV is a genuine danger, which is exactly why the new prevention tools described below are such a meaningful advance. A reassuring overall picture for most families should not obscure the real stakes for a 3-week-old or an 85-year-old with heart failure.
10. Prevention
For decades, preventing RSV meant little more than washing hands and hoping. That changed in 2023. There is now a real toolkit, and for the first time most of it works before a baby or older adult ever gets sick. We will report it accurately — these tools are new and genuinely effective, without overpromising that they make RSV vanish.
Protecting infants — the new era
Nirsevimab (brand name Beyfortus) is a long-acting monoclonal antibody — not a vaccine, but a ready-made protective antibody given as a single shot to infants entering their first RSV season (and to certain high-risk toddlers entering their second). Rather than training the baby's immune system, it hands them the protection directly, and one dose lasts through the season. In its pivotal trials (MELODY and the real-world HARMONIE study), nirsevimab reduced RSV-related hospitalizations and medically attended infections by roughly 75–80%. U.S. advisors now recommend it for essentially all infants under 8 months entering their first RSV season.
The maternal RSV vaccine (RSVpreF, brand Abrysvo) takes a different route to the same goal: it is given to the pregnant person at 32–36 weeks of pregnancy, prompting them to make antibodies that cross the placenta and protect the newborn during the riskiest first months of life. In its pregnancy trial (MATISSE), it meaningfully cut severe RSV illness in young infants. A family typically uses one of these two approaches — the maternal vaccine or the infant antibody — to cover the baby's first season.
Palivizumab (Synagis) is the older antibody, in use since 1998. It works but requires monthly injections through the season and was reserved for the highest-risk premature and medically fragile infants. Nirsevimab, with its single longer-lasting dose, has now largely replaced it for most uses, though palivizumab remains part of the story and is still used in some settings.
Protecting older adults — the first RSV vaccines
2023 also brought the first RSV vaccines for adults. Two are available — Arexvy and Abrysvo — both single-dose shots that, in large trials, reduced RSV lower-respiratory illness in older adults by roughly 70–85%. They are recommended for adults 60 and older, with the strongest case (and current routine recommendation) for those 75 and older and for younger adults with risk factors such as chronic heart or lung disease. If you or an older relative falls in these groups, it is worth a conversation with the doctor or pharmacist about getting vaccinated ahead of the fall–winter season.
Everyday prevention — still matters
The basics protect the vulnerable people around you, especially newborns:
- Wash hands often with soap and water before holding a baby.
- Keep sick visitors and tobacco smoke away from infants — ask people with cold symptoms not to hold or kiss a newborn, and keep the home smoke-free.
- Clean high-touch surfaces and toys, since RSV survives on them for hours.
- Breastfeed if you can — breast milk passes along protective antibodies and is linked to milder illness.
- Cover coughs, and keep mildly sick children home from daycare when possible.
11. Recent Research and Advances
RSV research has moved faster in the last few years than in the previous fifty. The breakthrough behind nearly all of today's tools was a basic-science discovery: scientists learned how to lock the virus's surface "fusion" protein into its pre-fusion shape — the form that the immune system best recognizes. Stabilizing the pre-fusion F protein is the engineering trick that finally made effective RSV vaccines and antibodies possible after decades of failure.
From that foundation came the cluster of 2022–2023 approvals: nirsevimab for infants (MELODY, HARMONIE), the maternal RSVpreF vaccine (MATISSE), and the adult vaccines (the AReSVi and RENOIR/MATISSE-family trials). Researchers are now studying how long the adult vaccines' protection lasts and whether a single dose suffices across multiple seasons, how to best combine or choose between the infant strategies, real-world effectiveness as these products roll out at population scale, and next-generation candidates including additional vaccine platforms. Antiviral drugs that directly attack RSV are also in development, though none has yet matched the impact of the prevention tools. For most families the practical headline is simple: after a long wait, there are now real, trial-proven ways to keep the most vulnerable people from getting seriously ill.
12. References & Research
Historical Background
RSV was first isolated in 1956 from chimpanzees with respiratory illness — it was originally called the "chimpanzee coryza agent" — and was soon recognized as a major cause of human infant respiratory disease. The field's most painful and instructive chapter came in the 1960s: an early formalin-inactivated RSV vaccine not only failed to protect children but actually made subsequent natural infections worse, leading to severe enhanced disease and tragic deaths. That disaster, documented by Kim and colleagues in 1969, cast a long shadow and made researchers cautious for decades, delaying RSV vaccine development for a generation. Progress crept forward with the monoclonal antibody palivizumab in 1998, which proved that giving protective antibodies could prevent hospitalizations in high-risk infants. Then, building on the pre-fusion-F discovery, the 2022–2023 wave — nirsevimab for infants, the maternal vaccine, and the first adult vaccines — finally delivered the broad protection that had eluded the field since 1956.
Key Research Papers
- Hall CB, Weinberg GA, Iwane MK, et al. The Burden of Respiratory Syncytial Virus Infection in Young Children. New England Journal of Medicine. 2009;360(6):588-598.
- Li Y, Wang X, Blau DM, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. The Lancet. 2022;399(10340):2047-2064.
- Nair H, Nokes DJ, Gessner BD, et al. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: a systematic review and meta-analysis. The Lancet. 2010;375(9725):1545-1555.
- Falsey AR, Hennessey PA, Formica MA, et al. Respiratory Syncytial Virus Infection in Elderly and High-Risk Adults. New England Journal of Medicine. 2005;352(17):1749-1759.
- Ralston SL, Lieberthal AS, Meissner HC, et al. Clinical Practice Guideline: The Diagnosis, Management, and Prevention of Bronchiolitis. Pediatrics. 2014;134(5):e1474-e1502.
- Mazur NI, Martinón-Torres F, Baraldi E, et al. Lower respiratory tract infection caused by respiratory syncytial virus: current management and new therapeutics. The Lancet Respiratory Medicine. 2015;3(11):888-900.
- The IMpact-RSV Study Group. Palivizumab, a Humanized Respiratory Syncytial Virus Monoclonal Antibody, Reduces Hospitalization From Respiratory Syncytial Virus Infection in High-risk Infants. Pediatrics. 1998;102(3):531-537.
- Griffin MP, Yuan Y, Takas T, et al. Single-Dose Nirsevimab for Prevention of RSV in Preterm Infants. New England Journal of Medicine. 2020;383(5):415-425.
- Hammitt LL, Dagan R, Yuan Y, et al. Nirsevimab for Prevention of RSV in Healthy Late-Preterm and Term Infants (MELODY). New England Journal of Medicine. 2022;386(9):837-846.
- Drysdale SB, Cathie K, Flamein F, et al. Nirsevimab for Prevention of Hospitalizations Due to RSV in Infants (HARMONIE). New England Journal of Medicine. 2023;389(26):2425-2435.
- Kampmann B, Madhi SA, Munjal I, et al. Bivalent Prefusion F Vaccine in Pregnancy to Prevent RSV Illness in Infants (MATISSE). New England Journal of Medicine. 2023;388(16):1451-1464.
- Papi A, Ison MG, Langley JM, et al. Respiratory Syncytial Virus Prefusion F Protein Vaccine in Older Adults (AReSVi-006, Arexvy). New England Journal of Medicine. 2023;388(7):595-608.
- Walsh EE, Pérez Marc G, Zareba AM, et al. Efficacy and Safety of a Bivalent RSV Prefusion F Vaccine in Older Adults (RENOIR, Abrysvo). New England Journal of Medicine. 2023;388(16):1465-1477.
- Jones JM, Fleming-Dutra KE, Prill MM, et al. Use of Nirsevimab for the Prevention of Respiratory Syncytial Virus Disease Among Infants and Young Children: Recommendations of the ACIP — United States, 2023. MMWR. Morbidity and Mortality Weekly Report. 2023;72(34):920-925.
- Melgar M, Britton A, Roper LE, et al. Use of Respiratory Syncytial Virus Vaccines in Older Adults: Recommendations of the ACIP — United States, 2023. MMWR. Morbidity and Mortality Weekly Report. 2023;72(29):793-801.
- Kim HW, Canchola JG, Brandt CD, et al. Respiratory Syncytial Virus Disease in Infants Despite Prior Administration of Antigenic Inactivated Vaccine. American Journal of Epidemiology. 1969;89(4):422-434.
Research Papers
RSV research spans pediatrics, geriatrics, virology, vaccinology, and public health. The live PubMed searches below open the latest peer-reviewed studies on each facet of RSV — from infant bronchiolitis and the new immunizations to older-adult outcomes and basic virology. Each link runs a current search in a new tab.
- Respiratory syncytial virus
- RSV bronchiolitis in infants
- Nirsevimab for RSV prevention
- Maternal RSV vaccine in pregnancy
- RSV vaccine in older adults
- RSV hospitalization in the elderly
- Palivizumab in high-risk infants
- RSV pre-fusion F protein
- RSV bronchiolitis supportive treatment
- RSV and COPD exacerbations
- Global burden of RSV in children
- RSV, later wheezing, and asthma
Connections
- Bronchitis
- Pneumonia
- Asthma
- COPD
- Influenza
- Common Cold
- Ear Infections
- Heart Failure
- Shortness of Breath
- Chronic Cough
- Cystic Fibrosis
- Interstitial Lung Disease
- Pulmonology (All Lung Conditions)
- All Conditions
- Measles
- Whooping Cough